

Research Article
Understanding Tumor Lysis Syndrome: A Risk Factor Analysis in Lymphoma Patients Using Nationwide Database
1 Wyckoff Heights Medical Center, New York, United States.
2 Nuvance Health/Vassar Brothers Medical Center, New York, United States.
3 Lake Erie College of Osteopathic Medicine, Erie, Pennsylvania, United States.
4 State University of New York, Upstate Medical University, Syracuse, New York, United States.
5 University of Arizona College of Medicine Phoenix, Phoenix, Arizona, United States.
*Corresponding Author: Saad Javaid, Wyckoff Heights Medical Center, NY, United States.
Citation: Javaid S, Frasier K, Li V, Vinagolu-Baur J R, Huisman K, et al. (2024). Understanding Tumor Lysis Syndrome: A Risk Factor Analysis in Lymphoma Patients Using Nationwide Database. International Journal of Clinical and Molecular Oncology, BioRes Scientia publishers. 3(1):1-10. DOI: 10.59657/2993-0197.brs.24.008
Copyright: © 2024 Saad Javaid, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 09, 2024 | Accepted: January 26, 2024 | Published: February 08, 2024
Abstract
Introduction: Tumor lysis syndrome (TLS) is a severe and potentially fatal condition that frequently occurs in individuals with leukemia, but it may also affect those with high-grade lymphomas. Our study sought to carry out an extensive analysis of the risk factors associated with TLS in patients with lymphoma, with the objective of identifying critical indicators that substantially increase the likelihood of developing this medical crisis.
Materials and Methods: The National Inpatient Sample (NIS) for the years 2019 and 2020 was employed to identify patients who were admitted with a primary diagnosis of lymphoma of any type and a secondary diagnosis of TLS. The primary objective of the study was to investigate the risk factors that contribute to the increased incidence of TLS in patients with lymphoma, as well as the odds of mortality and the total cost of hospitalization for these patients. To account for confounding variables, multivariate regression analysis was utilized to calculate the desired outcomes.
Results: A total of 82,245 patients with lymphoma were hospitalized, of which 5,065 had a concurrent diagnosis of TLS. After adjusting for confounding variables, the odds of mortality were found to be increased in TLS patients (OR 3.3, 95% CI 2.7-4.02, P<0.001). Total charges were significantly higher in TLS patients (USD 149,262, 95%CI 127,644-170,881 without TLS and USD 242,730, 95% CI 196,533-288,927 with TLS, P<0.001). The length of stay was also increased in patients with TLS (10.17 days, 95% CI 9.38-10.96 without TLS and 13 days, 95% CI 11.75-14.17 with TLS, p<0.001). Fluid and electrolyte disorders (OR 3.63, 95% CI 3.1-4.25, P<0.001), malnutrition (OR 1.23, 95% CI 1.04-1.46, P=0.015), and heart failure (OR 1.24, 95% CI 1.01-1.57, P=0.006) demonstrated a higher risk of association with TLS. TLS patients were also more likely to have palliative care involvement (OR 1.61, 95% CI 1.35-1.92, P<0.001). Conversely, major depressive disorder (OR 0.62, 95% CI 0.48-0.79, P<0.001) and hematopoietic stem cell transplant (OR 0.1, 95% CI 0.05-0.18, P<0.001) were associated with a decreased risk of TLS in patients with lymphoma.
Conclusions: The study found that in patients with lymphoma, TLS was associated with increased mortality risk, longer hospital stays, and higher treatment costs. Furthermore, fluid and electrolyte disorders, malnutrition, and heart failure were identified as risk factors for developing TLS, while major depressive disorder and hematopoietic stem cell transplant were associated with a decreased likelihood of TLS occurrence.
Keywords: tumor lysis syndrome; lymphoma patients; palliative care involvement; fluid and electrolyte disorders
Introduction
Lymphoma is a type of cancer of the lymphatic system, which includes the lymph nodes, spleen, thymus gland, and bone marrow. Lymphomas arise from two types of white blood cells: B lymphocytes (B cells) and T lymphocytes (T cells). Cancerous B Cells and T Cells circulate to different parts of the body, where they accumulate and form a tumor. There are more than 70 types of lymphoma, however they are broadly categorized as 1) Hodgkin lymphoma (HL) and 2) non-Hodgkin lymphoma (NHL) [1,2]. According to American Cancer Society estimates for 2023, there are about 8,830 new cases of HL and 900 deaths related to the cancer, with a 5-year relative survival rate approaching 89%. Conversely, there are approximately 80,550 new cases of NHL detected in the United States annually, with 20,180 deaths from cancer [3]. NHL is more common than HL, comprising 4% of all cancers [4,5].
