

Research Article
The Role of Single Progesterone Assay in Predicting the Outcome of Threatened Miscarriage During First Trimester Pregnancy at Usmanu Danfodiyo University Teachimg Hospital Sokoto, A Prospective Cohort Study
1Department of Obstetrics and Gynaecology, Usmanu Danfodiyo University Teaching Hospital Sokoto, Sokoto, Nigeria.
2Department of Obstetrics and Gynaecology Specialist Hospital Sokoto, Sokoto, Nigeria.
3Department of internal Medicine, Usmanu Danfodiyo University Teaching Hospital Sokoto, Sokoto, Nigeria.
*Corresponding Author: Rabiu F. Anas, Department of Obstetrics and Gynaecology, Usmanu Danfodiyo University Teaching Hospital Sokoto, Sokoto, Nigeria.
Citation: Rabiu F. Anas, Henry C. Nwosu, Nafisatu A, Abubakar U. Mayana, Chapa A. Mohammmed. (2025). The Role of Single Progesterone Assay in Predicting the Outcome of Threatened Miscarriage During First Trimester Pregnancy at Usmanu Danfodiyo University Teachimg Hospital Sokoto, A Prospective Cohort Study. Journal of Women Health Care and Gynecology, BioRes Scientia Publishers. 5(3):1-6. DOI: 10.59657/2993-0871.brs.25.082
Copyright: © 2025 Anas Rabiu Funtua, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 28, 2025 | Accepted: February 14, 2025 | Published: March 08, 2025
Abstract
Background: Threatened miscarriage is an early pregnancy complication that is common worldwide. Its outcome is unpredictable causing more anxiety. A highly sensitive and specific biomarker that is capable of discriminating between viable and non-viable pregnancy would be useful for counselling, prognosticating and management. Progesterone has been studied as a useful biomarker for discriminating viable from non-viable pregnancy in patient presenting with threatened miscarriage. However, its usefulness is still questionable due to different cut off values and accuracy.
Aims and Objectives: Is to determining the usefulness of a single progesterone assay as a biomarker for predicting early pregnancy failure and to establish a cut off value in our population.
Methodology: This was a prospective Cohort study involving pregnant women presenting with threatened miscarriage in the first trimester. Relevant information was obtained and blood sample was collected for progesterone assay. At the end of first trimester, viability of their pregnancy was assessed using an ultrasound. Progesterone was compared with viability. The predictive value using the Receiver Operative Characteristic curve was also obtained.
Result: Amongst 80 respondents, 68 (85%) had a viable pregnancy, while 12 (15%) were non–viable. Mean progesterone level of 17.99 ± 9.49ng/ml in the viable group was significantly higher than 4.385 ± 1.30ng/ml in the non-viable group (p < 0.001). The predictive value using the Receiver Operative Characteristic curve (ROC)was 6.609ng/ml, with a sensitivity of 98.5% and specificity of 91.6%.
Conclusion: Serum progesterone may be a good predictor of pregnancy outcome in threatened abortion during the first trimester.
Keywords: miscarriage; threatened; abortion; progesterone; early pregnancy; first trimester; prediction; viability
Introduction
Threatened miscarriage is defined as bleeding from the genital tract during pregnancy with or without abdominal pain in absence of cervical dilation before the age of viability [1]. The World Health Organization (WHO) defined threatened abortion as pregnancy related bloody vaginal discharge or frank bleeding during the first half of pregnancy without cervical dilatation [2]. It is the most common gynecological emergency [1]. About 15 to 20% of all pregnancies will be threatened, 25% will abort spontaneously and the remainder will be carried to viability [1, 3-5].
There is often an uncertainty on the outcome of threatened miscarriage. This is because of lack of universally acceptable predictive or prognostic tool [8,9]. This often results in a lot of anxiety among patients about the pregnancy outcome. Several tools have been tried in an attempt to predict the outcome of threatened abortion with varying results. Maternal demographic characteristics, ultrasound features including Doppler parameters and maternal serum biochemical markers such as β human chorionic gonadotropin (β hCG), Progesterone, Estrogen, Activin A, Inhibin A, Testosterone, Human placental lactogen, CA 125 and pregnancy associated plasma protein – A [4, 10-14]. Results of various studies were varied and conflicting. Where results seem to tally, they differ in cutoff values of the various makers or their combinations. These contributed to the lack of a universally acceptable tool, combination of tools or cut of value for the prediction of outcome in threatened miscarriage. There is no evidence to date that has proven beyond reasonable doubt that medication or life style modification including bed rest improve the pregnancy outcome of patient presenting with threatened abortion [6]. This results in conservative measure of watchful wait. This period of uncertainty is associated with significant anxiety to both the mother and caregivers. In the presence of a reliable maker that can predict outcome of threatened miscarriage, it will allow for appropriate counselling and alley anxiety. It will also assist in further development of patient management plan.
