

Case Report
Surgical Treatment of Femoral Epiphysis: A Systematic Review with Meta-Analysis
- Bianca Gabriella de Oliveira 1*
- Nicholas de Oliveira Marttins 2
- Luís Henrique Pimentel Boechat 3
- Henrique Oliveira Netto da Cunha 3
- Abdias Leal Caldas Neto 4
- Laís Cristina Pereira da Silva 5
1Medical student at Salvador University - UNIFACS, Salvador, BA, Brazil.
2Resident in Orthopaedics and Traumatology at Hospital Regional de Santa Maria, DF, Brazil.
3Resident in Orthopedics and Traumatology at Hospital São José do Avaí, Itaperuna, RJ, Brazil.
4Resident in Orthopedics and Traumatology, Facisa University Center - UNIFACISA, Campina Grande, PB, Brazil.
5Medical student at Salvador University - UNIFACS, Salvador, BA, Brazil.
*Corresponding Author: Bianca Gabriella de Oliveira, Medical student at Salvador University - UNIFACS, Salvador, BA, Brazil.
Citation: Bianca G. de-Oliveira, Nicholas O. Marttins, L.H.P. Boechat, H.O.N. Cunha, A.L.C. Neto, et al. (2024). Surgical Treatment of Femoral Epiphysis: A Systematic Review with Meta-Analysis, Journal of Clinical Research and Clinical Trials, BioRes Scientia Publishers. 3(2):1-7. DOI: 10.59657/2837-7184.brs.24.027
Copyright: © 2024 Bianca Gabriella de Oliveira, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 29, 2024 | Accepted: May 01, 2024 | Published: May 08, 2024
Abstract
Epiphysiolysis involves the widening and weakening of the hypertrophic layer of the proximal femoral growth plate during the growth spurt phase, which leads to epiphysiolisthesis. It affects 2 out of every 100,000 adolescents, and is more prevalent in blacks, on the left side and in males. The aim of this study is to evaluate the therapeutic options for slipped proximal femoral epiphysis using the modified Dunn osteotomy, whether performed openly or arthroscopically. Since this is a systematic literature review, it was carried out in the databases indexed in the Medical Literature Analysis and Retrieval System Online (MEDLINE) according to the precepts established by the PRISMA methodology (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). Five studies were selected on children who were submitted to surgical treatment of femoral epiphysiolysis using the modified Dunn osteotomy technique and arthroscopic osteotomy. The arthroscopic osteotomy surgical technique, discussed in recent studies, represents an innovative option to the classic subcapital realignment techniques for the treatment of chronic and stable femoral epiphysiolysis.
Keywords: femoral epiphysis; osteotomy; orthopedic procedures
Introduction
There is currently much discussion in the literature about femoral epiphysiolysis and its therapeutic evolution. It is defined by the widening and weakening of the hypertrophic layer of the proximal femoral growth plate during the growth spurt phase, which leads to epiphysiolisthesis. Pathogenesis is established and measured by the stability of the physis, taking into account the perichondral cartilaginous complex, mammillary process, collagen fibers, thickness and contour of the growth plate and physeal inclination [1]. It affects 2 out of every 100,000 adolescents, and is more prevalent in blacks, on the left side and in males. Etiologically, it has various causes: traumatic (inclination of the left femoral neck when sitting), anatomical (retroversion of the femoral head), familial (heredity 5%), inflammatory (synovitis) and/or hormonal, the most accepted, investigated by glandular or metabolic alteration [2]. The clinical manifestation is given by insignificant complaints at the beginning of the condition, evolving to pain in the inguinal region radiating to the anteromedial thigh and training, limitation of mobility, internal rotation, abduction and flexion of the frame, altered gait due to antalgic claudication. It is clinically classified as prodromal, acute and chronic [1,2].
The prodromal period is characterized by referred pain, episodic claudication, decreased internal rotation and few radiographic alterations, osteopenia and a normal femoral plate/collar ratio. The acute phase affects 10% of patients. The pain is sudden and intense, lasting less than 3 weeks and on physical examination it is possible to notice external rotation and shortening [3]. And finally, chronic is the most frequent classification, with symptoms lasting longer than 03 weeks, external rotation and shortening on physical examination due to muscle atrophy. It is worth noting the possibility of the condition worsening. Another classification is the ability to walk, with unstable patients unable to walk even with the aid of crutches and stable patients who walk with claudication [1,2,3]. Diagnosis is based on clinical suspicion in the face of pain and confirmed by complementary imaging tests. Radiography, ultrasound, bone scintigraphy, computed tomography and magnetic resonance imaging. The therapeutic approach is precisely defined with a view to preventing slippage, reducing the degree of slippage and salvage to avoid complications. The main and most aggravating complication is osteonecrosis [4].