Tumor Lysis Syndrome (TLS) is an oncologic emergency that results when a large number of cancer cells are lysed within a short period of time, releasing their contents into the bloodstream. TLS often occurs after chemotherapy or other cancer treatments such as steroids, hormonal therapy, targeted therapy, or radiation therapy. As cancer cells break down rapidly, the levels of their cell contents in the blood rise faster than the kidneys can discard them. This results in elevated levels of uric acid, potassium, and phosphorus, which can lead to electrolyte imbalances such as hypocalcemia, hyperkalemia, and hyperphosphatemia. This is evident in the case of excess phosphorus, which “sops up” calcium, thereby reducing levels of calcium in the blood. Changes in electrolyte balance can impact several organs in the body, especially the kidneys, gastrointestinal tract, muscles, heart, and brain [6]. Hyperkalemia can cause cardiac arrest from arrhythmia, and complications from hypocalcemia include arrhythmia, tetany, seizures, and even death, to name a few complications [7].
Tumor lysis syndrome is common in patients diagnosed with leukemia with high white blood cell (WBC) count; however, it is also seen in high-grade lymphomas, particularly post-initiation of aggressive chemotherapy [8]. The risk of developing TLS varies according to tumor type. Of note, the highest degree of risk of TLS in cancers of the lymphatic system occurs in Burkitt’s lymphoma, high-grade non-Hodgkin lymphoma, and lymphoblastic lymphoma. A moderate risk of TLS is seen in low-grade lymphoma that is treated with chemotherapy, radiation, or corticosteroids, and a low risk of TLS is associated with low-grade lymphoma treated with interferon [9,10]. In a previously published query of the National Inpatient Sample, the most common malignancy associated with tumor lysis syndrome is non-Hodgkin lymphoma (30%) in addition to other malignancies such as solid tumors, acute myeloid leukemia, and acute lymphocytic leukemia at 20%, 19% and 13% respectively. According to the study’s findings, in-hospital mortality was approximately 21% [11].
A thorough examination of the existing literature unveils an abundance of studies focused on TLS in leukemia patients. Nevertheless, there is a conspicuous scarcity of comprehensive information regarding the pathogenesis and intricate nuances of TLS in lymphoma patients across a variety of subcategories. To bridge this gap, our study is designed to offer a more in-depth comprehension of the incidence, risk factors, and clinical outcomes for hospitalized lymphoma patients who experience TLS during their hospitalization.
Methods and Materials
Data design and source
This research was based on the extensive National Inpatient Sample (NIS), which spans the years 2019-2020 and serves as a robust repository encompassing inpatient care details from a broad spectrum of healthcare facilities in the United States. With data aggregated from over 21 million hospital admissions annually and including information from 46 states and the District of Columbia, the NIS offers an impressive representation covering approximately 98% of the U.S. population. It is important to note that entries related to rehabilitation and federal institutions like Veterans Affairs hospitals are excluded from this comprehensive compilation. Administered by the Agency for Healthcare Research and Quality through its Healthcare Costs and Utilization Project, the NIS provides an exceptionally large sample size conducive for conducting in-depth analyses of various healthcare phenomena, even those associated with rare diseases.
Study population
Our research entailed a comprehensive analysis of discharge data sourced from the National Inpatient Sample database for adults aged 18 and above who had been diagnosed with lymphoma. The International Classification of Diseases, Tenth Revision, Clinical Modification/Procedure Coding System (ICD-10-CM/PCS) was employed as the coding scheme for this investigation. Subsequently, we meticulously classified the patients into those with and without tumor lysis syndrome.
Study variables and outcomes
The study aimed to compare the effects of tumor lysis syndrome on outcomes in hospitalized patients diagnosed with lymphoma. The primary endpoint was inpatient mortality rates among patients with lymphoma with and without tumor lysis syndrome. The secondary outcomes included length of stay, total cost of hospitalization, and odds of association of different risk factors with TLS.
Statistical analysis
The representation of categorical data was through percentage; conversely, mean values and standard deviations were used to characterize continuous variables. To compare categorical variables among different groups, Pearson’s chi-square test or Fisher’s exact test was employed, whereas the student’s t-test was used to evaluate continuous variables. Both univariate and multivariate analyses were performed to determine the associations between tumor lysis syndrome and critical parameters, such as in-hospital mortality, prolonged length of stay, total treatment cost, and the risk factors. The Stata 17 software (College Station, TX, USA) was utilized to conduct all statistical analyses, which provided valuable insights that significantly contributed to answering research questions and hypotheses, ultimately enhancing the overall quality of the study.