Progesterone is a C21 steroid hormone that is released by the granulosa cell of the ovary and corpus luteum during early pregnancy. It is important in maintaining pregnancy. Recent available evidences have suggested the important role of serum progesterone level for the prediction of pregnancy outcome following threatened miscarriage [6, 11,15]. However, its sensitivity and specificity as well as critical value for differentiating between viable and nonviable pregnancy in women with threatened abortion differ between populations [16]. The aim of this study is to predict the outcome of threatened miscarriage in early pregnancy using maternal serum progesterone and to determine the cut off value of progesterone that may predict pregnancy loss in threatened miscarriage during the first trimester.
Materials and Methods
This was a prospective study involving women presenting with threatened miscarriage in Usmanu Danfodiyo University Teaching Hospital Sokoto. Women who conceived via assisted reproduction, carrying multiple gestation, are on luteal phase support with progestogen, ectopic pregnancy and pregnancy of unknown location or other forms of miscarriages were excluded. The minimum sample size was determined using the sample formula for prospective study and the standard deviation of variable from previous study was 21.3 [17] and attrition rate of 10% was added for non-despondence

A total of 80 patients were recruited consecutively. Selected cases were pregnant women within first trimester (calculated from the first day of their last menstrual period and or confirmed by an ultrasound) of pregnancy presenting with vaginal bleeding, with or without lower abdominal pain and a closed cervix. Pregnancy viability was assessed based on the criteria from the Society of Radiologist in Ultrasound Multispecialty Consensus conference on early first trimester [18].
Their bio-demographic information, and other relevant information were obtained using interviewer administered structured questionnaire. About 3mls of blood was taken by venipuncture using vacutainer method observing aseptic technique and put to a plain bottle for progesterone assay and labelled. The serum was stored at a temperature of 2 – 80 C for analysis within 5 days. AccuBind ELISA microwell was the machine that was used for the progesterone assay. It is produced by the Microbind Inc. Lake Forest, CA92630, USA. A dose response curve was plotted to ascertain the concentration of progesterone. The absorbance is plotted against progesterone concentration on a graph.
All recruited patients were followed up until the end of first trimester. They had a repeat of ultrasound at the end of the first trimester to ascertain viability. They were then grouped into viable and non-viable pregnancy.
Result
The age distribution was between 15 to 40 years, with a mean age of respondents 26.95 ± 5.663 years. There was no statistical difference between viable and non-viable pregnancy group when compared with respondent age, parity, previous history of miscarriage and occupation (Table 1).
Table 1: Socio-demographic characteristics and clinical presentation of respondents
| Characteristics | Viable n = 68 (%) | Non-viable n = 12 (%) | c2/ Fisher exact | P value |
| Age (Years) | ||||
| < 20> | 4(5.9) | 2 (1.6) | 3.694 | 0.449 |
| 20 – 24 | 15(22.1) | 3 (0.4) | ||
| 25 – 29 | 25 (31.2) | 4 (5) | ||
| 30 – 34 | 18 (22.5) | 1 (1.25) | ||
| ˃35 | 6 (7.5) | 2 (2.5) | ||
| Total | 68 (89.2) | 12 (10.8) | ||
| Parity | ||||
| Primigravida | 25 (31.3) | 6 (7.5) | 1.973 | 0.373 |
| Multigravida | 37(46.25) | 4 (5) | ||
| Grand multipara | 6 (7.5) | 2 (2.5) | ||
