

Research Article
Service-Seeking Knowledge and Behavior Toward Safe Dental Care Among Bangladeshi Patients
- Kazi Maria Haque 1
- Bilkis Banu 2
- Nasrin Akter 2
- Sujana Haque Chowdhury 2
- Nusrat Nobi 2*
- Asma Begum 3
1.Department of Dental and Oral Health, Decent Specialized Dental Care, Khulna, Bangladesh.
2.Department of Public Health, Northern University Bangladesh, Dhaka, Bangladesh.
3.Department of Dental and Oral Health, Shahid Sheikh Abu Naser Specialized Hospital, Khulna, Bangladesh.
*Corresponding Author: Nusrat Nobi, Department of Public Health, Northern University Bangladesh, Dhaka, Bangladesh
Citation: Haque KM, Bnau B, Akter N, Chowdhury SH, Nobi N, Begum A, et al. (2023). Service-Seeking Knowledge and Behavior Toward Safe Dental Care among Bangladeshi Patients. Dentistry and Oral Health Care, BioRes Scientia Publishers. 2(4):1-11. DOI: 10.59657/2993-0863.brs.23.023
Copyright: © 2023 Nusrat Nobi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 17, 2023 | Accepted: November 30, 2023 | Published: December 08, 2023
Abstract
Aims: Safe dental service-seeking knowledge and behavior, which may help to access precise treatment management facilities regarding dental concerns, is fundamental to the sustainable management and prevention of dental diseases among the general population. The purpose of this study was to evaluate participants' knowledge and behavior about safe dental service-seeking practices.
Materials and methods: Cross-sectional research of 312 respondents in the city of Khulna dental patients was undertaken. Face-to-face interviews using a semi-structured questionnaire were utilized to collect the data, and multi-variate approaches were used to analyze it.
Results: With more female respondents (61.2%), the average age was found to be 34 years. The majority of the survey participants (69.6%) were college graduates or higher educated, came from a nuclear family (24.7%), and lived in an urban region (71%). The vast majority of respondents had inadequate knowledge (69.6%) and conduct (64.1%) when it came to seeking out safe dental care. Some socio-demographic and clinical characteristics were shown to be substantially (p0.05) linked to inadequate knowledge (less education, low blood pressure), as well as behavior (living in the country, having negative habits, and low blood pressure).
Conclusion: Regarding knowledge and conduct on safe dental service-seeking practices, this study offers a depressing scenario. To make the information more broadly applicable and to make the situation better, a sizable investigation is required. As a result, this study will give future researchers in the subject a solid foundation for their work and will be extremely helpful to the relevant policymakers.
Keywords: service-seeking; knowledge; behavior; dental care; bangladeshi patients
Introduction
One of the most crucial aspects of someone's general health and overall well-being is their oral health. It is tied to people's knowledge of oral health and good oral hygiene practices [1]. Since attitudes and behaviors are typically formed after conceptualizing oral health practices, knowledge of oral health practices alone does not guarantee that they will change in the future. On the other hand, poor dental health can cause pain and suffering, which can reduce a person's quality of life and reduce their ability to work productively [2]. The safe dental care-seeking knowledge and gets that may aid to utility accurate treatment operation facilities regarding dental troubles are fundamental to the sustainable management and prevention of dental challenges among the general public. It is stated that health-seeking behavior is any action made by a person who believes they have health problems with the intention of defining their level of health until they realize they need and accept suitable treatment [3]. Case's views on making decisions about their dental health are now shifting from being passive recipients to donors who actively participate in controlling their health and taking care of themselves [4]. Maintaining proper dental hygiene is fundamental to an individual's overall well-being in society and also helps people live longer, healthier lives. Cases should evaluate a number of variables before choosing to receive treatment at any dental clinic. The case or service provider may have a bond for these deputies [5]. This study was designed to evaluate dental patients from the Khulna megacity who seek safe dental care and visit various dental offices and sanitariums for their dental care. Dentistry that prioritizes patient safety doesn't exist in every office. Due to the nature of dental treatment, procedures frequently result in aerosols and splatters that might contain significant amounts of slaver or blood from cases and provide a risk of widespread virus transmission [6]. Age, gender, and family history appear to be particularly important determinants in the progression of oral disorders, whereas the hazard to pastoral populations seems to rise as a result of their geographic location, dietary choices, and oral hygiene practices. Socio Economic Status (SES) is the key factor in predicting oral illness [7]. There are significant regional, national, and even intranational variations in oral hygiene practices. Across the country, different oral hygiene practices have different effects on oral health. For instance, there is a high prevalence of scrapes, dental caries, periodontal diseases, and oral lesions in pastoral regions of central India as a result of the recreational and therapeutic use of tobacco and areca nuts [8]. For a very long time, the majority of people have viewed seeking dental health as an emergency step. Since pain is a symptom that manifests in the later stages of the evolution of oral diseases, there has been a significant increase in the search for treatment. Dental care is typically very expensive, which may contribute to people delaying care until it is too late. Another concern is the availability of facilities and a restricted labor force for dental healthcare [9]. An important factor in halting the development of the complaint and improving the case's quality of life is the early discovery and forestalling of it. Caregivers have a significant impact on the case's internal health, which has a significant impact on how the case seeks medical attention [10,11]. In our area, it can be difficult to convince patients to seek therapy because they are frequently ignorant, illiterate, superstitious, and of poor socioeconomic position. The authors of the study focused on analyzing the case's health seeking gets because there were little studies on this topic in our area. By analyzing the case's health-seeking behavior, it is possible to determine their attitude toward oral health, which can aid to lessen the damage the lesion causes and speed up the lesion's development. As a result, the decision to access a particular service as well as when and where to receive healthcare services is frequently linked to the claim for oral healthcare services [12]. Oral diseases, which are a crucial part of general health and have a significant impact on people's quality of life and the healthcare system, have generated a lot of public health concerns [13]. Treatment for oral health issues is typically not included in universal health coverage because it is known to be expensive [14]. With the addition of urbanization and changes in living conditions, the prevalence of oral diseases is still rising in the majority of low- and middle-income nations [14]. The spread of illness inside a dental chamber can happen through direct towel contact with blood, dribbles carrying contagious agents, or infected sharps using improperly sterilized equipment [15]. Health-related issues might arise from viral infections including HBV, AIDS, COVID-19, and HSV not just for dentists but also for their families, friends, and other cases. Therefore, the connected population's understanding of safe dental services is essential to reducing a number of cross-infection-related health effects. There have been a lot of articles published on this topic, however they are insufficient. This study fills in some of the gaps left by the previous studies. The absence of awareness of safe dental treatment seeking among dental cases is demonstrated later in the paper. More research on this topic is required to raise public awareness of the risk of dental treatment-related trans infection within dental chambers. Public and original rules and guidelines should also be easily verified and obeyed where appropriate. Among the dental cases in Khulna City, we wish to evaluate the level of awareness and behavior regarding safe dental service-seeking practices. This study will aid policymakers in developing future initiatives for the improvement of awareness of safe dental service-seeking practices, which will raise community mindfulness and help to promote dental health.
Materials And Methods
Study design
From March to June 2022, a descriptive cross-sectional study was conducted among Bangladeshi dental patients. In this study, semi-structured data on safe dental service seeking knowledge and behavior, comprising several aspects linked to demography, lifestyle, clinical and oral hygiene practice, were extracted.
Study participants, sample size and sampling
In total, 312 dental patients who were treated in two hospitals-one public and one private—in the Bangladeshi divisional city of Khulna were included in this study. Eight Bangladeshi divisions—Dhaka, Chittagong, Rajdhani, Khulna, Rangpur, Mymensingh, Sylhet, and Barisal-were chosen through a multi-stage random sampling process. The study was carried out in the two best and biggest dental hospitals, given that Khulna Divisional City has the greatest availability of dental professionals in other words, the Decent Specialized Dental Care of Khulna, Bangladesh, and the Khulna Medical College and Hospital. Quantitative data for this study was gathered from respondents indicated dental patients who went to the hospitals that were chosen for the study, were in good physical health, and gave their consent. The initial assumption was that a possible standard sample size of 368 would be obtained using the formula "n='Z2pq/d2," where Z (standard normal deviates) was taken into account as 1.96; p (the proportion was assumed to be 39.6% considering respondents' visits to dental facilities) 24 was taken into consideration as 0.50; and margin of error was taken into consideration as 0.05. However, the computed samples were reduced by 10% to 331 when respondents' non-response was taken into account. After initial management and data cleansing, the final samples were set at 312.
Data collection
Face-to-face interviews were performed to collect data from the dental patients using a pre-tested and semi-structured questionnaire. In this study, respondents were gathered in April 2022. The interviewer finished the survey in around 10 to 15 minutes. While collecting data or after it was collected, all writers had access to participant information. With the full backing of the hospital and dental administration, the survey was conducted in Bengali.
