

Research Article
Treatment Personalization and Optimization in Patients with Nasopharyngeal Carcinoma: A Single Institution Experience
1 Former, Radiation Oncologist. Princess Norah Oncology Center, King Abdul Aziz Medical City, Jeddah, Saudi Arabia.
2 Medical physics section, Princess Norah Oncology Center, King Abdul Aziz Medical City, Jeddah, Saudi Arabia.
3 Head Medical physics section. Princess Norah Oncology Center, King Abdul Aziz Medical City, Jeddah, Saudi Arabia.
4 Medical Oncology department. Princess Norah Oncology Center, King Abdul Aziz Medical City, Jeddah, Saudi Arabia.
*Corresponding Author: Alsafadi N, Former, Radiation Oncologist. Princess Norah Oncology Center, King Abdul Aziz Medical City, Jeddah, Saudi Arabia.
Citation: Alsafadi N, Khan M, Albarakati Y, Alduhaiby E, Alshehri A. (2024). Treatment Personalization and Optimization in Patients with Nasopharyngeal Carcinoma. A Single Institution. Journal of Cancer Management and Research, BioRes Scientia publishers. 2(1):1-9. DOI: 10.59657/2996-4563.brs.24.007
Copyright: © 2024 Alsafadi N. Akl, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 04, 2023 | Accepted: September 18, 2023 | Published: September 26, 2023
Abstract
Background: Despite the significant improvement achieved in the management of patients with Nasopharyngeal Carcinoma (NPC), the results in terms of survival and Quality-of-Life (QoL) can still be optimized. Locally advanced tumors require aggressive approach for long-term control. Young patients have a higher cure rate, however, may suffer worsening QoL as they live longer. The aim of this study is to retrospectively compare 2 groups of patients treated with a personalized radiotherapy (RT) approach with regards to their survival and QoL outcome.
Methods and material: We reviewed all non-metastatic adult NPC patients who received radical radiation therapy (RT) at our institution from January 2014 through December 2018. Twenty-six patients were treated with conventionally fractionated RT and constitute group 1 (G-1. SFX), and another 30 patients were treated with dose-adapted hyperfractionated RT, labelled group 2 (G-2. HFX). The choice of the protocol was based on the primary tumor extent, and patient’s age. All patients received Adaptive Radiotherapy (ART). The majority of all 56 patients had stage III & IV disease and therefore received induction and concurrent weekly chemotherapy.
Results: G-2 patients had a significantly more T4s, and stage IV than G-1 patients (T4: 70% vs. 8%, p<0.001. Stage IV: 80% vs. 19%. p<0.001), were younger (Mean age: 38 years vs. 49. p=0.025), and had a significantly shorter mean follow-up time (38.5 months vs. 63.7 months. p<0.001). We counted 5 relapses in G-1 (3 Local-regional), and 4 in G-2 (1 Local-regional). There was no significant difference between the two groups in any of the measured oncologic outcome parameters, including Overall survival (OS), Progression Free survival (PFS), and Local-Regional Progression free survival (LR-PFS). If both groups are combined, the 4-year PFS, and OS were 84%, and 93%. No major severe long-term complications were encountered in either group.
Conclusion: The personalization of the RT dose/fractionation protocol and the integration of ART in every patient’s management plan seems beneficial, and can optimize the tumor control and QoL. The usage of chemotherapy (adjuvant/concurrent) can be adjusted accordingly.
Keywords: nasopharyngeal cancer; locally advanced tumors; treatment personalization and optimization; hyper fractionated radiotherapy; quality of life
Introduction
The outcome of patients with Nasopharyngeal Carcinoma (NPC) has significantly improved during the last few decades [1]. The 5-year survival rates jumped from around 25% in the 1960s to over 75% in the 2000s.This is probably the results of better imaging, staging, and the integration of effective chemotherapy. The technical innovations in radiotherapy (RT) including the wide use of Intensity Modulated Radiation Therapy (IMRT) and similar techniques had a major impact, not only on improving the toxicity profile, but also on achieving better tumor control. The combination of all these tools resulted in the outstanding increase in patients’ survival rates.