| Total | 68 (85) | 12 (15) | ||
| Tribe | ||||
| Hausa | 53 (66.25) | 9 (11.25) | 2.229 | 0.526 |
| Yoruba | 6 (7.5) | 0 (0) | ||
| Igbo | 2 (2.5) | 1 (1.25) | ||
| Others | 7 (8.75) | 2 (2.5) | ||
| Total | 68 (85) | 12 (15) | ||
| Religion | ||||
| Islam | 59 (73.75) | 11 (13.75) | 0.246 | 0.536 |
| Christianity | 9 (11.25) | 1 (1.25) | ||
| Others | 0(0) | 0 (0) | ||
| Total | 68 (85) | 12 (15) | ||
| Educational status | ||||
| No formal education | 9 (11.25) | 3 (3.75) | 2.353 | 0.502 |
| Primary | 4 (5) | 1 (1.25) | ||
| Secondary | 23 (28.75) | 5 (6.25) | ||
| Tertiary | 32 (40) | 3 (3.75) | ||
| Total | 68 (85) | 12 (15) | ||
| Occupation | ||||
| House wife | 42 (52.5) | 10 (0) | 4.070 | 0.397 |
| Student | 3 (3.75) | 0 (0) | ||
| Trader | 6 (7.5) | 0 (0) | ||
| Business | 2 (2.5) | 1 (1.25) | ||
| Civil servant | 15 (18.75) | 1 (1.25) | ||
| Total | 68 (85) | 12 (15) | ||
| Marital Status | ||||
| Married | 67 (83.75) | 12 (15) | 0.327 | 0.850 |
| Single | 1 (1.25) | 0 (0) | ||
| Total | 68 (85) | 12 (15) | ||
| Lower abdominal pain | ||||
| Present | 53 (66.25) | 9 (11.25) | 0.50 | 0.539 |
| Absent | 15 (18.75) | 3 (3.75) | ||
| Total | 68 (85) | 12 (15) | ||
| Previous Miscarriage | ||||
| Present | 30 (37.5) | 6 (7.5) | 0.142 | 0.472 |
| Absent | 38 (47.5) | 6 (7.5) | ||
| Total | 68 (85) | 12 (15) | ||
Table 2: Comparison between mean gestational age at presentation and serum progesterone value with pregnancy outcome
| Characteristics | Viable | Non-Viable | t test | P value |
| Mean gestational age at presentation | 9.07 ± 1.765 | 7.58 ± 0.669 | 2.876 | 0.005. |
| Mean serum progesterone level (ng/ml) | 17.99 ± 9.49 | 4.385 ± 1.30 | 4.933 | <0> |
The mean gestational age and progesterone level at presentation were significantly higher in the viable group compared to the non-viable group (Table 2). The Receiver Operator Characteristic (ROC) curve of serum progesterone is shown in figure 1. The area under the curve (AUC) was 0.998 with 95% confidence interval (0.991 – 1.000) as shown in table 3. Receiver operator characteristics curve identified that with cutoff value of 6.609 ng/ml, the sensitivity and specificity of serum progesterone level in predicting pregnancy out come with threatened abortion within the first trimester was 98.5% and 91.6% respectively. Other coordinates are shown in shown in table 4 below.
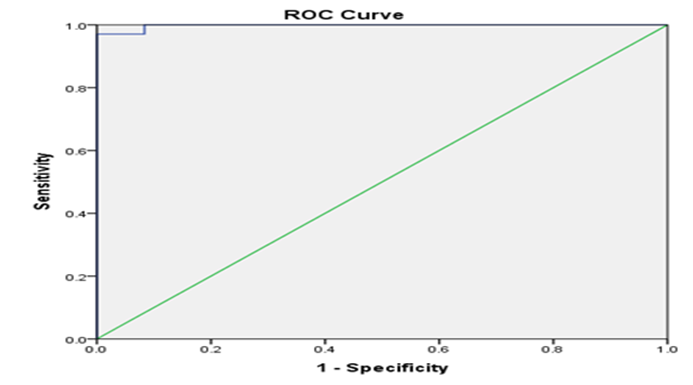
Figure 1: Sensitivity and specificity of serum progesterone in predicting the outcome of pregnancy following threatened abortion
Table 4: shows the coordinate of the curve relevant to the value with the highest sensitivity and specificity
| Cutoff values | Sensitivity | 1 - specificity |
| 5.06800 | 1.000 | 0.250 |
| 5.74350 | 1.000 | 0.167 |
| 6.21050 | 1.000 | 0.093 |
| 6.60950 | 0.985 | 0.083 |
| 6.98300 | 0.971 | 0.083 |
| 7.56050 | 0.971 | 0.000 |
| 8.04150 | 0.956 | 0.000 |
Table 5: A 2 x 2 table that shows the level of progesterone and the outcome of pregnancy
| Viable | Non-Viable | Total | ||
| Serum progesterone | ≥ 6.609 ng/ml | 67 | 1 | 68 |
| less than 6.609 ng/ml | 1 | 11 | 12 | |
| Total | 68 | 12 | 80 | |
From table 5 67 of the respondents with progesterone level equal to or above the cut off value of 6.609 ng/ml had viable pregnancy beyond first trimester and 11 of the respondents with progesterone level lower than the cut-off value of 6.609 ng/ml ended up with non-viable pregnancy. This in essence means with a cut off value of 6.609 ng/ml, the positive predictive value is 98.5 percentage, while the negative predictive value is 91.6 percentage and false positive value of 8.3% and false negative value of 1.47 percentage.