A simple radiography allows the signs of the disease to be identified, and is always recommended in two views, the front view (anteroposterior) and the Lauenstein view (or frog view or double abduction), due to the three-dimensional condition of the human body to better show the initial signs of slippage. The concept has spread that in chronic and moderate slippage, the epiphysis deviates medially and posteriorly, leading to varus and retroversion deformities. The possibility should be considered that the displacement is of the neck and not the femoral head, which may remain in its original location because it is attached by the round ligament to the bottom of the acetabulum [5,6]. The main purposes of treating slipped capital femoral epiphysis are to prevent the progression of this slippage, restore and stabilize hip function and prevent premature osteoarthritis (OA) of the hip, reducing the risk of avascular necrosis and proximal femoral deformity. However, its treatment is a controversial subject among orthopaedic surgeons [7,8,9].
Its classic treatment is operative and may include internal fixation with in situ screws, often referred to as "pinning" or closed reduction [10,11] Numerous attempts have been made to treat severe SCFE with open and closed reduction techniques, many fraught with very high rates of avascular necrosis and chondrolysis of the epiphysis [12,13]. Therefore, the standard has become in situ fixation of the epiphysis with or without a gentle attempt at closed reduction in cases of acute dislocation, reducing the occurrence of complications, but generating femoral deformities, enabling the development of femoroacetabular impingement (FAI) [14,15]. Ganz and his colleagues then described a modified Dunn's osteotomy, performed through a surgical hip dislocation approach, thus protecting the blood supply to the femoral head, preventing avascular necrosis and also correcting the deformity. The aim of this study is to evaluate the therapeutic options for proximal femoral epiphyseal slippage using the modified Dunn osteotomy, whether performed openly or arthroscopically [16,17].
Materials and Methods
This is a study of a systematic review of the literature, structured according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), with a subsequent PRISMA checklist for analyzing the results. In addition to a flow chart of phases, prioritizing clarity and transparency in the execution of the systematic review and selection of studies.18 The data search took place on June 5th, 2022, in the databases linked to the Medical Literature Analysis and Retrieval System Online (MEDLINE), using the SPICE strategy to identify the relevant studies:
- Setting: patients with proximal epiphysiolysis
- Perspective: individuals with proximal epiphysiolysis evaluated for surgical treatment
- Intervention: surgery to correct proximal epiphysiolysis
- Comparison: surgical correction using the modified Dunn osteotomy, arthroscopically compared to the open technique.
- Evaluation: effectiveness of the surgical technique
The descriptors in health sciences (DECS) / MESH TERMS were used in combination, according to the following structures: Femoral epiphysis AND Osteotomy AND Orthopedic procedures [19].
Inclusion and exclusion criteria
Studies that met the following criteria were included: (1) age group < 18>
The studies were analyzed by two independent reviewers. Production was based on the use of the DECS and Boolean operators mentioned above, selecting studies published in the last fifteen years (2008-2022). At this stage, the titles and abstracts were analyzed, as well as the texts, and studies that did not meet the inclusion criteria were excluded.
The systematic review protocol was registered in the International prospective register of systematic reviews (PROSPERO) under ID CRD42023474382.
Results
A total of 193 papers were selected and articles published more than 15 years ago were removed, leaving 49 papers. After evaluating the titles, 09 articles were excluded, leaving 21 for full reading. Finally, 5 articles were selected for evaluation and discussion of the results. Five studies were selected on children who underwent surgical treatment of the femoral epiphysis using the modified Dunn osteotomy technique and/or arthroscopic osteotomy. The study included 126 patients with a mean age of 12.2 years. Of these, seven were treated using the arthroscopic osteotomy technique and 119 using the modified Dunn osteotomy. The results obtained are related to the variations in the measurements of the epiphyseal-diaphyseal angles (EDA) pre- and post-operatively.
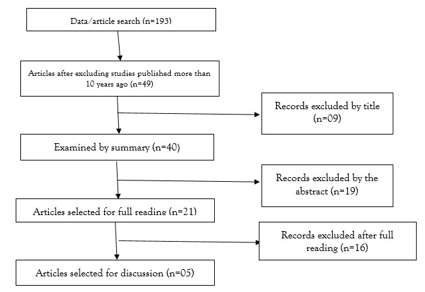
Figure 1: shows the method for selecting articles using the PRISMA methodology as a basis.