Unfortunately, the majority of our patients present with locally advanced disease (LA-NPC), requiring an aggressive management approach to achieve Local-regional Control (LRC) with optimal survival rates. A less studied and reported outcome is the long-term toxicity, particularly in patients treated with RT and full dose concurrent chemotherapy (CT). This is probably more relevant in younger patients, especially those under 30 years, commonly seen in our population. They have better cure rates, yet are particularly vulnerable to the long-term side effects of the standard treatment.
Conventionally fractionated RT (SFX) uses doses of 66-70 Gy in 33-35 fractions delivered once a day, five days a week. This is comparable to the protocols used in other squamous cell carcinoma of the head & neck region (HN-SCC). When combined with Cisplatin based concurrent chemotherapy a significant gain in LRC, and OS rates is shown in a recent meta-analysis[5]. The same applies to LA-NPC reported more recently, particularly for trials using concurrent and adjuvant chemotherapy (Mortality hazard ratio: 0.65, 0.56-0.76 in favor of concurrent and adjuvant chemotherapy) [6]. Concurrent chemotherapy alone conferred a less significant absolute improvement in OS of 5.3% (70.4% vs. 65.1% for the control).
On the other hand, a few meta-analyses of trials dealing with modified fractionation RT in patients with locally advanced HN-SCC show significant improvement in LRC & OS compared to SFX. The best results are obtained using hyper fractionated RT (HFX) consisting of 2 small daily fractions (1.1-1.2 Gy) separated by at least 6 hours to a total of 80-82 Gy [7,8]. The improvement in OS with HFX is of the same magnitude shown with concurrent chemo-radiotherapy. Unlike the latter, HFX is not associated with excessive late toxicity[7,9]. Despite the above, concurrent chemoradiotherapy continues to be the preferred choice for most clinicians [10]. This is probably the result of the early reports of the RTOG 90-03 trial[11,12], the belief among oncologists that concurrent chemoradiotherapy is more effective, and likely the logistic issues associated with HFX.
Material and Method
Our goal has been to optimize the treatment package offered to our patients. We treat many young patients, and many with T4 lesions, difficult to manage even with IMRT. For many years, we have been using induction chemotherapy, mainly a combination of Docetaxel, Cisplatin and 5-FU (TPF), followed by a “less aggressive” form of concurrent chemo-radiotherapy (CRT) using weekly Carboplatin for patients presenting with stage IV, and majority of stage III [13]. More recently, there was a trend to treat young patients under 30 years of age, and those with T4 lesions with dose-adapted HFX (69-77 Gy with fraction size 1.1-1.15 Gy to the gross Tumor Volume: GTV), aiming at limiting the occurrence of severe late toxicity while maintaining and/or improving the primary tumor control. The use of Volumetric Modulated Arc Therapy (VMAT) with concomitant boost technique, added to adaptive RT (ART) helped a lot in planning optimization. All of our patients are replanned twice during the 7-week course of RT, with contrast enhanced CT scan, re-contouring and re-optimization.
We collected 56 patients treated with radical RT between January 2014 and December 2018. These were divided into two groups. Group 1 (G-1) treated with SFX (one fraction a day) with 26 patients, and group 2 (G-2) treated with HFX (2 fractions a day) with 30 patients. The use of HFX showed a relative increase over time, and the majority of patients in G-2 were treated more recently, therefore, have a shorter follow-up. The majority of these patients were staged using the AJCC staging system 7th edition.
Results
As expected, G-2 consisted of younger patients (Mean age 38 vs. 49 years. p<0>Table 1. The histopathology data were not collected for the purpose of this study. However, from our previous series over 90% of our patients present with the endemic type (Undifferentiated Carcinoma Nasopharyngeal Type, WHO type 3) [13].
