

Case Report
Excision of Posterior Cruciate Ligament Cyst Using Arthroscopic Two Portal Posteromedial Technique
1 District Hospital Bundi, Rajasthan, India.
2 Cosmopolitan Hospital, Thiruvananthapuram, Kerala, India.
3 Sri Siddhartha Medical College, Tumkuru, Karnataka, India.
4 Dubai Falcon Hospital, Dubai, UAE.
*Corresponding Author: Christudas Silvanose, Dubai Falcon Hospital, Dubai, UAE.
Citation: Jibin V Gladston, Srinivas R, Das S, Silvanose C. (2024). Excision of Posterior Cruciate Ligament Cyst Using Arthroscopic Two Portal Posteromedial Technique. Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers. 3(1):1-6. DOI: 10.59657/2992-9989.brs.24.017
Copyright: © 2024 Christudas Silvanose, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: October 19, 2023 | Accepted: November 03, 2023 | Published: January 02, 2024
Abstract
Posterior cruciate ligament (PCL) ganglion cysts are rare benign lesions of the knee that can cause pain and limit the range of motion. A 42-year-old female, presented with 2 years of pain in her right knee that was worse with kneeling, full extension, and strenuous activities. Physical examination revealed tenderness in the popliteal fossa and MRI confirmed the presence of a PCL ganglion cyst. A two-portal posteromedial technique is used to excise a PCL ganglion cyst that underwent arthroscopic surgery under combined spinal and epidural anesthesia. Two posteromedial portals were created, and the cyst was removed with a combination of a radiofrequency wand and shaver. The cyst wall was cleared from the PCL fibers and shiny white fibers of the posterior horn of the medial meniscus were preserved. The patient tolerated the procedure well, returned to her normal activities after 2 weeks, and was able to weight bear. This case report demonstrates the effectiveness of the two-portal posteromedial technique, which gives excellent visualization of the posterior compartment and allows for the safe and effective removal of the cyst without injury to the PCL or other structures.
Keywords: ganglion cyst; arthroscopy; posteromedial technique
Introduction
A posterior cruciate ligament (PCL) ganglion cyst is a benign fluid-filled sac that can develop in the knee joint which is seen in women in the third decade of life with a prevalence of < 0>
Case Summary
A 42-year-old woman without any known comorbidities has been experiencing a sharp pain accompanied by a clicking sensation in her right knee during terminal flexion, for the past two years. The discomfort intensifies when kneeling, fully extending the knee, or engaging in strenuous activities, but she finds relief when resting. There was no history of any traumatic or twisting injuries to the leg and during the physical examination, there were no visible swellings noted, and on palpation, no supra-patellar effusion was detected. However, tenderness was observed in the popliteal fossa area. Interestingly, there was no tenderness along the joint line. The patient reported experiencing pain specifically during terminal flexion.
All tests conducted to assess the posterior cruciate ligament (PCL) were negative, including McMurray's test, Lachman's test, anterior drawer test, posterior drawer test, Clarke's test, patellar compression test, and patellar lateral apprehension sign. Additionally, there were no indications of any distal neurovascular deficits during the examination. The knee's plain film radiographs did not reveal any abnormal findings related to the bones. However, a 3 Tesla magnetic resonance imaging (MRI) of the right knee showed the following findings.
A well-defined intra-articular encapsulated multilocular cyst measuring 1.5x1.8x2.3cm (anteroposterior, transverse, and craniocaudal dimensions) located in the posterior aspect of the knee, situated posterior to the posterior cruciate ligament (PCL). This cyst is seen to extend anteriorly, involving the distal posteromedial bundle fibers of the PCL and pushing them apart. It is limited posteriorly by an intact posterior joint capsule, indicating that it is likely a PCL ganglion cyst located within the joint space (Figures 1 and 2).
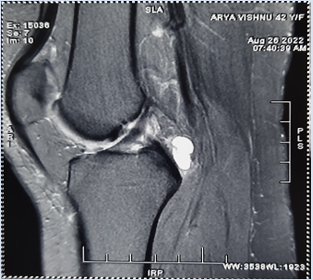
Figure 1: Lateral view of MRI of the right knee showing ganglion cyst in the PCL
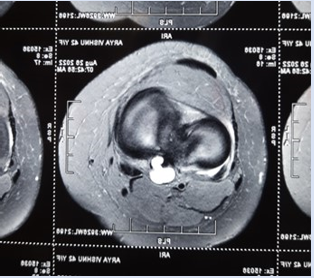
Figure 2: Axial view of MRI of right knee showing the PCL cyst.