Table 1: shows the studies selected for analysis and their respective results (Table 1). [20,24]
| Study | Sample | Average age | Arthroscopic osteotomy | Osteotomy modified Dunn technique | EDA pre-surgery* | EDA post-surgery* |
| Roos e col | 7 patients | 11 years old | 7 patients | - | 51.2 +- 12.4 | 11.2 +- 5.1 |
| Zuo e col | 20 patients | 13.2 years olds | - | 20 patients | 63.2 +- 8.1 | 7.5+-3.5 |
| Lerch e col | 46 patients | 13 years old | - | 46 patients | 64 +- 6.5 | 7 +- 2.3 |
| Slongo e col | 23 patients | 11.9 years old | - | 23 patients | 47.6 +- 19 | 4.6+-2.9 |
| Persinger e col | 30 patients | 12.3 years old | - | 30 patients | 65 +- 11.2 | 16+-3.3 |
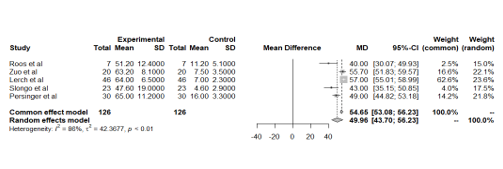
Figure 2: shows the analysis of the variation in pre- and post-operative epiphyseal-diaphyseal angle (EDA) measurements in each study.
The pre- and post-operative epiphyseal-diaphyseal angle (EDA) measurements showed a reduction of approximately 89.0% in the number of cases treated by Dunn's osteotomy.
Discussion
Several aspects of slipped capital femoral epiphysis remain controversial. Loder's work was fundamental in changing the understanding and delimitation of the surgical approach through the evaluation of sliding instability [25] However, two different types of SCFE became apparent; unstable where the patient cannot ambulate even with crutches, and stable where the patient can ambulate. Loder showed that AVN developed in 47% of the unstable slips, but none of the stable hips [25,28]. Loder's classification is often used to define stability, since a stable slip is defined as one in which the patient can ambulate with or without the aid of crutches. An unstable slip, on the other hand, is one in which the individual is unable to ambulate even with help [25]. Its severity, on the other hand, depends on the Southwick sliding angle. This is defined as the angle between the axis and a line perpendicular to the epiphysis in the lateral view of the frog's hip. Then subtract from the normal hip against the lateral view or in the case of bilateral epiphysiolysis, subtract 10 degrees. Slippages are characterized as mild (0-30°), moderate (30-60°) or severe (> 60°).29 Although the diagnosis of SCFE is generally based on radiographic findings, ultrasound can also be used to diagnose and classify the severity of the deformity [30,43,44].
The historical treatment of SCFE included immobilization with plaster, which was replaced by in situ fixation or pinning, to stabilize the physis with a few pins and, more recently, one or two cannulated screws [31]. Although it demonstrates stable closure of the proximal femoral physis and good short-term clinical results, other studies point to the development of early OA in patients, especially in cases of severe deformity. In addition, the hip can remodel into an abnormal junction of the femoral head and neck, and residual deformities can lead to FAI [32,33]. The recognition of this deformity has led some surgeons to try closed or open reduction, and even closed reduction and internal fixation, similar to a femoral neck fracture, but these have not prevailed due to the increased risk of avascular necrosis [34]. Another even proposed a cuneiform osteotomy with removal of the anterior metaphysis without violating the posterior cortex. This therapeutic option allowed the epiphysis to be anatomically reduced in the metaphysis and was theoretically associated with a lower risk of avascular necrosis [35]. Then, in 1970, Dunn's osteotomy was described and has since been modified to its current form [36]. After describing the surgical approach to the dislocation, a modified technique was described to reduce the epiphysis in SCFE using trochanteric osteotomy, an extremely demanding technique, and its results depend on the experience and acumen of the surgeon [37].