Table 1: Patients’ characteristics
| GROUP 1 | % | % | GROUP 2 | p | ||
| AGE (year) | MEAN/MEDIAN | 49/52 | 38/39 | 0.025 | ||
| RANGE | 15-99 | 14-64 | ||||
| SEX | MALE/FEMALE | 15/11 | 58% | 70% | 21/9 | NS |
| STAGE | IV/TOTAL | 5/26 | 19% | 80% | 24/30 | <0> |
| T4 | T4/TOTAL | 2/26 | 8% | 70% | 21/30 | <0> |
| N3 | N3/TOTAL | 2/26 | 8% | 23% | 7/30 | NS |
| RT | MEAN D/F | 68/33.6 | 72.5/63.5 | <0> | ||
| RANGE: D | 66-70 | 69-77 | ||||
| RANGE: F | 33-35 | 60-67 | ||||
| MEAN TIME (D) | 49 | 49 | NS | |||
| RANGE TIME | 45-55 | 45-56 | ||||
| FU | MEAN (M) | 63.7 | 38.5 | <0> | ||
| FU | RANGE | 25-83 | 14-78 |
RT: Radiotherapy. D: Total dose in Gy. F: Total number of fractions. Time: Total treatment time in days. FU: Follow-up. M: Month
The compliance to RT was good in both groups, with minimal interruptions. All patients were treated with VMAT, with concomitant boost technique. The mean total dose was significantly higher with HFX vs. SFX (72.5 Gy vs. 68 Gy. p<0>G-1 vs. G-2 with 95% Confidence Interval (CI). PFS: 80% (CI: 59-91) vs. 87% (CI: 69-95). LR-PFS: 88% (CI: 68-96) vs. 97% (CI: 78-99). OS: 96% (CI: 78-99) vs. 90% (CI: 73-97). If both groups are combined, the 4-year PFS, and OS will be 84% (CI: 72-92), and 93% (CI: 84-98). Table 2. Figure 1-4.
Table 2: Patients’ outcome.
| GROUP 1 | GROUP 2 | p | ||
| NUMBER | 26 | 30 | ||
| F.U (MONTH) | MEAN | 63.7 | 38.5 | <0> |
| RANGE | 25-83 | 14-78 | ||
| RELAPSE | LRR | 2 | 1 | |
| D | 2 | 3 | ||
| LRR+D | 1 | 0 | ||
| T.T.R (MONTH) | MEAN | 26 | 16 | NS |
| RANGE | 14-38 | 9-24 | ||
| SALVAGED | 1 | 0 | ||
| AWD | 3 | 1 | ||
| ADF | 1 | 0 | ||
| DEAD | 1 | 3 | ||
| PFS | 3 YEARS | 84 | 86 | NS |
| 4 YEARS | 80 | 86 | NS | |
| OS | 3 YEARS | 100 | 90 | NS |
| 4 YEARS | 96 | 90 | NS | |
| LRPFS | 3 YEARS | 92 | 96 | NS |
| 4 YEARS | 88 | 96 | NS | |
| GROUP 1 & 2 | ||||
| PFS | 3 YEARS | 84 | ||
| 4 YEARS | 84 | |||
| OS | 3 YEARS | 94 | ||
| 4 YEARS | 94 | |||
F.U: Follow-up. T.T.R: Time to relapse. AWD: Alive with disease. ADF: Alive disease-free. LRR: Local-Regional relapse. D: Distant relapse. PFS: Progression-free survival. OS: Overall survival. LRPFS: local-regional progression free survival.
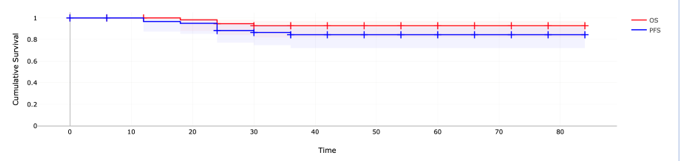
Figure 1: Overall survival & Progression-free survival in months.
All 56 patients (OS: Overall survival. PFS: Progression free survival)
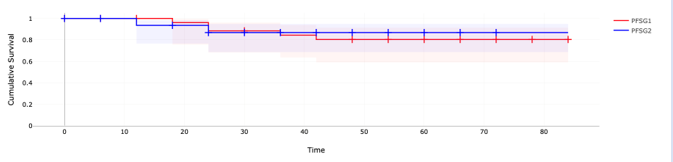
Figure 2: Progression-free survival in months.
PFSG1: Group 1. PFSG2: Group 2
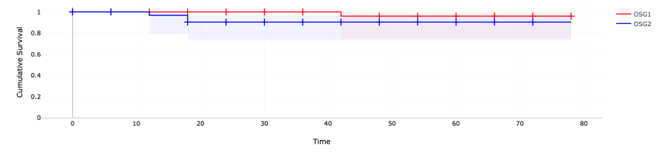
Figure 3: Overall survival in months.