Ethical considerations
This study adheres to the Helsinki Declaration and received approval from the Northern University of Bangladesh Department of Public Health's Ethical Review Committee (NUB/DPH/EC/2022/17) to proceed. Participation in the survey was entirely optional and anonymous. The verbal informed consent of the respondents was taken at the beginning of the survey, and they were free to withdraw at any point.
Questionnaire design
The questionnaire was pre-validated by two independent reviewers and pre-tested by five respondents. The validity of the questionnaire was discussed in the pre-test responses. There were several sections in the questionnaire: Patient demographic data includes: education level, occupation, marital status, place of residence, and monthly family income (BDT). Patients are also asked about their knowledge of safe service-seeking practices, frequency of visits to safe dental chambers each year, and the type of institution they use to seek safe dental services. (iii) Personal dental knowledge and experience, including unhealthy routines, previously used medications for the mouth, and knowledge of infectious diseases.
Data analysis
Using the statistical package for the social sciences (SPSS) program, the data is verified and evaluated. Descriptive statistics (frequency and percentage) were used to the study characteristics to summarize the data that had been collected. A scoring method was used to categorize the participant's dental service knowledge and behavior. Each knowledge and behavior component were taken into account by the grading methodology. The precise responses to each knowledge question are presented. Each correct response was given a score of 1, while each incorrect response was given a score of 0. For questions with multiple answers, the score of one was divided by the total number of responses. The two categories were then separated from the overall score and converted to percentages. A score of (60%) denoted a lack of knowledge, whereas (>60%) denoted a high level of expertise. 25. A backward elimination method with the inclusion of pre-specified confounders was modelled after a multinomial logistic regression analysis. Odds ratios with 95% confidence intervals were calculated for the stated exposures for ideal and prolonged daily standing times.
Results
Table 1: Status of safe dental service seeking practice of the respondents according to their level of knowledge (n= 312)
| Knowledge on safe dental service seeking practice | Behavior on safe dental service seeking practice | ||
| Number of participants, n (%) | Good behavior, n (%) | Poor behavior, n (%) | |
| Good knowledge | 125 (40.1) | 50 (16) | 75 (24) |
| Poor knowledge | 187 (59.9) | 34 (10.9) | 153 (49.0) |
| Total | 312 (100) | 84 (26.9) | 228 (73.1) |
Chi-square analysis was carried out to determine the relationship; 2/p=18.13/0.01.
The respondent's safe dental service seeking practice is shown in Table 1 along with their level of expertise. An overall analysis reveals that the majority of the 312 respondents had inadequate knowledge, and as a result, a larger percentage of respondents also had bad conduct with reference to safe dental treatment seeking practices. But the most important thing to note is that more than half of them exhibit poor behavior (24%, n=75) rather than having strong understanding (40.1%, n=125) on safe dental care seeking practice (Table 1).
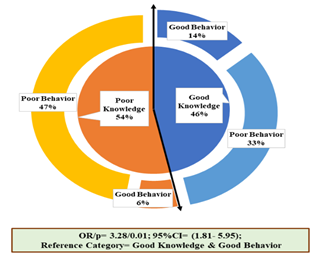
Figure-1: Correlation between Knowledge and behavior on safe dental service seeking practice among the respondents (n= 312)
Figure 1 demonstrates the relationship between respondents' knowledge and actions related to Bangladesh's safe dental service seeking practices. It was surprised to see that even while the majority of respondents did not put their good knowledge (40%) into effect in their daily lives and exhibited poor behavior (24%). However, the overall correlation result revealed that the majority of respondents (60%) had inadequate understanding, which led to bad behavior (49%) as a result (Figure 1).
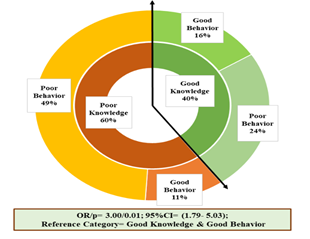
Figure-2: Correlation between Knowledge and behavior on oral hygiene practice among the respondents (n= 312).
Figure 2 shows an exclusive view of the relationship between respondents' knowledge and oral hygiene practices. Poor behavior is a rather clear effect of poor knowledge. Similar results were seen in this study, where respondents with poor understanding (54%) demonstrated resistance to practicing oral hygiene and bad conduct (47%). Furthermore, it was regrettable to learn that 33% of respondents exhibit poor practice rather than strong awareness of oral hygiene practices (Figure 2).