In stable cases, treatment can be through arthroscopic osteotomy, with good results [38]. In unstable cases, the currently indicated approach is the modified Dunn procedure, which is a surgical dislocation of the hip, helping to restore the alignment of the proximal femur and reducing the rate of FAI [39]. The approach is carried out according to the technique described by Ganz et al. The patient is positioned in lateral decubitus and the incision is placed in line with the greater trochanter. After opening the fascia lata, a trochanteric osteotomy is performed and the pieces are rotated anteriorly, allowing the hip capsule to be exposed. This capsule is opened and aligned with the femoral neck and a capsulotomy is completed, which allows the hip to be moved after releasing the round ligament. This is followed by a complete assessment of the acetabular cavity and treatment of chondral and labral pathology. This is followed by osteochondroplasty of the head-neck junction with the hip in flexion and internal rotation, despite the osteochondroplasty, a rotation-flexion osteotomy is performed [40]. The surgical technique of arthroscopic osteotomy in the treatment of femoral epiphysiolysis, reported in recent articles, has shown satisfactory postoperative results, close to those achieved using the well-established technique of modified Dunn osteotomy. It represents an innovative option to the classic subcapital realignment techniques for the treatment of chronic and stable femoral epiphysiolysis, allowing adequate access to the hip joint, as well as adequate reduction of slippage, with the consequent theoretical advantage of rapid rehabilitation [22,24].
The two most serious complications of this disease are avascular necrosis and chondrolysis, the treatment of which attempts to prevent or delay their occurrence. The former, which occurs in up to 50% of cases with unstable epiphysiolysis, results from the kinking of blood vessels or the formation of a hematoma, preventing the blood supply to the head of the femur, which is usually associated with severe dislocation and/or fixation with more than one screw [38,39]. This complication, in particular, leads to advanced and early degenerative OA. Chondrolysis, on the other hand, is the acute loss of articular cartilage, generating stiffness and pain in the joints. Usually reported as a complication of surgical treatment, or the use of a plaster cast on the hip and/or untreated advanced SCFE, its most common cause is the unrecognized perforation of the femoral head by a pin [41,42]. The treatment of this pathology is most effective, successful and safe in its early stages, and its early recognition and treatment should be the central focus of future efforts to reduce healthcare obligations [43]. Roos et al [20] showed an angular variation of 78.0% through arthroscopic osteotomy.
Conclusion
The surgical technique of arthroscopic osteotomy, discussed in recent studies, represents an innovative option to the classic techniques of subcapital realignment for the treatment of chronic and stable femoral epiphysis. It is important to mention that the growing excess weight in the adolescent population is a common predisposing factor, suggesting an increase in incidence and highlighting the importance of studies on the subject. The results are satisfactory when compared to well-established techniques such as the arthroscopically modified Dunn's osteotomy used in cases of unstable femoral epiphysiolysis. Investment in new studies to explore this technique is therefore extremely important in order to obtain increasingly satisfactory clinical results in the treatment of femoral epiphysiolysis.
Declarations
Conflicts of Interest
This study has no conflicts of interest
Funding
This study received no financial support from public, commercial or non-profit sources.
References
- Rab GT. (1999). The geometry of slipped capital femoral epiphysis: implications for movement, impingement and corrective osteotomy. J Pediatr Orthop, 19(4):419-424.
Publisher | Google Scholor - T. D. Lerch, S. Vuilleumier, F. Schmaranzer, K. Ziebarth, S. D. Steppacher, M. Tannast, K. A. Siebenrock. (2019). Patients with severe slipped capital femoral epiphysis treated by the modified Dunn procedure have low rates of avascular necrosis, good outcomes, and little osteoarthritis at long-term follow-up, 101(4):403-414.
Publisher | Google Scholor - Dan Cosma, Dana Elena Vasilescu, Andrei Corbu, Mădălina Văleanu and Dan Vasilescu. (2016). Procedimento de Dunn modificado . The modified Dunn procedure for slipped capital femoral epiphysis does not reduce the length of the femoral neck, 32(2): 379-384.
Publisher | Google Scholor - Alshryda S, Tsnag K, Ahmed M, Adedapo A, Montgomery R. (2014). Severe slipped upper femoral epiphysis; fish osteotomy versus pinning-in-situ: an eleven year perspective. Surgeon, 12(5):244-248.
Publisher | Google Scholor - Cooperman D.R, Charles L.M, Pathria M et al. (1992). Post-mortem descrip- tion of slipped capital femoral epiphysis. J Bone Joint Surg [Br], 74:595-599.
Publisher | Google Scholor - Waldenström H. (1940). Slipping of the upper femoral epiphysis. Surg Gynec Obstet 71:198-210.