OSG1: Group 1. OSG2: Group 2.
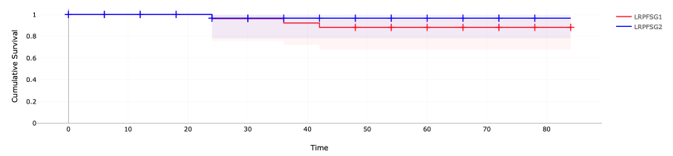
Figure 4: Local-regional progression-free survival in months.
LRPFSG1: Group1. LRPFSG2: Group 2.
This study was designed to collect Quality-of-Life (QoL) data using the EORTC QLQ-H&N35 questionnaire for a randomly chosen patients in both groups. We used the Arabic version of the given questionnaire that was completed by the patients. Unfortunately, for some organizational issues, only 15 patients in G-2 completed the questionnaire. Subsequently, we used a matching sample of 20 patients treated with SFX outside this study as a control group. The findings are reported in table 3. The most encountered late effects in G-2 patients were related to dry mouth, sticky saliva, and teeth problems with a mean score of 2-3/4. The 30 items mean score was 53.5 (35-135). This is not different from the control SFX group. It is worth mentioning that no patient required a feeding tube during or after RT, and no patient showed evidence of a major late toxicity including cranial nerves dysfunction, symptomatic brain necrosis in either group.
Table 3: QoL. EORTC-QLQ. H&N35.
| QSR | SFX. MEAN (20) | G2. MEAN (15) | P | |
| Swallow pureed food | 1-4 | 1.25 | 2.07 | |
| Dry mouth | 1-4 | 2.45 | 2.33 | |
| Sticky saliva | 1-4 | 1.8 | 2.1 | |
| Teeth problems | 1-4 | 2.05 | 2 | |
| Chocking | 1-4 | 1.5 | 1.6 | |
| Feeding tube | 1-2 | 1 | 1 | |
| Mean | 1.67 | 1.85 | ||
| Total Score | 35-130 | 50.65 | 53.5 | NS |
QSR: Questionnaire score range.
Discussion
Late treatment related complications remain a concernwhen treating LA-NPC with chemoradiotherapy [14,15]. The role of HFX in the management these patients has been poorly investigated[16,17]. Standard HFX dose in the rage of 80 Gy may lead to unacceptable toxicities. However, HFX dose up to 77 Gy are probably safe, and would likely improve the therapeutic ratio (i.e., uncomplicated cure). In this retrospective review, we tried to assess the effect of our “personalized” approach on the patients’ outcome. Our aim was to find-out if the detrimental effect of T4/stage IV on LR-PFS/OS and QoL can be offset by the use of HFX within the reported dose range. We previously demonstrated the positive effect of HFX on the Tumor Control Probability (TCP), and Normal Tissues Complication Probability (NTCP) in an experimental study, using a radiobiological model[18]. Even though limited by the small number of events/patients, our present study does not show any significant difference in any of the oncologic end results, or QoL score between the two groups. After correcting for the effect of confounding factors including younger age and shorter follow-up in G-2, it is unlikely these results will change. For example, the latest relapse in G-1 occurred at 38 months which equals the mean follow-up of G-2. One might expect 2 more relapses in G-2 with longer follow-up which will not affect the relatively good outcome. The short-term results of HFX in patients presenting with T4 tumors in this series are promising and deserve further follow-up.
It would also be worth reviewing the entire series as a single group of patients. This is basically a LA-NPC series treated at a single institution with a dynamic management plan. Apart from the personalized approach to choosing the RT dose/fractionation, the quality of RT delivered was well controlled. The integration of VMAT for all patients along with the Adaptive RT (ART) is interesting. We previously reported that ART improves target coverage with better organ at risks sparing [19]. The avoidance of full dose Cisplatin concurrent chemoradiation certainly helped improving the treatment compliance, and may lead to better QoL. Longer follow-up is required.