Results
In the year 2019-2020, a total of 82,245 patients with lymphoma were admitted to hospital; of these, 5,065 patients were diagnosed with TLS, while 77,180 were not. The mean age of patients with TLS was 62.18±17.90 years, compared to 61.57±18.62 years for those without TLS, with a statistically significant difference of P less than 0.001. A greater proportion of male patients had TLS compared to females (63.38% vs 58.51%, P=0.002). A higher proportion of patients with TLS had a Charlson comorbidity index of ≥3 (64.56% vs 57.07%, P=0.001), while fewer patients had a Charlson In the year 2019-2020, a total of 82,245 patients with lymphoma were admitted to hospital; of these, 5,065 patients were diagnosed with TLS, while 77,180 were not. The mean age of patients with TLS was 62.18±17.90 years, compared to 61.57±18.62 years for those without TLS, with a statistically significant difference of P less than 0.001. A greater proportion of male patients had TLS compared to females (63.38% vs 58.51%, P=0.002). A higher proportion of patients with TLS had a Charlson comorbidity index of ≥3 (64.56% vs 57.07%, P=0.001), while fewer patients had a Charlson comorbidity index of 2 or less (34.16% vs 41.46%, P=0.001). Patients with TLS were found to have fewer cases of hypertension (30.9% vs 35.88%, P=0.001) and a higher prevalence of CKD. Fluid and electrolyte disorders were also more prevalent in patients with TLS (68.21% vs 36.67%, P less than 0.001). A higher percentage of patients with TLS had malnutrition (28.73% vs 19.57%, P less than 0.001), heart failure (14.61% vs 9.44%, P less than 0.001), and required more palliative care involvement (18.36% vs 10.09%, P less than 0.001). However, fewer patients with TLS had depression (8.29% vs 11.13%, P=0.005); fewer patients with TLS underwent hematopoietic stem cell transplant (1.48% vs 9.89%, P less than 0.001); and a greater proportion underwent chemotherapy (1.88% vs 1.13%, P=0.03). A higher proportion of patients with TLS were discharged to their homes with home care (30.31% vs 23.37%) and skilled nursing facilities (7.17% vs 4.57%). In contrast, a greater proportion of patients without TLS were discharged to homes (71.3% vs 61.79%, P less than 0.001) (Table 1).
Table 1: Comparison of baseline characteristics of Lymphoma patients with and without TLS
| Lymphoma without TLS | Lymphoma with TLS | P-value | |
| No. of patients | 77180 | 5065 | |
| Patient Characteristics | |||
| Gender (%) | 0.002 | ||
| Male | 45158 (58.51) | 3210 (63.38) | |
| Female | 32022 (41.49) | 1855 (36.62) | |
| Age | |||
| Mean Age (SD) | 61.57(18.62) | 62.18(17.90) | less than 0.001 |
| Age Distribution (%) | 0.010 | ||
| 18-35 | 6869 (8.9) | 342 (6.75) | |
| 36-45 | 5156 (6.68) | 249 (4.91) | |
| 46-64 | 23972 (31.06) | 1673 (33.03) | |
| >65 | 41168 (53.34) | 2802 (55.32) | |
| Race (%) | 0.781 | ||
| White | 56295 (72.94) | 3707 (73.19) | |
| Black | 8104 (10.5) | 517 (10.2) | |
| Hispanic | 9987 (12.94) | 629 (12.41) | |
| Other | 2794 (3.62) | 213 (4.21) | |
| Median household income national quartile for patient zip code (%) | 0.297 | ||
| $1-$49,999 | 18948 (24.55) | 1121 (22.13) | |
| $50,000-$64,999 | 18732 (24.27) | 1325 (26.16) | |
| $65,000-$85,999 | 19557 (25.34) | 1284 (25.35) | |
| >$86,000 | 19943 (25.84) | 1335 (26.36) | |
| Charlson comorbidity index (%) | 0.0001 | ||
| 0 | 733 (0.95) | 45 (0.89) | |
| 1 | 401 (0.52) | 20 (0.39) | |
| 2 | 31999 (41.46) | 1730 (34.16) | |
| 3 or more | 44047 (57.07) | 3270 (64.56) | |
| Insurance Provider (%) | 0.180 | ||
| Medicare | 39022 (50.56) | 2659 (52.5) | |
| Medicaid | 9694 (12.56) | 631 (12.46) | |
| Private | 25855 (33.5) | 1666 (32.89) | |
| Uninsured | 2609 (3.38) | 0 (0) | |
| Comorbidities (%) | |||
| Hypertension | 27692 (35.88) | 1565 (30.9) | 0.001 |
| Diabetes Mellitus | 14533 (18.83) | 925 (18.26) | 0.669 |
| Chronic Kidney Disease | |||
| CKD2 | 764 (0.99) | 55 (1.09) | 0.769 |
| CKD3 | 4368 (5.66) | 380 (7.5) | 0.015 |
| CKD4 | 756 (0.98) | 110 (2.17) | less than 0.001 |
| CKD5 | 85 (0.11) | 15 (0.3) | 0.099 |
| CKD Unspecified | 2748 (3.56) | 370 (7.31) | less than 0.001 |
| ESRD | 795 (1.03) | 65 (1.28) | 0.448 |
| Hyperlipidemia (HLD) | 22012 (28.52) | 1435 (28.33) | 0.898 |