Table 2: Association between different components of knowledge and behavior related to safe dental service-seeking practice (n= 312).
| Characteristics | Behavior on different components of safe dental service seeking practice | ||||||
| Number of responders, n (%) | Poor, n (%) | Good, n (%) | OR (Poor vs Good) | 95% CI | p-value (≤0.05) | ||
| Knowledge on different components of safe dental service seeking practice | A professional degree of service provider of a safe dental chamber | ||||||
| Poor | 187 (59.9) | 134 (42.9) | 53 (17.0) | 2.26 | 1.41- 3.63 | 0.01* | |
| Good | 125 (40.1) | 66 (21.2) | 59 (18.9) | Ref | |||
| Frequency of visiting dental chamber in a year | |||||||
| Poor | 249 (79.8) | 207 (66.3) | 42 (13.5) | 6.57 | 3.61- 11.96 | 0.01* | |
| Good | 63 (20.2) | 27 (8.7) | 36 (11.5) | Ref | |||
| Type of institution for seeking a safe dental service | |||||||
| Poor | 180 (57.7) | 141 (45.2) | 39 (12.5) | 3.40 | 2.08- 5.57 | 0.01* | |
| Good | 132 (42.3) | 68 (21.8) | 64 (20.5) | Ref | |||
| Overall level | |||||||
| Poor | 125 (40.1) | 50 (16.0) | 75 (24.0) | 3.00 | 1.79- 5.03 | 0.01* | |
| Good | 187 (59.9) | 34 (10.9) | 153 (49.0) | Ref | |||
Data are presented as frequency (n), percentage (%); *Statistical significance at p value ≤0.05. Chi-square test was used to observe the association; risk estimated by Odds Ratio calculation and reference category considered as good knowledge and good behavior for all the variables.
The association between knowledge and behavior concerning different components of safe dental service-seeking practice is revealed in table 2. It was fortunate to observe that, the majority of respondents had overall good knowledge (59.9%, 187/312) towards safe dental service-seeking practice, which in return is significantly (p=0.01) associated with good practice (49%, n=153/312). Moving towards some basic components, the study found that majority of the respondent is not concerned about the dentist’s professional degree and types of institutes to visit for dental care, here poor knowledge (59.9%, 57.7% & n=187/312, n=180/312 respectively) is significantly (p=0.01) associated with poor behavior (42.9%, 45.2% & n=134/312, n=141/312 respectively). Finally, upon questioning, how frequently a respondent needs to visit a dental clinic, it was observed that three fourth portion of the total study subjects got poor knowledge (79.8%, n=249/312) which results in the major having poor practice (66.3207/312) (Table 2).
Table 3: Characteristics of the respondents according to the knowledge and behavior related to safe dental service seeking practice (n= 312).
| Characteristics | Knowledge | Behavior | ||||||
| Number of responders, n (%) | Good, n (%) | Poor, n (%) | p-value | Number of participants, n (%) | Good, n (%) | Poor, n (%) | p-value (≤0.05) | |
| Demography-related information | (≤0.05) | |||||||
| Education | ||||||||
| Up to SSC | 69 (22.1) | 13 (4.2) | 56 (17.9) | <0> | 69 (22.1) | 25 (8.0) | 44 (14.1) | 0.14 |
| HSC | 26 (8.3) | 16 (5.1) | 10 (3.2) | 26 (8.3) | 7 (2.2) | 19 (6.1) | ||
| Graduation/ above | 217 (69.6) | 96 (30.8) | 121 (38.8) | 217 (69.6) | 52 (16.7) | 165 (52.9) | ||
| Occupation | ||||||||
| Job Holder | 98 (31.4) | 48 (15.4) | 50 (16.0) | 0.03* | 98 (31.4) | 29 (9.3) | 69 (22.1) | 0.33 |