As stated wisely by Feigen berg in his elegant comment on RTOG 90-03 trial [20] HFX is certainly not from the “passé”. It is unfortunate that this “best-fit” form of radiotherapy in Head & Neck cancer was abandoned prematurely without waiting for final results of the RTOG 9003 trial, and before the long-term reports on late toxicity of concurrent chemoradiotherapy became available.
The late toxicity figures reported by Blanchard [6] in his meta-analysis are probably an underestimate of the true incidence. Late toxicity figures were available for less than 50% of the entire patient’s population. Those receiving concurrent chemoradiotherapy were not analyzed separately. Therefore, the late toxicity in this subgroup of patients is likely higher based on the data from other Head & Neck cancer reviews. We exceptionally use full dose concurrent cisplatin following induction chemotherapy. Instead, weekly Carboplatin dosed at an Area Under the Curve of 1.5-2 is tolerable with HFX. We believe avoiding concurrent chemoradiotherapy in favor of HFX alone is possible following induction chemotherapy, in patients achieving a major response. (Figure 4). Table 4 compares four schemes of RT including the one used in this series. In the setting of LA-NPC, and following induction chemotherapy, HFX with VMAT with 2 dose levels to 77 Gy & 66 Gy in 67 fractions seems to achieve to best biologic dose equivalent (BED) distribution, particularly at the primary tumor site, and surrounding neurologic structures.
Table 4: Comparison of different radiotherapy schemes.
| Scheme | T. Dose | D/F | T. F | a/b | D2 | TTT | D.I (Gy/W) | BED | BED vs. R | |
| HFX-CB | GTV | 77 | 1.15 | 67 | 10 | 73.5 | 46 | 11 | 88 | +5% |
| CTV | 64 | 0.95 | 67 | 10 | 55 | 46 | 9.4 | 66 | +10% | |
| LRNT1 | 77 | 1.15 | 67 | 2 | 61 | 46 | 122 | -13% | ||
| LRNT2 | 64 | 0.95 | 67 | 2 | 47 | 46 | 94 | -6% | ||
| SFX-CB | GTV | 70 | 2 | 35 | 10 | 70 | 47 | 10 | 84 | 0 |
| CTV | 60 | 1.7 | 35 | 10 | 54.5 | 47 | 8.5 | 72 | +12 | |
| LRNT1 | 70 | 2 | 35 | 2 | 70 | 47 | 140 | 0 | ||
| LRNT2 | 60 | 1.7 | 35 | 2 | 55.5 | 47 | 111 | +11% | ||
| HFX-2P | GTV | 77 | 1.15 | 67 | 10 | 73.5 | 46 | 11.5 | 88 | +5% |
| CTV | 60 | 1.15 | 52 | 10 | 56 | 37 | 11.5 | 67 | +12% | |
| LRNT1 | 77 | 1.15 | 67 | 2 | 65 | 46 | 122 | -13% | ||
| LRNT2 | 60 | 1.15 | 52 | 2 | 47 | 37 | 94 | -6% | ||
| SFX-2P | GTV | 70 | 2 | 35 | 10 | 70 | 47 | 10 | 84 | R |
| CTV | 50 | 2 | 25 | 10 | 50 | 33 | 10 | 60 | R | |
| LRNT1 | 70 | 2 | 35 | 2 | 70 | 47 | 140 | R | ||
| LRNT2 | 50 | 2 | 25 | 2 | 50 | 33 | 100 | R |
T. Dose: Total dose. D/F: Dose per-fraction. T.F: Number of fractions. D2: Dose equivalent at 2 Gy/F, 5 fractions/week. for GTV & CTV every day gain/loss in TTT is counted as +/- 0.5 Gy. TTT: Total treatment time in days. D.I: Dose intensity (Gray per-week). BED: Biologic effective dose. HFX-CB: Hyper fractionated radiotherapy with concomitant boost. SFX: Conventionally fractionated radiotherapy. 2P: 2 phases plan. GTV: Gross Tumor Volume. CTV: Clinical Target Volume. LRNT1,2: Late Reacting Normal Tissues included in GTV & CTV. R: Reference scheme.
