

Case Report
Terrible Triad of the Elbow with Simultaneous Fractures of the Ipsilateral Distal Radius
- Aamer Alharbi
- Elham Alghamdi *
- Ayman Ali
Orthopedic Surgery, King Saud Medical City, Riyadh, Saudi Arabia.
*Corresponding Author: Elham Alghamdi, Orthopaedic Surgery, King Saud Medical City, Riyadh, Saudi Arabia.
Citation: Alharbi A, Alghamdi E, Ali A. (2024). Immunotherapy and Dietary Selection, Journal of Clinical Research and Clinical Trials, BioRes Scientia Publishers, 3(1):1-5. DOI: 10.59657/2837-7184.brs.24.017
Copyright: © 2024 Elham A. Alghamdi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 08, 2023 | Accepted: September 11, 2023 | Published: January 04, 2024
Abstract
This paper presents two cases of young patients who sustained an ipsilateral terrible triad and fracture of the distal radius after falling from a significant height onto an outstretched hand. The mechanisms and management of these complex injuries are discussed, including surgical techniques and postoperative rehabilitation. This study highlights the importance of prompt diagnosis and comprehensive treatment in achieving optimal outcomes for patients who suffer from these challenging injuries.
Keywords: elbow; terrible triad; dislocation; fracture; distal radius; trauma; injury
Introduction
Dislocations of the elbow joint are common and usually involve proximal radius or ulna fracture. In general, for earm fractures occur independently [1]. Among all injuries caused in the extremities, distal radius fractures accounted for 14percentage [2]. Distal radius fractures associated with elbow dislocation are rare [3,4]. Only a few reports in the literature on elbow fracture-dislocation with ipsilateral distal radius fracture has no data on the incidence rate [1,4,5]. When a patient falls on an outstretched arm, the forces transmitted to the arm are typically loads that will be directed predominantly through either the distal radius alone or the elbow; the incidence of combined injuries is unusual. Several factors influence the management of a fracture, including the level of displacement, fracture pattern, patient's physical demands, and his/her age [2]. These two cases represent a terrible triad with ipsilateral distal radius fracture management and follow-up.
Case Report
Case 1: A 22-year-old male, medically free, was Referred from a peripheral hospital to our tertiary hospital with a history of fall from 4 meters height. Resuscitation of the patient was performed according to the Advanced Trauma Life Support protocol. Regarding orthopedics, the individual appears to have a history of right elbow dislocation with a reduction attempt in a previous hospital [figure 1].
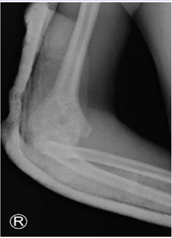
Figure 1: Trial of Reduction of a right elbow dislocation in another facility.
Along with a right radial head, distal radius fracture, right second metacarpal fracture, right ilium fracture, right sacra ala fracture extending to the Sacroiliac joint, and right superior and inferior pubic rami fracture. There was no evidence of any neurological deficit. After admission, a computed tomography scan of the right elbow reveled combination of the comminuted radial head and coronoid fractures with posterior dislocation [Figure 2] [6].
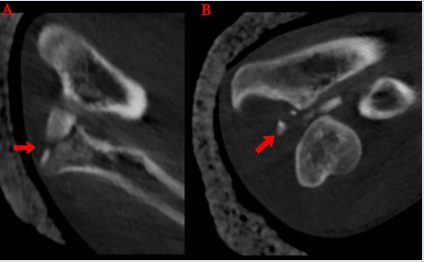
Figure 2: CT scan of the right elbow, 4A: Comminuted radius head fracture, 4B: A fracture of the ulnar coronoid process was identified [6].
As a first step, the patient underwent urgent surgery to reduce the elbow, the replacement of the radial head was carried out, and the repair of the coronoid process and the Lateral Ulnar Collateral Ligament (LUCL) [Figure 3].
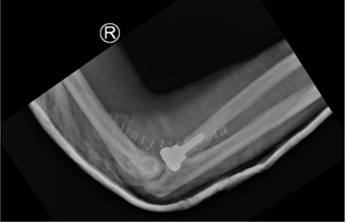
Figure 3: Postoperative replacement of the radial head.
Surgical fixation was performed to address the distal radius of the right hand [Figure4], the second metacarpal of the right hand, and the pelvis fracture on the right side.

Figure 4: Surgical fixation of the right distal radius.
Case 2: A 31-year-old male, medically free, presented with a history of falls from a height of 4 meters. Following the advanced trauma life support protocol, the patient was resuscitated. As a result of the orthopedic evaluation, the patient had a post-remedial dislocation of the left elbow [Figure 5].

Figure 5: Posteromedial dislocation of the left elbow.
A fracture of the left distal radius and the left pelvis. In the emergency room, a close reduction of the left elbow was performed, and a back slab was applied. Computed tomography (CT) image of the left elbow showed a comminuted radial head with a displaced fracture of the coronoid process. The patient needed a surgical procedure to reduce his elbow and replace his radial head using a lateral approach. After that, Surgical fixation of the left distal radius and the left-sided pelvic fracture was performed [Figure6].