Distal vertical limb of PCL posteromedial bundle shows linear ill-defined Proton density (PD) fat-saturation hyperintensity–suggestive of mucoid degeneration.
Additionally, a small loculated cyst was identified between the anterior cruciate ligament (ACL) and the PCL in the intercondylar region. This cyst did not appear to have any obvious communication with the PCL cyst.
The MRI also revealed a small area of partial thickness cartilage loss in the postero-central aspect of the patella, measuring 1.3 x 1.7mm.
The menisci, other ligaments, cartilage, bones, muscles, and tendons in the knee joint exhibit normal morphology and signal on the MRI.
In summary, the MRI findings indicate the presence of a well-defined PCL ganglion cyst within the knee joint, as well as a smaller cyst between the ACL and PCL. Moreover, there is a small area of cartilage loss on the patella. After explaining the pros and cons of the treatment, the patient elected to undergo arthroscopic cyst excision.
Surgical Procedure
The patient underwent arthroscopic PCL ganglion cyst decompression in the right knee, performed under combined spinal and epidural anesthesia. The patient was positioned supine on a well-padded operating room table without the use of a leg holder. Preoperative prophylactic antibiotics (Inj Cefotaxime 1.5g IV ATD and Inj Vancomycin 1g) were administered, and the right lower extremity was prepared and draped in a sterile manner.
The procedure began with the application of a tourniquet and an anesthesia evaluation indicated no instability in the knee. Diagnostic arthroscopic examination was conducted using anterolateral (AL) and anteromedial (AM) portals in the right knee (Figure 3) which visualized within the medial compartment, a flap tear at the medial aspect of the medial femoral condyle, near the root of the intercondylar notch. Additionally, fibrillation was found in the patellofemoral joint. Both menisci were intact, and the anterior cruciate ligament (ACL) was also found to be intact. The cyst was identified anterior to the PCL, and the scope was passed between the ACL and PCL to visualize the posterior compartments (Figure 4).
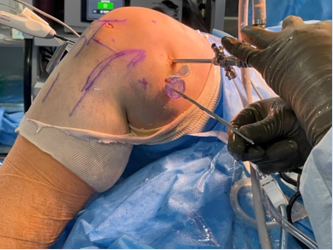
Figure 3: Right knee, knee flexed. Medial knee with skin markings to establish dual posteromedial portals.
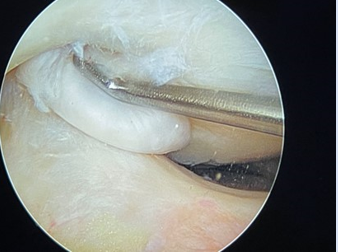
Figure 4: A well-defined intra-articular encapsulated multilocular cyst measuring 1.5 x 1.8 x 2.3cm (anteroposterior, transverse, and craniocaudal dimensions) located in the posterior aspect of the knee, situated posterior to the posterior cruciate ligament (PCL).
Two posteromedial portals were established to gain access to remove the cyst. A cystic mass with 1.5 x 1.8 x 2.3 cm was located behind the PCL, extending posteriorly and interiorly, covering the lower third of the PCL. A shaver and a rapid frequency wand (Arthrocare) were introduced through the posteromedial portals to excise the cyst. Care was taken to clear the cyst wall from the PCL fibers while preserving the shiny white fibers of the posterior horn of the medial meniscus.
A posterolateral portal was made under arthroscopic guidance and through this portal, a shaver and radiofrequency wand were used to remove the remaining part of the cyst. An additional cyst was found anterior to the PCL and was also removed using the shaver and radiofrequency tools. Throughout the procedure, the shaver blade was positioned facing anteriorly without suction.
After the cyst decompression, a negative result was obtained in the posterior drawer test, indicating stability. Additionally, stabilization was achieved for chondral lesions and fibrillation. Distal pulse was palpable, and limb saturation remained within normal limits, confirming adequate blood flow. The patient exhibited good tolerance to the procedure. Subsequently, the patient received detailed instructions regarding essential precautions, utilization of knee mobilizers, application of ice, elevation, and prescribed medications.