Figure 5 demonstrates the advantage of HFX on sparing late reacting tissues, especially in the setting of VMAT. Notice that the 68 Gy equivalent of HFX at the level of the gross tumor volume (GTV) is delivered in 6 weeks, adding an element of acceleration as well, where it is needed most (GTV). The dose intensity (Gy/Week) at the 66 Gy CTV and surrounding normal tissues is under 10 in favor of better tolerance and compliance. We are using the same concept for patients with locally advanced laryngeal cancer who are candidate for laryngeal preservation. Patients showing a major response to induction chemotherapy are treated with full dose HFX without chemotherapy. Our early results in terms of tumor control and laryngeal function are excellent (Figure 5).
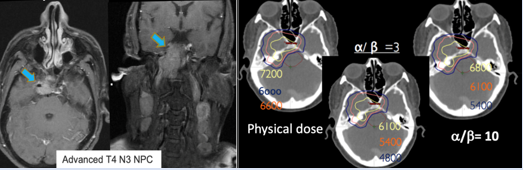
Figure 5: A: Tumor extent at presentation. B: Schematization of the advantage of HFX on sparing late reacting tissues.
HFX 72 Gy in 60 fractions twice-a-day in 6 weeks. Left: Physical dose distribution. Right: Dose equivalent in 2 Gy/F for tumor (a/b=10). Middle: Dose equivalent in 2 Gy/F for late reacting tissues (a/b=3).
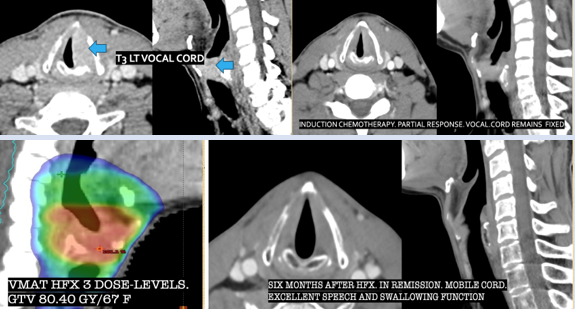
Figure 6: Locally advanced left vocal cord carcinoma (T3N0M0). A: At presentation. B: Following 3 cycles of chemotherapy. C: Radiotherapy plan. D: At six months follow-up.
Certainly, as mentioned by Mathtay [9]: “When dealing with locally advanced Head & Neck cancer, the highest priority is cure and length of survival. Excessive concern about treatment toxicity should not prevent the use of proven aggressive multimodality treatment, provided the patient is well informed about the potential late sequelae of these aggressive treatment regimens”. However, when other treatment options exist (i.e., Hyper fractionated radiotherapy), they also should be discussed with the patients before making a final decision.
Conclusion
The optimal results when dealing with NPC patients depend largely on the quality of care delivered. This includes staging, choice of the treatment protocol, handling the combination of chemotherapy-radiotherapy, and particularly the quality of RT delivered. Treatment personalization and optimization is a useful tool to be integrated in the treatment protocols. Cutting-down the intensity of concurrent chemotherapy in favor of HFX is possible, and may improve the functional outcome, and reduce the treatment toxicity without compromising the cure rate.
It is a little surprising that other forms of modified fractionation (i.e., Hypofraction) have become standard of care when dealing with certain tumor types such as breast and prostate cancer, despite the lack of tumor control or late toxicity benefits. Certainly, the shorter treatment time and reduced number of fractions, is a significant advantage in favor of hypofractionation. In contrast, in Head and Neck cancer we had definite evidence of superiority of hyper fractionation in terms of both tumor control and late toxicity (depending on the dose level chosen) for long time, yet this form of fractionation is rarely used in the clinic. Instead, a more complex, potentially toxic, and probably more costly combination with chemotherapy is often recommended. We believe, the practice of hyper fractionated radiotherapy in squamous cell carcinoma of the Head and Neck deserves to be re-visited.
References
- Lee Lin. (2012). Current Management of Nasopharyngeal Cancer. Semin. Rad. Oncol, 22(3):233-244.
Publisher | Google Scholor - Alsafadi N. (2020). Nasopharyngeal Cancer: Prevalence, Outcome, and Impact on Health-Related Quality of Life at Princess Norah Oncology Center, Jeddah, Saudi Arabia, 12(5):8199.
Publisher | Google Scholor - Yi Zhu. (2019). Assessment of Nasopharyngeal Cancer in Young Patients Aged ≤ 30 Years, 9:1179.