| Fluid and Electrolyte Disorders | 28302 (36.67) | 3455 (68.21) | less than 0.001 |
| Obesity | 8667 (11.23) | 575 (11.35) | 0.909 |
| Constipation | 13352 (17.3) | 955 (18.85) | 0.229 |
| Palliative care | 7787 (10.09) | 930 (18.36) | less than 0.001 |
| Malnutrition | 15104 (19.57) | 1455 (28.73) | less than 0.001 |
| Coronary artery disease | 10172 (13.18) | 635 (12.54) | 0.547 |
| Heart Failure | 7286 (9.44) | 740 (14.61) | less than 0.001 |
| Major depressive disorder | 8590 (11.13) | 420 (8.29) | 0.005 |
| Valvular Heart Disease | 2393 (3.1) | 185 (3.65) | 0.311 |
| Smoking | 448 (0.58) | 25 (0.49) | 0.721 |
| Opioid use disorder | 671 (0.87) | 35 (0.69) | 0.549 |
| Cocaine Use | 254 (0.3) | 5(0.009) | 0.2044 |
| COPD | 5742 (7.44) | 390 (7.7) | 0.76 |
| Hematopoietic stem cell Transplant | 7633 (9.89) | 75 (1.48) | less than 0.001 |
| Chemotherapy | 872 (1.13) | 95 (1.88) | 0.03 |
| CAR-T Therapy | 1227 (1.59) | 125 (2.47) | 0.1841 |
| Discharge Disposition (%) | less than 0.001 | ||
| Home | 55029 (71.3) | 3130 (61.79) | |
| Home with home health | 18037 (23.37) | 1535 (30.31) | |
| Skilled nursing facility | 3527 (4.57) | 363 (7.17) | |
| Against Medical Advice | 579 (0.75) | 37 (0.73) | |
| Hospital characteristics (%) | |||
| Bed size of hospital (STRATA) | 0.010 | ||
| Small | 10728 (13.9) | 565 (11.15) | |
| Medium | 17211 (22.3) | 1020 (20.14) | |
| Large | 49202 (63.75) | 3480 (68.71) | |
| Hospital location | 0.031 | ||
| Rural | 2439 (3.16) | 100 (1.97) | |
| Urban | 74741 (96.84) | 4965 (98.03) | |
| Region of hospital | 0.02 | ||
| Northeast | 16208 (21) | 1095 (21.62) | |
| Midwest | 16856 (21.84) | 1200 (23.69) | |
| South | 28263 (36.62) | 1600 (31.59) | |
| West | 15853 (20.54) | 1170 (23.1) | |
The mortality rate for patients without TLS was 4.7%, while for patients with TLS, it was 17.7%. After adjusting for confounding factors, the odds of mortality were significantly higher in patients with TLS (OR 3.3, 95% CI 2.7-4.02, P less than 0.001) (Table2). Furthermore, the length of stay was longer for lymphoma patients who developed TLS (10.17 days [95% CI 9.38-10.96] without TLS vs. 13 days [95% CI 11.75-14.17] with TLS), P less than 0.001. The total cost of hospitalization was also greater in patients with TLS ($14,9262 [95% CI $127644- $170881] without TLS, $24,2730 [95% CI $19,6533- $28,8927] with TLS), P less than 0.001.(Table 3). Fig 1 and 2 demonstrate the adjusted predicted margins of Length of stay and total cost of hospitalization in lymphoma patients with and without TLS
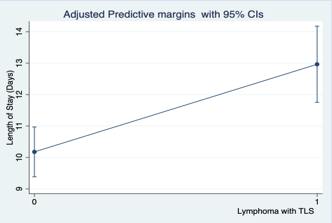
Figure 1
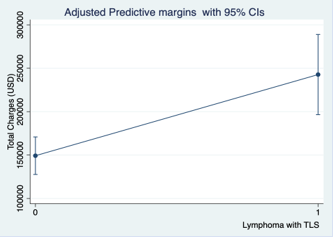
Figure 2
Table 2: Odds ratio of Mortality in Lymphoma patients with TLS
| CRS | Rate (%) | Odds Ratio | Confidence Interval | P- value | |
| Lower limit | Upper limit | ||||
| No | 4.7 | Reference | |||
| Yes | 17.7 | 3.3 | 2.7 | 4.02 | less than 0.001 |
Table 3: Length of stay and total cost of treatment in Lymphoma patients with and without TLS
| Lymphoma without TLS | Lymphoma with TLS | P-value | |
| LOS Days (Adjusted) | 10.17(95%CI 9.38 - 10.96) | 13 (95%CI 11.75- 14.17) | P less than 0.001 |
| Total Charges USD (Adjusted) | 149262 (95%CI 127644- 170881) | 242730 (95%CI 196533- 288927) | P less than 0.001 |
The association of several risk factors with the development of TLS was calculated. Females were less likely to develop TLS compared to male patients (OR 0.77, 95% CI 0.67-0.9, P=0.001). Patients with fluid and electrolyte disorders (OR 3.63, 95% CI 3.1-4.25, P less than 0.001), malnutrition (OR 1.23, 95% CI 1.04-1.46, P=0.015), and heart failure (OR 1.24, 95% CI 1.01-1.57, P=0.006) were more likely to develop TLS compared to those without these conditions. Additionally, patients with TLS had higher odds of palliative care involvement (OR 1.61, 95% CI 1.35-1.92, P less than 0.001). Those with major depressive disorder (OR 0.62, 95% CI 0.48-0.79, P less than 0.001) and patients who had undergone hematopoietic stem cell transplant (OR 0.1, 95% CI 0.05-0.18, P less than 0.001) had significantly lower odds of developing TLS. However, no significant difference was observed in the development of TLS between patients who underwent chemotherapy and those who underwent CAR-T cellular therapy (Table 4).