| Housewife/self-employed/student | 214 (68.6) | 77(24.7) | 137 (43.9) | 214 (68.6) | 55 (17.6) | 159 (51.0) | ||
| Marital Status | ||||||||
| Married | 212 (67.9) | 74 (23.7) | 138 (44.2) | 0.02* | 212 (67.9) | 61 (19.6) | 151 (48.4) | 0.28 |
| Unmarried | 100 (32.1) | 51 (16.3) | 49 (15.7) | 100 (32.1) | 23 (7.4) | 77 (24.7) | ||
| Place of living | ||||||||
| Urban | 241 (77.2) | 105 (33.7) | 136 (43.6) | 0.02* | 241 (77.2) | 71 (22.8) | 170 (54.5) | 0.06* |
| Rural | 71 (22.8) | 20 (6.4) | 51 (16.3) | 71 (22.8) | 13 (4.2) | 58 (18.6) | ||
| Monthly Family Income (in USD) | ||||||||
| ≤482.14 | 281 (90.1) | 107 (34.3) | 174 (55.8) | 0.03* | 281 (90.1) | 68 (21.8) | 213 (68.3) | 0.01* |
| >482.14 | 31 (9.9) | 18 (5.8) | 13 (4.2) | 31 (9.9) | 16 (5.1) | 15 (4.8) | ||
| Personal knowledge and practice on dental issues | ||||||||
| Deleterious Habit | ||||||||
| Yes | 94 (30.1) | 27 (8.7) | 67 (21.5) | 0.01* | 94 (30.1) | 18 (5.8) | 76 (24.4) | 0.04* |
| No | 218 (69.9) | 98 (31.4) | 120 (38.5) | 218 (69.9) | 66 (21.2) | 152 (48.7) | ||
| Medicine-taking history for dental issues | ||||||||
| Yes | 64 (20.5) | 79 (25.3) | 50 (16.0) | 0.5 | 64 (20.5) | 23 (7.4) | 41 (13.1) | 0.06* |
| No | 248 (79.5) | 46 (14.7) | 137 (43.9) | 248 (79.5) | 61 (19.6) | 187 (59.9) | ||
| Knowledge on infectious diseases | ||||||||
| Yes | 129 (41.3) | 28 (9.0) | 36 (11.5) | 0.01* | 129 (41.3) | 37 (11.9) | 92 (29.5) | 0.56 |
| No | 183 (58.7) | 97 (31.1) | 151 (48.4) | 183 (58.7) | 47 (15.1) | 136 (43.6) | ||
Data are presented as frequency (n), percentage (%); *Statistical significance at p value ≤0.05. Chi-square test was used to observe the association.
Multivariate (cross table) analysis of the study revealed a significant demographic and personal overview on dental problems related characteristics that influence their knowledge and behavior level regarding safe dental service-seeking practice. Concerning demographic background an interesting finding spot on the fact that respondent’s living status (Place of living and monthly family income) really impacts both knowledge and behavior simultaneously. Majority of the respondents who reside in urban settings & had a monthly income of less than 482.14 USD were observed to had significantly poor knowledge (43.6%, n=136/241, p= 0.02 & 55.8%, n=174/28, p= 0.03 respectively) similarly, they were also found to had statistically significant poor behavior (54.5%, n= 170/241, p= 0.06 & 68.3%, n= 213/281, p=0.01 respectively). On the other hand, it was unfortunate to observe that graduate respondents also had a significant association with poor knowledge (38.8%, n=121/217, p<0 xss=removed xss=removed n=137/214, xss=removed n=120/218, xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed p=0.06)>
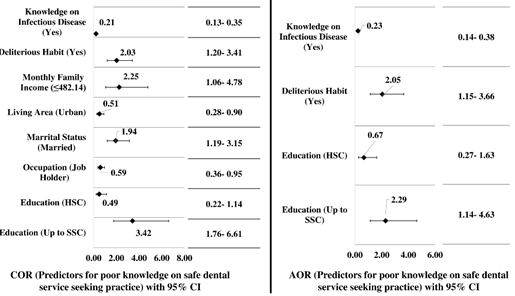
Figure 3: Predictors influencing poor knowledge on safe dental service-seeking practice among the respondents (n=312)
Fig 3 footnote: Statistically significant predictor is considered at p ≤0.05. Reference category for Knowledge on infectious disease is ‘No’; Deleterious habit is ‘No’; Monthly family income is ‘(>482.14)’; Living area is ‘Rural’; Marital status is ‘unmarried’; Occupation is ‘Housewife/self-employed/student’; Education is ‘Graduation/ above’ (Regression Analysis).