Discussion
Ganglion cysts have been well-documented on the dorsum of the wrist, their occurrence in the knees is infrequent, with posterior cruciate ligament (PCL) cysts being even rarer. The incidence of cysts arising from the posterior cruciate ligament (PCL) is lower compared to those originating from the anterior cruciate ligament. It's noteworthy that not all PCL cysts exhibit symptomatic manifestations. Nevertheless, in select cases, these cysts can have clinical significance, leading to knee pain and restricting the range of flexion [6].
The approach to treating PCL cysts is contingent upon factors such as cyst size, location, and symptomatology. When dealing with smaller, asymptomatic cysts, conservative strategies often take precedence, encompassing measures like rest, modifying activities, pain control, and targeted physical therapy to enhance surrounding muscle strength. Conversely, for larger or symptomatic cysts unresponsive to conservative approaches, an alternative entail draining the cyst through aspiration under ultrasound guidance to mitigate pressure and alleviate symptoms. It is essential to bear in mind that cyst recurrence is plausible following aspiration. In scenarios where the PCL demonstrates substantial injury or tearing, coupled with persistent symptoms or complications attributable to the cyst, a surgical course of action may be contemplated. This surgical intervention frequently employs arthroscopic techniques to concurrently address the PCL injury and excise or repair the cyst [7].
In contrast to the approach advocated by Bertrand Sonnery-Cottet, we have introduced a novel "two portal posteromedial technique," as delineated by Ahn J.H. and Ha, with the primary objective of minimizing the potential for cyst-related injury during the procedure [8,9]. Our surgical methodology initiates by inserting the scope through the trans-notch, affording visualization of the posterior compartment, encompassing structures like the adductor, gastrocnemius, and semi-membranous folds. To mitigate the risk of inadvertent harm, we meticulously introduce two 16 G cannula needles, exercising heightened caution to safeguard the saphenous vein and the sartorial branch of the saphenous nerve [9]. Within this technique, we deploy the superior posteromedial port for observational purposes, while the inferior posteromedial port serves as the operative access point. Upon shaver insertion, the trans-septal tissue is judiciously excised superior to the ganglionic mass, with careful attention to preserving the supreme genicular artery. As the shaver is directed into the posterolateral compartment, the shaver tip is strategically positioned against the deeper surface of the lateral skin, specifically anterior and superior to the short head of the biceps femoris, thereby ensuring a safe distance from the common peroneal nerve. Notably, the latter nerve is demarcated on the skin following meticulous preparation and draping to ensure its protection.
For a clear surgical pathway, the shaver blade's tip is then directed through a portal wound in the lateral skin. This is facilitated by a slotted cannula (half pipes) rail-roded over the shaver blade, enabling smooth withdrawal of the shaver blade into the joint. Because of these steps, two posteromedial portals and one posterolateral portal were established. The utilization of the posterolateral portal for shaver insertion, coupled with the high postero-medial portal for optimal visualization, synergistically enhances the clarity of the view into the posterior compartment. In addition, a Wissinger rod is introduced through the inferior postero-medial portal to exert controlled retraction of the posterior capsule in a posterior direction. Throughout the procedure, a meticulous blend of tools, including a radiofrequency wand (Arthrocare) and the shaver, is strategically employed to effectually excise the posterior cystic mass, ensuring the safeguarding of both the integrity of the PCL and the glossy white fibers of the medial meniscus root. In the subsequent anterior arthroscopy, we take care to apply a traction stitch on the cystic tissue anterior to the PCL, utilizing a knee scorpion (Arthrex) for traction. The cyst wall is gently peeled from the anterior aspect of the PCL using a Duck bell (Smith & Nephew) and shaver, with meticulous attention to preserving the PCL tissue.
Our "two portal posteromedial technique" differs significantly from the technique described by Sonnery-Cottet. Particularly, we emphasize the careful creation of the trans-septal portal with the aid of arthroscopic guidance, which has proven to be instrumental in providing excellent visualization of the entire posterior compartment, minimizing the risk of cyst injury during the procedure.
The benefits of employing the two posteromedial techniques are as follows:
- The meticulous creation of the trans-septal portal under arthroscopic guidance ensures meticulous precision, minimizing the potential for complications.
- Visualization of the cyst is optimized prior to the establishment of the trans-septal portal, enabling precise procedural planning and execution.
- The shaver can be adeptly utilized from both the posterolateral and posteromedial inferior ports, streamlining the process of cyst removal for enhanced efficiency.