Publisher | Google Scholor - Yecai Huang. (2018). Clinical Outcome and Prognostic Analysis of Young Adults Nasopharyngeal Carcinoma Patients of a Nonendemic Area in Intensity-Modulated Radiotherapy Era, 15(4).
Publisher | Google Scholor - Benjamin L. (2021). Meta-Analysis of Chemotherapy in Head and Neck Cancer (MACH-NC): An Update on 107 Randomized Trials and 19,805 Patients, on Behalf of MACH-NC Group, 156:281-293.
Publisher | Google Scholor - Blanchard P. (2015). Chemotherapy and Radiotherapy in Nasopharyngeal Carcinoma: An Update of the MAC-NPC Meta-Analysis, 116(6):645-655.
Publisher | Google Scholor - Beitler J. (2014). Final Results of Local-Regional Control and Late Toxicity of RTOG 90-03; A Randomized Trial of Altered Fractionation Radiation for Locally Advanced Head and Neck Cancer, 89(1):13-20.
Publisher | Google Scholor - Lacas B. (2017). Role of Radiotherapy Fractionation in Head and Neck Cancers (MARCH): An Updated Meta-Analysis, 18(9):1221-1237.
Publisher | Google Scholor - Mathtay M. (2008). Factors Associated with Severe Late Toxicity After Concurrent Chemoradiation for Locally Advanced Head and Neck Cancer: An RTOG Analysis, 26(21):3582-3589.
Publisher | Google Scholor - James T. (2015). Summary of Major Radiation Fractionation and Chemotherapy Trials for Organ Preservation Therapy in Locally Advanced Head and Neck Squamous Cell Carcinoma, 5:343-349.
Publisher | Google Scholor - Fu KK. (1999). A Radiation Therapy Oncology Group (RTOG) Phase III Randomized Study to Compare Hyper- Fractionation and Two Variants of Accelerated Fractionation to Standard Fractionation Radiotherapy for Head and Neck Squamous Cell Carcinomas: Preliminary Results of RTOG 9003 [Abstract], 45:145.
Publisher | Google Scholor - Fu KK. (2000). A Radiation Therapy Oncology Group (RTOG) Phase III Randomized Study to Compare Hyper- Fractionation and Two Variants of Accelerated Fractionation to Standard Fractionation Radiotherapy for Head and Neck Squamous Cell Carcinomas: First Report of RTOG 9003, 48:7-16.
Publisher | Google Scholor - Alqadah F. (2005). Nasopharyngeal Carcinoma in the Kingdom of Saudi Arabia. The Experience of the Princess Nourah Oncology Center (POC), Jeddah, 23(16):5597-5597.
Publisher | Google Scholor - Wicem S. (2014). Late Toxicities after Conventional Radiotherapy for Nasopharyngeal Radiotherapy.
Publisher | Google Scholor - Ying, J. (2015). Analysis of Late Toxicity in Nasopharyngeal Carcinoma Patients Treated with Intensity Modulated Radiation Therapy, 10:17.
Publisher | Google Scholor - Jereczek-Fossa, B. (2004). Hyper fractionated Radiotherapy in Locally Advanced Nasopharyngeal Cancer. An Analysis of 43 Consecutive Patients, 180(7):425-433.
Publisher | Google Scholor - Wygoda A. (2020). Hyperfractionated Radiotherapy Alone or in Sequential Combination Chemotherapy in Patients with Advanced Nasopharynx Cancer with Contraindications to Concurrent Radio-Chemotherapy. Long Term Results, 106(5):1154.
Publisher | Google Scholor - Alsafadi N. (2018). Toward a Personalized Radiotherapy Dose-Prescription in Locally Advanced Nasopharyngeal Carcinoma, 100(5):1346-1347.
Publisher | Google Scholor - Alsafadi N. (2016). Adaptive Radiation Therapy in Adults with Nasopharyngeal Carcinoma: A Retrospective Study at 1 Institution, 94(4):905-906.
Publisher | Google Scholor - Feigenberg S. (2014). RTOG-9003: The Untold Story, 90(2):251-252.
Publisher | Google Scholor