Figure 6: Surgical fixation of the left distal radius.
Further follow-up after discharging the patient to determine the outcome, stability, and range of motion.
Discussion
Typically, in the event of elbow dislocation, they are accompanied by fractures around the elbow involving the radial head, olecranon, and coronoid process [7]. It is thought that several mechanisms may contribute to injury, including longitudinal compression, external rotatory force, and valgus stress to the semi flexed elbow leading to elbow dislocation [2,3]. This mechanism depends on the position of the forearm and the joint during impact. In addition, they are affected by the degree of flexion or extension of the elbow. The elbow is injured as a result of posterior tension forces. A radio capitellar joint abduction thrust could result in compression forces across the joint. A distal radius fracture occurs first in the sequence of injury. As a result, the elbow ends into the valgus. This causes secondary fractures of the radial head or neck after the radial head impacts the numerus [8].
Double injuries of the forearm are uncommon, underscoring the importance of thorough clinical examination and radiographs of joints above and below the level of injury; due to the high incidence of missed injuries, a thorough diagnostic evaluation of these injuries is crucial [4,9]. The treatment of this type of injury is not currently outlined in the guidelines. Various factors determine fracture management, including fracture pattern, displacement, stability, patient age, and physical activity [7,10,11]. A case study was done by (Wang et al., 2015) on the open reduction and stabilization of radial head fractures, followed by open reduction and internal fixation of the distal radius fractures were undertaken to restore the palmar tilt and radial inclination of the articular surface. In a case by (Akma Kamaludin et al. (2018), they first addressed ORIF for the distal end of the radius to restore radial height and reduce intraarticular fragments. Both ended with a successful clinical outcome. In our cases, due to the failure of the trial of reduction in the emergency department, we started with open reduction of the elbow and subsequent replacement of the radial head then proceeded to the distal radius.
After accurately diagnosing and treating our patients, we observed a significant improvement in the function of their elbow and wrist joints. The successful outcomes of our interventions demonstrate the crucial role of proper diagnosis and treatment in facilitating functional recovery in these joints.
Conclusion
Our experience highlights the importance of carefully examining the elbow in cases of significant wrist injuries. We also emphasize the need to consider the possibility of an elbow dislocation in such cases, as it can often be missed or misdiagnosed. By sharing our insights, we aim to raise awareness among healthcare professionals and improve the diagnosis and treatment of these injuries. Only a limited number of reports are available on the combination of a Fracture dislocation of the elbow and distal radius, ipsilaterally. This report is the first documented study in Saudi Arabia.
Disclosure of interest
The authors declare no conflicts of interest concerning this article.
References
- Ahmad R, Ahmed SM, Annamalai S, Case R. (2007). Open dislocation of the elbow with ipsilateral fracture of the radial head and distal radius: A rare combination without vascular injury. Emerg Med J, 24:860.
Publisher | Google Scholor - Elgassim M, AbuAlhaya A, Abdelrahman A, Elgassim M & Kumar T. S. (2022). Rare triad of fractures in the upper limb. Simultaneous fractures of the distal radius, with the radial head and the ulna styloid. Radiology Case Reports, 17(11):4439-4444.
Publisher | Google Scholor - Ring D, Jupiter JB. (1998). Fracture-dislocation of the elbow. J Bone Joint Surg Am, 80:566-580.
Publisher | Google Scholor - Batra S, Andrew JG. (2007). Ipsilateral compound distal radius fracture with missed elbow dislocation. A rare injury pattern. Eur J Emerg Med, 14:363-364.
Publisher | Google Scholor - Nanno M, Sawaizumi T, Ito H. (2007). Transverse divergent dislocation of the elbow with ipsilateral distal radius fracture in a child. J Orthop Trauma, 21:145-149.
Publisher | Google Scholor - Elham Ali Alghamdi, et al. (2023). “Terrible Triad Fracture Dislocation Injury Review of Current Fixation Protocols and Illustration of Single Incision Technique in 8 cases “Case Series”. Acta Scientific Orthopaedics, 6(3):148-155.
Publisher | Google Scholor - Meena S, Trikha V, Kumar R, Saini P & Sambharia A. (2013). Elbow dislocation with ipsilateral distal radius fracture. Journal of Natural Science, Biology and Medicine, 4(2):479.
Publisher | Google Scholor - Akma Kamaludin N. A, Ferdaus Kamudin N. A, Abdullah S & Sapuan J. (2018). Ipsilateral proximal and distal radius fractures with unstable elbow joint: Which should we address first? Chinese Journal of Traumatology.
Publisher | Google Scholor - El Kadi K, Benabid M, Saliou S, El Assil O, Marzouki A, Lahrach K, Boutayeb F. (2017). Simultaneous ipsilateral fractures of distal and proximal ends of the radius. Pan Afr Med J, 8(27):98.
Publisher | Google Scholor - Wang Y, Wang L & Miao, J. (2015). Comminuted fractures of ipsilateral radial head and distal radius: A rare injury pattern. Chinese Journal of Traumatology, 18(2):106-108.
Publisher | Google Scholor - Park Il-Jung MD, PhDa Sur, Yoo Joon MD, PhDb Kim, Jongmin MDa Jeon, Jin Hwa MDa Park, Ho Youn MD, PhDb. Simultaneous ipsilateral distal radius and radial head fractures: Two case reports of radius bipolar fracture. Medicine, 100(3):24036.
Publisher | Google Scholor