Publisher | Google Scholor - Sankar WN, Vanderhave KL, Matheney T, et al. (2013). The modified Dunn procedure for unstable slipped capital femoral epiphysis: a multicenter perspective. J Bone Joint Surg Am, 95:585-591.
Publisher | Google Scholor - Falciglia F, Aulisa AG, Giordano M, Guzzanti V. (2017). Fixation in slipped capital femoral epiphysis avoiding femoral-acetabular impingement. J Orthop Surg Res, 12(1):163.
Publisher | Google Scholor - Tokmakova KP, Stanton RP, Mason DE. (2003). Factors influencing the development of osteonecrosis in patients treated for slipped capital femoral epiphysis. J Bone Joint Surg Am, 85:798-801.
Publisher | Google Scholor - Meier MC, Meyer LC, Ferguson RL. (1992). Treatment of slipped capital femoral epiphysis with a spica cast. J Bone Joint Surg Am, 74:1522-1529.
Publisher | Google Scholor - Millis MB, Novais EN. (2011). In situ fixation for slipped capital femoral epiphysis perspectives in 2011. J Bone Joint Surg Am, 93:46-51.
Publisher | Google Scholor - Gordon JE, Abrahams MS, Dobbs MB, Luhmann SJ, Schoenecker PL. (2002). Early reduction, arthrotomy, and cannulated screw fixation in unstable slipped capital femoral epiphysis treatment. J Pediatr Orthop, 22:352-358.
Publisher | Google Scholor - Carney BT, Weinstein SL, Noble J. (1991). Long-term follow-up of slipped capital femoral epiphysis. J Bone Joint Surg Am, 73:667-674.
Publisher | Google Scholor - Gage JR, Sundberg AB, Nolan DR, Sletten RG, Winter RB. (1978). Complications after cuneiform osteotomy for moderately or severe- ly slipped capital femoral epiphysis. J Bone Joint Surg Am, 60:157-165.
Publisher | Google Scholor - Oduwole KO, de Sa D, Kay J, Findakli F, Duong A, Simunovic N et al. (2017). Surgical treatment of femoroacetabular impingement follow- ing slipped capital femoral epiphysis: a systematic review. Bone Joint Res, 6:472-480.
Publisher | Google Scholor - Dunn DM. (1964). The treatment of adolescent slipping of the upper femoral epiphysis. J Bone Joint Surg Br, 46:621-629.
Publisher | Google Scholor - Ziebarth K, Zilkens C, Spencer S, et al. (2009). Capital realignment for moderate and severe SCFE using a modified Dunn procedure. Clin Orthop Relat Res, 467:704-716.
Publisher | Google Scholor - Liberati A, Altman DG, Tetzlaff J, et al. (2009). The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Medicine, 6(7).
Publisher | Google Scholor - Booth A. (2016). Searching for qualitative research for inclusion in systematic reviews: a structured methodological review. Systematic Reviews, 5(1).
Publisher | Google Scholor - Roos BD, Assis MC de, Roos MV, Camisa A, Lima EMU, Pagani RC. (2017). Arthroscopic subcapital realignment osteotomy in chronic and stable slipped capital femoral epiphysis: early results☆. Rev bras ortop. 52(1):87-94.
Publisher | Google Scholor - Zuo B, Zhu JF, Wang XY, Wang CL, Ma F, Chen XD. (2020). Outcome of the modified Dunn procedure in severe slipped capital femoral epiphysis. J Orthop Surg Res, 15(1):506.
Publisher | Google Scholor - Lerch TD, Vuilleumier S, Schmaranzer F, et al. (2019). Patients with severe slipped capital femoral epiphysis treated by the modified Dunn procedure have low rates of avascular necrosis, good outcomes, and little osteoarthritis at long-term follow-up. Bone Joint J, 101(4):403-414.
Publisher | Google Scholor - Slongo T, Kakaty D, Krause F, Ziebarth K. (2010). Treatment of slipped capital femoral epiphysis with a modified Dunn procedure. J Bone Joint Surg Am, 92(18):2898-2908.
Publisher | Google Scholor - Persinger F, Davis RL 2nd, Samora WP, Klingele KE. (2018). Treatment of Unstable Slipped Capital Epiphysis Via the Modified Dunn Procedure. J Pediatr Orthop, 38(1):3-8.
Publisher | Google Scholor - Alshryda S, Tsang K, Ahmed M, Adedapo A, Montgomery R. (2013). Epífise femoral superior grave escorregada; Osteotomia de peixes versus pinagem in situ: uma perspectiva de onze anos. Cirurgião, 12(5):244-248.