In figure 3 binary regression analysis of the study revealed significant predictors associated with poor knowledge of the safe dental service-seeking practice. Initially, married respondents (COR=1.94; 95% CI: 1.19-3.15), residing in an urban setting (COR=0.51; 95% CI: 0.28-0.90) with a monthly family income of <482 COR=2.25; COR=0.59; COR=3.42; COR=0.49; AOR=2.29; xss=removed>
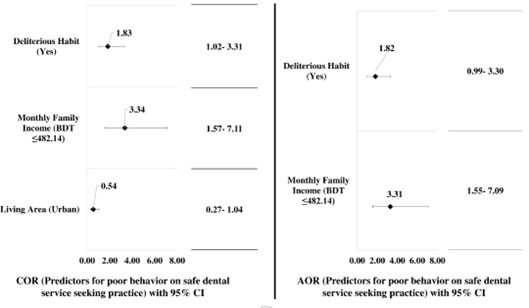
Figure 4: Predictors influencing poor behavior on safe dental service seeking practice among the respondents (n=312)
Fig 4 footnote: Statistically significant predictor is considered at p ≤0.05. Reference category for Deleterious habit is ‘No’; Monthly family income is ‘(>482.14)’; Living area is ‘Rural’ (Regression Analysis). Binary regression analysis of the study revealed significant predictors associated with poor behavior on safe dental service-seeking practice. Initially, as a predictor, respondents who resided in an urban setting (COR= 0.54; 95% CI: 0.27 – 1.04) with a monthly family income of less than 482 USD (COR= 3.34; 95% CI: 1.57 – 7.11) and who had some deleterious habits (COR= 1.83; 95% CI: 1.02 – 3.31) were identified for poor behavior. Later on, after adjusted modeling and elimination of confounders study revealed final significant predictors that are associated with poor behavior on safe dental service-seeking practice. Finally, it was observed that respondents with a monthly family income of less than 482.14 USD (AOR= 3.31; 95% CI: 1.55 – 7.09) and those respondents who had some deleterious habits (AOR= 1.82; 95% CI: 0.99 – 3.30) are our final predictors. This finding demonstrated once more that lifestyle choices and habits always account for the majority of behavior in daily life (Figure 4).
Discussions
Age, gender, occupation, and working experience have no discernible effects on the knowledge and behavior distribution pattern identified in this study. This study, however, revealed that there is a gap between the respondents' conduct and knowledge. Although oral health knowledge does not always transition into oral health behavior, it has been suggested that persons who have internalized this knowledge have some control over their dental health and are more likely to adopt healthy self-care habits [16]. This study's findings, which show that the same group of people who exhibit bad knowledge (59.9%) also exhibit poor behavior (49.0%), provide solid evidence in favor of this school of thought. According to the respondents, the link between knowledge and conduct about safe dental services is nearly three times worse (OR/p= 3.00/0.01, 95% CI= 1.79-5.03) than it is for oral hygiene practices (OR/p= 3.28/0.01, 95% CI= 1.81-5.95). Poor oral practice was also noted (57.6%) in a similar survey of school teachers conducted in the same area (Benin, Nigeria) [17]. This resemblance in pattern could be cultural. It is thought that cultural or regional factors may have influenced certain habits and customs [18]. Poor knowledge and behavior are also related to some aspects of personal compliance. Such as the type of institution for finding a safe dental service (45.2%), frequency of visiting a dentist chamber in a year (66.8%), and professional degree of the service provider. According to research performed in Saudi Arabia, 87.1% of students believe that dental appointments should be made every six months, and 34% of students had already been to the dentist [19]. The level of knowledge recorded in this study is lower (54%) than what was reported in a primary school teacher group (83.9%) where several persisting misconceptions on oral health were unveiled. 20 The respondents who completed their education up to SSC had poor knowledge (17.9%, AOR=2.29, 95% CI= 1.14-4.63). On the other side, a study projected good behavior of respondents with at least primary-level educational status (93.2%). 21 A married person's (44.2%) and the group of housewives/self-employed or students' (43.9%) poor knowledge is also taken into account. Two demographic parameters were significantly related to knowledge and conduct. One is the respondents' place of residence (COR/p= 0.54/0.01, 95% CI= 0.27-1.04), and the other is their family's monthly income (in USD) (AOR= 3.31, 95% CI= 1.55-7.09). Additionally, unfavorable possibilities were projected based on personal experience and dental practice. The respondents with harmful behaviors reported poor conduct (48.7%, AOR=1.82, 95% CI= 0.99-3.30) and knowledge (38.5%, AOR=2.05, 95% CI= 1.15-3.66) about safe dental procedures. On the other hand, history of taking medications for dental problems revealed good behavior (11.9%) in safe dental practice as well as good understanding (25.3%) of infectious diseases. Self-medication, which has been observed to be widespread among dental patients, may be the cause of this discrepancy [22,23]. The study findings were only applicable having similar situations in Bangladesh. Due to the time limitation, few dental surgeons were taken as respondents and the location was also limited. However, the strengths of the study are that the selection of participants was random and an appropriate sampling strategy was ensured. The questionnaire was tested in a pilot phase to ensure the quality and face validity of the data collection tool. The study was conducted among a diverse group of 312 dental patients reported