Discussion
The sociodemographic and clinical characteristics are similar between the viable and non-viable group suggesting similar risk factors for threatened miscarriage and not affecting outcome of pregnancy. The mean gestational age at presentation was 9.07 ± 1.765 weeks for the viable group and 7.58 ± 0.699 weeks for the non-viable group. This was shown to be statistically significance (t = 2.879, p = 0.005). Similar values were recorded in a study from Egypt, France and Singapore by Azza A, Puget C and Chee W respectively [13-17]. This was because over 80% of abortive condition tend to occur during the first trimester of pregnancy and the chances of failed pregnancy reduced with increased gestational age [8, 12]. There are however some studies that showed no significant relationship between the gestational age at presentation and pregnancy outcome [13, 15].
The mean progesterone level at presentation was 17.99 ± 9.09ng/ml for viable pregnancy and 4.385 ± 1.3ng/ml for non-viable pregnancy which were significant for pregnancy outcome. Similar values were recorded by Vijay in India.7 However, higher values were reported by Amr in Egypt, Zainab in Dublin, and a much higher value in a study by Hanita in Malaysia [12, 15]. This may be as a result of inherent biological and environmental differences. There seem to be consistent difference between progesterone level of viable and non-viable pregnancy which are statistically significant when correlated with pregnancy outcome. However, a study by Sherif on the prediction of spontaneous miscarriage risk by the use of first trimester ultrasound measurement and maternal serum progesterone level at week 7 of pregnancy showed a nearly similar value of progesterone values in both viable and non-viable pregnancy 30.2 ± 10ng/ml and 27.2 ± 9 ng/ml respectively [13]. This was also not found to be statistically significant (p = > 0.05). In this study apparently healthy pregnant women were recruited and progesterone assay was done at 7 weeks and pregnancy followed to 20 weeks. Therefore, it was not surprising that the serum progesterone levels are similar with no statistical difference in terms of outcome.
The predictive accuracy (Power) of maternal serum progesterone in this study was assessed using the ROC curve. The cutoff value with the highest sensitivity and specificity was 6.61ng/ml. At this cutoff, the sensitivity was 98.5% and the specificity was 91.6 percentage. The positive predictive value (PPV) was 98.5 percentage and the negative predictive value (NPV) 91.6%. In the same vein the false positive value was 8.3% and false negative value of 1.47 percentage. Similarly, the accuracy of maternal serum progesterone in predicting the outcome of threatened abortion during the first trimester has been determined by other studies using the ROC curve. In most of these studies the cutoff value of serum progesterone is higher than the value obtained in this study. The closest was a study by Puget et al whose cutoff value was 6.2ng/ml. It has a sensitivity of 20% but a specificity of 100%, PPV 100% and NPV 65.2 percentage. However, this study was conducted among women with early pregnancy of unknown viability using ultrasound definition. The mean age at presentation was also earlier than found in this study [4]. Most other results have a higher cutoff value. These were found in studies from India [11], Egypt,[16] and in Kuwait. The difference in cutoff values may be as a result of difference in studied population and methods of serum progesterone analysis. The sensitivity are all in excess of 90%, while the specificity ranges from 87.5% to 98.9 in the aforementioned studies [4, 10, 16, 20]. The negative and positive predictive values also vary from studies, from 75 percentage - 94.9 and 79.77% to 97 percentage respectively [4, 10, 16]. Despite variations in the cutoff values from different studies, it was clear that sensitivity and specificity are almost uniform, with high values. This further demonstrated the relevance of serum progesterone assay in the prediction of the outcome of pregnancy that is complicated by threatened abortion.
Conclusion
This study showed that the maternal serum level of progesterone is significantly higher in viable pregnancy than non-viable pregnancy. It has also demonstrated that a single maternal serum assay of progesterone in threatened abortion may be valuable in predicting the outcome of the pregnancy by the end of first trimester. In addition, at a serum progesterone level of 6.61ng/ml during the first trimester, the outcome of pregnancy can be predicted with a high sensitivity and specificity in our environment. This concluded that serum progesterone is a good predictor of pregnancy outcome in threatened abortion during the first trimester.
Declaration of Conflict of Interest
The authors declare no conflict of interest with respect to the research, it funding, and authorship.