Publisher | Google Scholor - Alves C, Steele M, Narayanan U, Howard A, Alman B, Wright JG. (2013). A redução aberta e fixação interna da epífise femoral capital deslizada instável por meio de luxação cirúrgica não diminui a taxa de necrose avascular: um estudo preliminar. J Ororte Infantil, 6(4):277-283.
Publisher | Google Scholor - Aronsson DD, Loder RT. (1996). Tratamento da epífise femoral capital instável (aguda). Clin Orthop Relat Res, 322:99-110
Publisher | Google Scholor - Carney BT, Weinstein SL, Noble J. (1991). Long-term follow-up of slipped capital femoral epiphysis. J Bone Joint Surg Am, 73(5):667-674.
Publisher | Google Scholor - Millis MB. (2017). SCFE: clinical aspects, diagnosis, and classification. J Child Orthop, 11:93-98.
Publisher | Google Scholor - Terjesen T. (1992). Ultrasonography for diagnosis of slipped capital femoral epiphysis. Acta Orthop Scand, 63(6):653-657.
Publisher | Google Scholor - Kallio PE, Lequesne GW, Paterson DC, et al. (1991). Ultrasonography in slipped capital femoral epiphysis. Diagnosis and assessment of severity. J Bone Joint Surg Br, 73(6):884-889.
Publisher | Google Scholor - Wylie JD, Novais EN. (2019). Evolving Understanding of and Treatment Approaches to Slipped Capital Femoral Epiphysis. Curr Rev Musculoskelet Med, 12(2):213-219.
Publisher | Google Scholor - Castañeda P, Ponce C, Villareal G, Vidal C. (2013). The natural history of osteoarthritis after a slipped capital femoral epiphysis/the pistol grip deformity. J Pediatr Orthop, 33(1):76-82.
Publisher | Google Scholor - Wu GS, Pollock AN. (2011). Slipped capital femoral epiphysis. Pediatr Emerg Care, 27:1095-1096.
Publisher | Google Scholor - Sankar WN, Vanderhave KL, Matheney T, et al. (2013). The modified Dunn procedure for unstable slipped capital femoral epiphysis: a multicenter perspective. J Bone Joint Surg Am, 95:585-591.
Publisher | Google Scholor - Kim SJ, Bloom T, Sabharwal S. (2013). Leg length discrepancy in patients with slipped capital femoral epiphysis. Acta Orthop, 84:271-274.
Publisher | Google Scholor - Howorth B. (1966). History: slipping of the capital femoral epiphysis. Clin Orthop, 48:11-32.
Publisher | Google Scholor - Wylie JD, Novais EN. (2019). Evolving Understanding of and Treatment Approaches to Slipped Capital Femoral Epiphysis. Curr Rev Musculoskelet Med, 12(2):213-219.
Publisher | Google Scholor - Ziebarth K, Milosevic M, Lerch TD, Steppacher SD, Slongo T, Siebenrock KA. (2017). High survivorship and little osteoarthritis at 10- year Followup in SCFE patients treated with a modified Dunn procedure. Clin Orthop Relat Res Springer US, 475:1212-1228.
Publisher | Google Scholor - This is the first long-term follow up study of the modified Dunn procedure for SCFE from Bern, Switzerland. They re- port minimal arthritis at long-term follow up that suggests acute reorientation of SCFE may prevent the degenerative change seen in many of these patients.
Publisher | Google Scholor - DUNN DM, Angel JC. (1978). Replacement of the femoral head by open operation in severe adolescent slipping of the upper femoral epiph- ysis. J Bone Joint Surg Br, 60:394-403.
Publisher | Google Scholor - Falciglia F, Aulisa AG, Giordano M, et al. (2017). Fixation in slipped capital femoral epiphysis avoiding femoral-acetabular impingement. J Orthop Surg Res, 12(1):163.
Publisher | Google Scholor - Katz DA. (2006). Slipped capital femoral epiphysis: the importance of early diagnosis. Pediatr Ann, 35(2):102-111.
Publisher | Google Scholor - Kalogrianitis S, Tan CK, Kemp GJ, Bass A, Bruce C. (2007). Does unstable slipped capital femoral epiphysis require urgent stabilization? J Pediatr Orthop B, 16(1):6-9.
Publisher | Google Scholor