Table 4: Odds ratios of association of different risk factors with TLS in Lymphoma patients
| Variables | Odds Ratio | Confidence Interval | P- value | |
| Lower limit | Upper limit | |||
| Gender (%) | ||||
| Male | Reference | |||
| Female | 0.77 | 0.67 | 0.9 | 0.001 |
| Age Distribution (%) | ||||
| 18-35 | Reference | |||
| 36-45 | 0.94 | 0.63 | 1.4 | 0.783 |
| 46-64 | 1.21 | 0.89 | 1.64 | 0.202 |
| >65 | 1.13 | 0.79 | 1.6 | 0.483 |
| Race (%) | ||||
| White | Reference | |||
| Black | 0.99 | 0.77 | 1.28 | 0.974 |
| Hispanic | 0.96 | 0.76 | 1.23 | 0.804 |
| Other | 1.2 | 0.84 | 1.71 | 0.314 |
| Median household income national quartile for patient zip code (%) | ||||
| $1-$49,999 | Reference | |||
| $50,000-$64,999 | 1.14 | 0.92 | 1.41 | 0.225 |
| $65,000-$85,999 | 1.01 | 0.83 | 1.24 | 0.864 |
| >$86,000 | 1.03 | 0.83 | 1.27 | 0.775 |
| Charlson comorbidity index (%) | ||||
| Reference | ||||
| 1 | 0.77 | 0.19 | 3.01 | 0.714 |
| 2 | 0.95 | 0.45 | 2.01 | 0.901 |
| 3 or more | 1.13 | 0.54 | 2.36 | 0.742 |
| Insurance Provider (%) | ||||
| Medicare | Reference | |||
| Medicaid | 1.07 | 0.79 | 1.44 | 0.65 |
| Private | 1.07 | 0.85 | 1.34 | 0.526 |
| Uninsured | 0.67 | 0.39 | 1.15 | 0.149 |
| Comorbidities (%) | ||||
| Hypertension | 0.85 | 0.72 | 1.01 | 0.072 |
| Diabetes Mellitus | 0.88 | 0.72 | 1.08 | 0.229 |
| Hyperlipidemia (HLD) | 0.94 | 0.8 | 1.11 | 0.503 |
| Fluid and Electrolyte Disorders | 3.63 | 3.1 | 4.25 | less than 0.001 |
| Obesity | 0.503 | 0.79 | 1.23 | 0.937 |
| Palliative care | 1.61 | 1.35 | 1.92 | less than 0.001 |
| Malnutrition | 1.23 | 1.04 | 1.46 | 0.015 |
| Coronary artery disease | 0.86 | 0.69 | 1.06 | 0.177 |
| Heart Failure | 1.24 | 1.01 | 1.57 | 0.006 |
| Major depressive disorder | 0.62 | 0.48 | 0.79 | less than 0.001 |
| Smoking | 1.04 | 0.43 | 2.49 | 0.916 |
| Opioid use disorder | 0.98 | 0.46 | 2.08 | 0.974 |
| Cocaine use | 0.31 | 0.04 | 2.39 | 0.263 |
| Valvular Heart Disease | 1.08 | 0.76 | 1.53 | 0.648 |
| COPD | 0.93 | 0.71 | 1.22 | 0.631 |
| Hematopoietic stem cell Transplant | 0.1 | 0.05 | 0.18 | less than 0.001 |
| Chemotherapy | 1.64 | 0.92 | 2.91 | 0.09 |
| CAR-T Therapy | 1.62 | 0.78 | 3.37 | 0.19 |
Discussion
In our comprehensive analysis of 82,245 lymphoma patients admitted to the hospital, 5,065 were diagnosed with TLS concurrently. This study has yielded crucial findings that illuminate the significant impact of TLS on patient outcomes and healthcare resources, as well as the risk factors associated with TLS development in this specific group of hematological cancer patients. Our research demonstrated that TLS significantly increased the risk of mortality in lymphoma patients, with an odds ratio of 3.3, indicating a more than threefold increase compared to those without TLS. Additionally, the presence of TLS is correlated with significantly longer hospital stays and substantially higher treatment costs, reflecting the intensive care and resources required for these patients. This can be explained by the multiple metabolic complications associated with TLS. According to Cairo et al., their review of literature provides a comprehensive explanation of the pathophysiological mechanisms and potential complications linked to TLS, including electrolyte disorders and the risk of acute kidney injury. These factors further increase the mortality risk for patients affected by TLS. Therefore, understanding and monitoring the metabolic abnormalities associated with TLS becomes crucial to prevent and manage potential complications, improve patient outcomes, and reduce mortality rates [12].