References
- Ku C, Allen J, Lek S, Chia M, Tan N, Tan T. (2018). Serum progesterone distribution in normal pregnancies compared to pregnancies complicated by threatened miscarriage from 5 to 13 weeks gestation: a prospective cohort study. BMC pregnancy and childbirth, 18(1):360.
Publisher | Google Scholor - Mouri MI, Rupp TJ. (2019). Threatened Abortion. [e book] Treasure Island: StatPearls.
Publisher | Google Scholor - Lek S, Ku C, Allen J, Malhotra R, Tan N, Ostbye T, et al. (2017). Validation of serum progesterone <35nmol/L as a predictor of miscarriage among women with threatened miscarriage. BMC pregnancy and childbirth, 17(1):78.
Publisher | Google Scholor - Azza A, Mai M. (2015). Maternal Serum Β -HCG, Progeterone, Activin A, Inhibin A and uterine artery blood flow as predictors of the outcome of threatened abortion. Al-azhar assiut med jornal, 13(3):120-128.
Publisher | Google Scholor - Umar NJ, Olubiyi SK, Aliyu U, Aminat GU, Imam AA, Ibraheem MA. (2014). Spontaneous abortion among women admitted into gynaecology wards of three selected hospitals in Maiduguri, Nigeria. Int J Nur Mid, 6(2):24-31.
Publisher | Google Scholor - Abdelazim IA, Elezz AA, Elsherbiny M. (2012). Relation between single serum progesterone assay and viability of the first trimester pregnancy. SpringerPlus, 1(1):80.
Publisher | Google Scholor - Kadam VK, Agrawal S, Saxena P, Laul P. (2019). Predictive Value of Single Serum Progesterone Level for Viability in Threatened Miscarriage. Journal of obstetrics and gynaecology of India, 69(5):431-435.
Publisher | Google Scholor - Poorolajal J, Cheraghi P, Cheraghi Z, Ghahramani M, Doosti Irani A. (2014). Predictors of miscarriage: a matched case-control study. Epidemiology and health, 36:24-28.
Publisher | Google Scholor - Manokhina I, Del Gobbo GF, Konwar C, Wilson SL, Robinson WP. (2017). Review: placental biomarkers for assessing fetal health. Human molecular genetics, 26(2):237-245
Publisher | Google Scholor - Puget C, Joueidi Y, Bauville E, Laviolle B, Bendavid C, Lavoue V, et al. (2018). Serial hCG and progesterone levels to predict early pregnancy outcomes in pregnancies of uncertain viability: A prospective study. European journal of obstetrics, gynecology, and reproductive biology, 220:100-105.
Publisher | Google Scholor - Pillai RN, Konje JC, Richardson M, Tincello DG, Potdar N. (2017). Prediction of miscarriage in women with viable intrauterine pregnancy a systemic review and diagnostic accuracy metaanalysis. European journal of obstetrics, gynecology, and reproductive biology, 10(24).
Publisher | Google Scholor - Mansy AA, Taher E, Abdelrahman M, Shehata SM. CA125, progesterone & β-hCG in prediction of first trimester abortion. Reprodução & Climatério, 32(1):24-30.
Publisher | Google Scholor - El-Mekkawi SF, El-Shahawy HF, Alyamni OM. Prediction of spontaneous miscarriage risk by the use of first trimester ultrasound measurements and maternal serum progesterone level at the 7th week of pregnancy. Middle East Fertility Society Journal, 20(1):16-20.
Publisher | Google Scholor - Ku C, Allen J, Malhotra R, Chong H, Tan N, Ostbye T, et al. How can we better predict the risk of spontaneous miscarriage among women experiencing threatened miscarriage? Gynecological endocrinology. the official journal of the International Society of Gynecological Endocrinology, 31(8):647-651.
Publisher | Google Scholor - Hanita O, Hanisah AH. (2012). Potential use of single measurement of serum progesterone in detecting early pregnancy failure. The Malaysian journal of pathology, 34(1):41-46.
Publisher | Google Scholor - Saraswat L, Bhattacharya S, Maheshwari A, Bhattacharya S. Maternal and perinatal outcome in women with threatened miscarriage in the first trimester: a systematic review.
Publisher | Google Scholor - Shen SY, Chen QZ, Zhang LF, He JR, Lu JH, Li WD, et al. (2018). Association between serum progesterone concentration in early pregnancy and duration of pregnancy: a cohort study. The journal of maternal-fetal & neonatal medicine: the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies. the International Society of Perinatal Obstet,1-7.
Publisher | Google Scholor