- The potential risks and necessary precautions associated with the two posteromedial techniques are outlined below:
- Potential risk of inadvertent injury to the saphenous vein during the procedure.
- Need for vigilant care to prevent possible injury to the sartorial branch of the saphenous nerve.
- Consideration of the risk of fluid extravasation into the calf area, necessitating appropriate management strategies to avert complications.
- The essential considerations to uphold in this technique are as follows:
- Maintaining the knee in a 90-degree flexion position facilitates the posterior movement of popliteal neurovascular bundles, enhancing the surgeon's visual field and manoeuvring capabilities.
- Employing a switching stick via the inferior posteromedial portal contributes to supplementary retraction of the posterior capsule, thereby augmenting visualization and procedural access.
- Application of an elastic crape bandage, positioned approximately 10cm below the popliteal fossa, serves to mitigate the potential for fluid extravasation into the calf region, consequently minimizing the risk of complications.
Conclusion
This case report underscores the diagnosis and successful treatment of a symptomatic ganglion cyst involving the posterior cruciate ligament (PCL) in a 42-year-old female patient. The MRI findings revealed a distinct PCL ganglion cyst within the knee joint, coupled with a smaller cyst situated between the anterior cruciate ligament (ACL) and PCL, alongside a minor region of cartilage loss on the patella. The surgical intervention employed an arthroscopic approach for PCL ganglion cyst decompression, employing the "two portal posteromedial technique" yielded a successful outcome, ensuring the preservation of both the PCL and the shiny white fibers of the medial meniscus root. The patient's postoperative experience was positive, with stability restored and symptomatic relief achieved. While this technique offers distinct advantages, including precise visualization and effective cyst removal, it is imperative to acknowledge potential drawbacks, encompassing the risk of saphenous vein and sartorial branch of the saphenous nerve injury, as well as the potential for fluid extravasation into the calf.
The "two portal posteromedial technique" introduces a valuable avenue for managing PCL ganglion cysts, furnishing invaluable insights into optimal strategies for addressing these uncommon knee lesions. As with any surgical intervention, scrupulous attention to patient-specific variables and potential hazards is paramount to attaining favorable outcomes. Further investigation and research are warranted to compare diverse techniques and refine surgical approaches for the effective management of PCL ganglion cysts.
References
- Townsend CM, editor. (2022). Sabiston textbook of surgery: the biological basis of modern surgical practice. 21st edition. St. Louis, Missouri: Elsevier, 2147.
Publisher | Google Scholor - Andreozzi V, Monaco E, Conteduca F, Iorio R, Mazza D, Drogo P, et al. (2019). Diagnosis and Treatment of a Symptomatic Posterior Cruciate Ganglion Cyst in a Child with Autism. Case Rep Orthop, 1-6.
Publisher | Google Scholor - Feger J. (2020). Posterior cruciate ligament ganglion cyst. In: Radiopaedia.org [Internet]. Radiopaedia.
Publisher | Google Scholor - Durante JA. (2009). Ganglion cyst on the posterior cruciate ligament: a case report. J Can Chiropr Assoc, 53(4):334-338.
Publisher | Google Scholor - Telischak NA, Wu JS, Eisenberg RL. (2014). Cysts and cystic-appearing lesions of the knee: A pictorial essay. Indian J Radiol Imaging, 24(2):182-191.
Publisher | Google Scholor - Abreu FG, De Abreu GV, Pioger C, Franck F, Vieira TD, Bulle S, et al. (2020). Excision of a Posterior Cruciate Ligament Cyst Using an Arthroscopic Trans-septal Approach. Arthrosc Tech, 9(4):581-585.
Publisher | Google Scholor - Lee BK, Nam SW. (2011). Rupture of Posterior Cruciate Ligament: Diagnosis and Treatment Principles. Knee Surg Relat Res, 23(3):135-141.
Publisher | Google Scholor - Gousopoulos L, Hopper G, Levy Y, Grob C, Vieira TD, Sonnery-Cottet B. (2022). Easy Arthroscopic Transseptal Approach of the Knee. Video J Sports Med, 2(4):26350254221087290.
Publisher | Google Scholor - Christopher ZK, Dulle DL, Makovicka JL, Chhabra A. (2021). Dual–Posteromedial Portal Technique for Complex Arthroscopy in the Posterior Knee. Arthrosc Tech, 10(2):257-261.
Publisher | Google Scholor