Our study delved into the specific risk factors that could lead to the development of TLS. We primarily focused on this aspect and did not explore the broader spectrum of adverse in-hospital outcomes beyond mortality and resource utilization within this subset of lymphoma patients. Gangani K et al. conducted a retrospective study using NIS data from 2009-2014 to explore the outcomes of 9,034 patients with arrhythmia and a concurrent diagnosis of TLS, out of which 37,861 patients had been hospitalized. The findings revealed that the coexistence of arrhythmia and TLS was linked to higher odds of mortality and increased resource utilization [13,14]. Notably, our research differed slightly as we specifically focused on evaluating the independent impact of TLS on lymphoma patients; however, it still evidenced an association between TLS and adverse outcomes. Our research revealed that TLS patients incur an average additional cost of $242,730, reflecting the extensive resources required for their management. This significant rise in costs and the length of stay can be attributed to the need for intensive monitoring, specialized treatments, and potential interventions for organ dysfunction and other complications associated with TLS [12]. Additionally, the extended length of hospital stays, as previously discussed, contributes substantially to these increased costs. This is corroborated by findings from Burudpakdee et al., who reported that peripheral T-cell lymphoma patients experienced considerably higher average monthly healthcare-associated costs, with 32.2% of these expenses stemming mainly from hospitalizations [15]. Additionally, a study by Rogers et al indicated that TLS among patients with chronic lymphocytic leukemia/small lymphocytic lymphoma was associated with an additional cost of $3,062 per-patient-per-month, predominantly due to increased inpatient expenses [16]. Therefore, the economic burden of hospitalization for lymphoma patients with TLS highlights the need for effective preventive strategies and cost-efficient management protocols to mitigate these expenses and alleviate the economic impact on both the healthcare system and the affected individuals.
The association between malnutrition and an increased risk of TLS in lymphoma patients is a critical connection that merits attention in clinical practice as evident from our study results. Malnutrition, characterized by inadequate intake of essential nutrients, can lead to a compromised physiological state, affecting various organ functions and the overall immune response [17]. The rapid cell turnover in lymphoma often precipitates profound metabolic disturbances, further compounding the elevated metabolic strain associated with TLS in malnourished patients [12]. Hebuterne et al.’s investigation into the prevalence of malnutrition among cancer patients found that 48.9% of those with leukemia/lymphoma were malnourished [18]. Although a study by Mansoor et al focuses on the pediatric population, their data demonstrating malnutrition and tumor lysis syndrome as significant risk factors in the acute mortality of mature B cell non-Hodgkin lymphoma concur with our results [19]. Furthermore, malnourished patients often have reduced muscle mass, which has been linked to dysregulated phosphate metabolism and phosphate toxicity [20]. This factor, combined with the hyperphosphatemia caused by tumor cell lysis, further escalates both the risk and severity of TLS in lymphoma patients. Recognizing malnutrition as a risk factor is imperative for healthcare providers, as it underscores the importance of nutritional assessment and support as part of the comprehensive care for lymphoma patients, particularly in relation to TLS.
Our study showed that heart failure is considered as a significant risk factor of LS. It can be due primarily to its impact on renal function and fluid balance, both of which are crucial in the pathophysiology of TLS. The compromised cardiac output and renal perfusion characteristic of heart failure leads to reduced clearance of uric acid and other metabolites, exacerbating electrolyte imbalances and renal complications often seen in TLS [12,26]. Impaired renal function is often secondary to heart failure, emphasizing the importance of our findings. This cardiorenal interplay becomes more evident with Gangani et al.’s retrospective study, revealing that 64.7% of TLS-related admissions and two-thirds of hospitalized arrhythmic patients involved fluid and electrolyte disorders [14]. Moreover, Rampello et al. highlight the complexities in fluid management for TLS patients with heart failure due to their increased susceptibility to fluid overload, potentially leading to worsened heart failure and acute kidney injury [21]. Thus, the presence of heart failure in lymphoma patients necessitates careful, tailored management strategies to mitigate the risk of developing TLS and to manage it effectively should it occur.
This association between TLS and heart failure holds substantial significance for clinicians, given the well-documented increased incidence of heart failure among lymphoma patients. This correlation is linked to the use of anthracycline-based chemotherapy agents, such as doxorubicin, which are commonly employed in the treatment of certain cancers, including lymphomas. Childhood cancer survivors treated with anthracyclines have demonstrated a striking 5- to 15-fold increased risk for developing heart failure [22]. Palliative care aims to enhance the quality of life of patients experiencing the burden of illness, encompassing physical, psychological, and spiritual aspects. Intriguingly, our analysis found that patients who experienced TLS were more likely to have palliative care involvement. While the reasons for this association are likely multifactorial, one plausible explanation lies in the fact that TLS risk factors such as heart failure or electrolyte imbalances stemming from kidney disease, as well as malnutrition and frailty, are among the same conditions that are commonly associated with the need for palliative care [23]. This unique association has not been thoroughly explored in existing literature and requires further investigation. Our study aimed to provide initial insights, but there is a clear need for additional research and prospective studies to fully understand its implications.