in one public and one private hospital in Khulna divisional city of Bangladesh. The dental examination could have offered an objective assessment of oral health with a possible examination of the link between knowledge and behavior with the actual dental health status of study participants. So, overall knowledge and behavior among the respondents have been assessed by exploring their knowledge of infectious disease, maintenance of oral hygiene, required facilities in a safe dental chamber, professional expertise of the dental surgeon, and frequency of sticky food. We got poor knowledge and behavior in all ties. According to the overview, knowledge about the procedures required to prevent the transmission of infection should be updated, health policymakers should overlook on major health issues, and monitoring to find the real burden and incidence of the disease should be considered. A large-scale study is required to generalize the information and improve the situation. Hence, this study will provide future researchers of this field with a concrete base for further study and assist the pertinent arena's policymakers.
Conclusions
This cross-sectional survey of patients who visited several dental clinics and hospitals in Bangladesh's Khulna city revealed a depressing scenario regarding knowledge and behavior on safe dental care seeking practice. The majority of respondents had poor knowledge, and as a result, a larger percentage of respondents displayed negative behavior when it came to patients in Khulna City seeking safe dental services. overall expertise and behavior of the respondents has been assessed through exploring their knowledge on infectious diseases, maintenance of oral hygiene, frequency of brushing teeth daily, frequency of changing toothbrush in a year, oral hygiene material, required facilities in a safe dental chamber, professional expertise of dental surgeon, frequency of visiting to dentist in a year, type of health care center for dental check-up, bad effect of sticky food. We got poor knowledge and behavior in all tiers. Correlation among respondent’s knowledge and behavior regarding safe dental service seeking practice in Bangladesh was surprising to observe that despite of having good knowledge majority of respondent’s dose not practice it in their daily life and shows poor behavior. On the other hand, concerning overall result of correlation it was found that among total respondent’s maximum of them had poor knowledge and which results poor behavior as well. To make the information more broadly applicable and to make the situation better, a sizable investigation is required. Therefore, this study will give future researchers in this subject a solid foundation for their future work and will be very helpful for the decision-makers in the relevant field.
Recommendations
Although the respondents' general level of knowledge was low, many of them had strong knowledge yet displayed poor behavior in real-world situations. Poor knowledge level has been linked to some sociodemographic and professional experience characteristics. In order to improve the situation and generalize the knowledge, a large-scale study is necessary. The general public's awareness and behavior regarding the use of safe dental services should be taken into account by those responsible for developing national health policies. To ascertain the improvement in knowledge of safe dental service seeking practices, the policy maker should develop techniques to gather evidence of the educational interventions provided among patients in dental clinics and hospitals. In health care institutions, including private dental clinics, adequate health education sessions on safe dental service seeking practice should be provided. Patients at all levels of healthcare facilities should have better access to information about infection control procedures. The awareness program should be expanded as much as feasible in the communities because cross infection and associated diseases continue to be a serious problem for developing countries, including Bangladesh.
Recommendations
Although the respondents' general level of knowledge was low, many of them had strong knowledge yet displayed poor behavior in real-world situations. Poor knowledge level has been linked to some sociodemographic and professional experience characteristics. In order to improve the situation and generalize the knowledge, a large-scale study is necessary. The general public's awareness and behavior regarding the use of safe dental services should be taken into account by those responsible for developing national health policies. To ascertain the improvement in knowledge of safe dental service seeking practices, the policy maker should develop techniques to gather evidence of the educational interventions provided among patients in dental clinics and hospitals. In health care institutions, including private dental clinics, adequate health education sessions on safe dental service seeking practice should be provided. Patients at all levels of healthcare facilities should have better access to information about infection control procedures. The awareness program should be expanded as much as feasible in the communities because cross infection and associated diseases continue to be a serious problem for developing countries, including Bangladesh.