In a longitudinal study by Oerlemans et al., the rate and duration of anxiety and depression in lymphoma patients was investigated [24]. Resulting data from this study found an increased rate and duration of depression and anxiety in patients with lymphoma. Interestingly, of these patients those with comorbidity and lower education reported higher rates, according to their study. Conversely, the results of our study demonstrated a decreased association of depression with TLS in lymphoma patients. A possible explanation for this phenomenon could be that patients with TLS often belong to the higher risk category and are more vulnerable to underlying depression and anxiety. They may also be receiving effective medication, which contributes to the management of their depression and other psychiatric manifestations associated with debilitating hematological conditions. However, considering the varying results of these two studies, the need to understand what comorbidities are present and their effect on adverse outcomes, provides the need for further investigation.
Tumor lysis syndrome is a phenomenon that occurs when rapid cell death causes the release of intracellular contents, particularly electrolytes, resulting in life threatening complications [7]. One such cause of rapid cell death is the use of chemotherapeutic intervention [7]. Stem cell transplant therapy can be implemented as first line therapy, second line, and/or adjunctive therapy among other options, and continued research remains necessary to determine best treatment plans with the incorporation of monoclonal antibodies [25]. The results of our study demonstrated that in patients with lymphoma who received hematopoietic cell transplant therapy, the odds of developing TLS was significantly lower. There might be a possible explanation for the reduced association of HSCT with TLS, as patients who have undergone HSCT often display poor responses to initial cytotoxic chemotherapy. Additionally, they may be refractory to treatment or in the relapse phase after initial therapy. This could lead to a decrease in the frequency of cytotoxic chemotherapy following HSCT, which ultimately results in decreased association with TLS. However, further research is needed to fully understand the relationship between HSCT and TLS risk reduction.
It should also be emphasized that retrospective analyses using databases have inherent limitations and therefore, these findings should be approached with caution. Relying on ICD-10-CM/PCS codes for diagnoses in this study has the potential to be inaccurate due to the absence of corresponding laboratory data in the NIS database. Other essential clinical information, such as symptoms, medications, and functional capacity, were inaccessible, which made it challenging to rule out any inaccuracies or coding related biases introduced by healthcare providers. These biases could have influenced the diagnostic accuracy. Additionally, the NIS database maintains hospitalization records per admission rather than per person, meaning that a single individual can be counted multiple times if admitted to different hospitals or experienced multiple hospital stays during the study period. As a result, analyzing secondary diagnoses in relation to each specific admission is hindered by the timing and sequencing information being inaccessible due to this methodology issue. Lastly, it is important to acknowledge that selection bias is also a potential concern with any retrospective analysis. Despite conducting thorough multivariate regression analysis aimed at mitigating this risk and ensuring accuracy, there remains room for further exploration through prospective trials for validation purposes.
Conclusion
The study findings underscore the severe consequences associated with TLS, revealing a significantly elevated mortality risk and prolonged hospital stays for those affected. Moreover, the economic burden of TLS is evident through substantially increased treatment costs, emphasizing the need for effective preventive strategies and management approaches. The identified risk factors, including fluid and electrolyte disorders, malnutrition, and heart failure, provide valuable insights into potential targets for intervention and risk mitigation. Notably, the study found decreased associations of major depressive disorder and hematopoietic stem cell transplant, offering avenues for further exploration in understanding the nuanced dynamics of TLS development in patients with lymphoma. These findings contribute significantly to the clinical understanding of TLS in the context of lymphoma, guiding healthcare practitioners toward more informed risk assessment and tailored management strategies.
References
- Memorial Sloan Kettering Cancer Center. (2023). Types of lymphoma.
Publisher | Google Scholor - Mayo Clinic. (2022, December 14). Lymphoma - Symptoms and causes.
Publisher | Google Scholor - American Cancer Society. (2023). Hodgkin lymphoma statistics | How common is Hodgkin disease?
Publisher | Google Scholor - Küppers R & Hansmann M. L. (2005). The Hodgkin and Reed/Sternberg cell. The international journal of biochemistry & cell biology, 37(3):511-517.
Publisher | Google Scholor - National Cancer Institute. (2019). Vaccine to treat lymphoma advancing in trials.
Publisher | Google Scholor - Gupta A & Moore J. A. (2018). Tumor lysis syndrome. JAMA Oncology, 4(6):895.
Publisher | Google Scholor - Adeyinka A, Bashir K. Tumor Lysis Syndrome. (2022). In: Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls Publishing; 2023 Jan.
Publisher | Google Scholor - Williams S. M & Killeen A. A. (2019). Tumor Lysis Syndrome. Archives of pathology & laboratory medicine, 143(3):386-393.
Publisher | Google Scholor - Jeha S. (2001). Tumor lysis syndrome. Seminars in hematology, 38(4-10):4-8.
Publisher | Google Scholor - Koontz, S. E. (2008, March 10). A review of tumor lysis syndrome. U.S. Pharmacist – The Leading Journal in Pharmacy.
Publisher | Google Scholor - Stephanos K & Picard L. (2018). Pediatric Oncologic Emergencies. Emergency medicine clinics of North America, 36(3):527-535.
Publisher | Google Scholor - Cairo M. S & Bishop M. (2004). Tumour lysis syndrome: new therapeutic strategies and classification. British journal of haematology, 127(1):3-11.
Publisher | Google Scholor - Ghimire C, Baral N, Mathew SM, Vinjam T, Acharya S, Bashyal KP, Karki S, Koduru U, Christy J, Kunadi A. (2022). Outcomes of Tumor Lysis Syndrome in Hospitalized Patients: A Retrospective Cohort Study from National Inpatient Sample 2016-2019. Blood, 140(1):11741.
Publisher | Google Scholor - Gangani K, Fong H. K, Faisaluddin M, Lodhi M. U, Manaktala P, Sadolikar A, Shah V, Gandhi Z, Abu Hassan F, Savani S, Doshi R & Desai R. (2020). Arrhythmia in tumor lysis syndrome and associated in-hospital mortality: A nationwide inpatient analysis. Journal of arrhythmia, 37(1):121-127.
Publisher | Google Scholor - Burudpakdee C, Lin H. M, Wang W, Seetasith A, Zhu Y, Bonthapally V & Carson K. R. (2016). Clinical and economic burden of peripheral T-cell lymphoma in commercially insured patients in the United States: findings using real-world claims data. Journal of medical economics, 19(10):965-972.
Publisher | Google Scholor - Rogers K. A, Lu X, Emond B, Côté-Sergent A, Kinkead F, Lafeuille M. H, Lefebvre P & Huang Q. (2022). Clinical and economic burden of tumor lysis syndrome among patients with chronic lymphocytic leukemia/small lymphocytic lymphoma: A real-world US retrospective study. Journal of managed care & specialty pharmacy, 28(9):1033-1045.
Publisher | Google Scholor - Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, Bozzetti F, Fearon K, Hütterer E, Isenring E, Kaasa S, Krznaric Z, Laird B, Larsson M, Laviano A, Mühlebach S, Muscaritoli M, Oldervoll L, Ravasco P, Solheim T, Strasser F, … Preiser J. C. (2017). ESPEN guidelines on nutrition in cancer patients. Clinical nutrition (Edinburgh, Scotland), 36(1):11-48.
Publisher | Google Scholor - Hébuterne X, Lemarié E, Michallet M, de Montreuil C. B, Schneider S. M & Goldwasser F. (2014). Prevalence of malnutrition and current use of nutrition support in patients with cancer. JPEN. Journal of parenteral and enteral nutrition, 38(2):196-204.
Publisher | Google Scholor - Mansoor R, Saeed H, Wali R. M, Rehman P & Abubakar M. (2019). Malnutrition, Sepsis, and Tumor Lysis Syndrome Are Associated with Increased Rate of Acute Mortality in Mature B Cell Non-Hodgkin Lymphoma in a Pediatric Population-Study from Tertiary Care Hospital in Pakistan. Mediterranean journal of hematology and infectious diseases, 11(1):2019043.
Publisher | Google Scholor - Brown R. B. (2022). Cancer Cachexia and Dysregulated Phosphate Metabolism: Insights from Mutant p53 and Mutant Klotho Mouse Models. Metabolites, 12(12):1284.
Publisher | Google Scholor - Rampello E, Fricia T & Malaguarnera M. (2006). The management of tumor lysis syndrome. Nature clinical practice. Oncology, 3(8):438-447.
Publisher | Google Scholor - Armenian S, Bhatia S. (2018). Predicting and Preventing Anthracycline-Related Cardiotoxicity. Am Soc Clin Oncol Educ Book. 38:3-12.
Publisher | Google Scholor - Palliative care. (2020, August 5).
Publisher | Google Scholor - Oerlemans S, Mols F, Nijziel M. R, Zijlstra W. P, Coebergh J. W. W & Poll-Franse L. V. van de. (2014, May 13). The course of anxiety and depression for patients with Hodgkin’s lymphoma or diffuse large B cell lymphoma: A longitudinal study of the profile’s registry - journal of cancer survivorship. SpringerLink.
Publisher | Google Scholor - Schmitz N, Buske C & Gisselbrecht C. (n.d.). Autologous stem cell transplantation in lymphoma. Seminars in hematology.
Publisher | Google Scholor - Wilson F. P & Berns J. S. (2012). Onco-nephrology: tumor lysis syndrome. Clinical journal of the American Society of Nephrology: CJASN, 7(10):1730-1739.
Publisher | Google Scholor