Acknowledgement
We strongly acknowledge the study participants and the authority of the study place
References
- Al Subait AA, Alousaimi M, Geeverghese A, Ali El Metwally A. (2016). Oral health knowledge, attitude and behavior among students of age 10–18 years old attending Jenadriyah festival Riyadh: a cross-sectional study. Saudi J Dental Res, 7(1):45-50.
Publisher | Google Scholor - Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day SNdiaye C. (2005). The global burden of oral diseases and risks to oral health. Bull World Health Organ, 83(9):661-669.
Publisher | Google Scholor - Azhar N, Doss JG. (2018). Health‑seeking behaviour and delayedpresentation of oralcancer patients in a developing country:A qualitative study based on the self‑regulatory model. Asian Pac J Cancer Prev, 19:2935‑2941
Publisher | Google Scholor - Dawood OT, Hassali MA, Saleem F, Ibrahim IR, Abdulameer AH. Et al. (2017). Assesment of health seeking behavior and self-medication among general public in state of Penang, Malaysia. Pharm Pract, 15:991.
Publisher | Google Scholor - AlZarea BK. (2017). Dental and oral problem patterns and treatment seeking behavior of geriatric population. Open dent J, 11:230‑236.
Publisher | Google Scholor - Harrel SK, Molinari J. (2004). Aerosols and splatter in dentistry: a brief review of the literature and infection control implications. J Am Dent Assoc, 135(4):429-437.
Publisher | Google Scholor - Karnam RR, Kumar NS, Eshwar S, Deolia S. (2016). Cognitive ability as a determinant of socioeconomic and oral health status among adolescent college students of Bengaluru, India. J Clin Diagn Res, 10: ZC62‑ZC66.
Publisher | Google Scholor - Kahar P. (2019). Patterns of oral hygiene behaviors, daily habits, and caries prevalence in India and Dominican Republic: A comparative study. Indian J Dent Res, 30:87‑93.
Publisher | Google Scholor - Musoke D, Boynton P, Butler C, Musoke MB. (2014). Health seeking behaviour and challenges in utilising health facilities in Wakiso district, Uganda. J Afr Health Sci, 14:1046‑55.
Publisher | Google Scholor - Behere P, Sinha S. (2014). Correlation of global mental health assessment tool (GMHAT‑ PC) in assessment of psychiatric patients as compared to the psychiatrist’s diagnosis in a primary care of central India‑preliminary findings. J Datta Meghe Inst Med Sci Univ, 9:1‑4.
Publisher | Google Scholor - Grover S, Avasthi A, Shah S, Lakdawala B, Chakraborty K. et al. (2015). Indian psychiatric society multicentric study on assessment of health‑care needs of patients with severe mental illnesses. Indian J Psychiatry, 57:43‑50.
Publisher | Google Scholor - Briggs RA. (2019). Normative Theories of Rational Choice: Expected Utility. In: Zalta EN, editor. The StanfordEncyclopedia of Philosophy [Internet]. Fall 2019. Metaphysics Research Lab, Stanford University.
Publisher | Google Scholor - Benzian H, Williams D. (2015). The challenge of oral disease: a call for global action. oral Heal atlas 2nd edGeneva FDI World Dent.
Publisher | Google Scholor - World Health Organization. Oral health [Internet]. 2020 [cited 2020 Sep 14].
Publisher | Google Scholor - Harte JA. (2010). Standard and transmission-based precautions: an update for dentistry. The Journal of the American Dental Association, 141(5):572-81.
Publisher | Google Scholor - Abramson JH. (2011). WINPEPI update; Computer programs for epidemiologists and their teaching potential. Epidemiologic perspectives and innovations, 8:1.
Publisher | Google Scholor - Ehizele A, Chiwuzie J, Ofili A. (2011). Oral health knowledge, attitude and practices among Nigerian primary school teachers. Int J Dent Hyg, 9:254-2560.
Publisher | Google Scholor - Hariharan S, Jonnalagadda R, Gora J. (2006). Knowledge, attitudes and practices of healthcare personnel towards Care-Ethics: A perspective from the Caribbean. Internet J Law Healthcare Ethics, 5:1.
Publisher | Google Scholor - Farsi JMA, FarghalyMM, Farsi N. (2004). Oral health knowledge, attitude and behavior among Saudi school students in Jeddah city. Journal of Dentistry, 32:47-53.
Publisher | Google Scholor - Ehizele AO, Azodo CC, Ehigiator O, Ezeja EB. (2012). Misconceptions about oral health among a group of Nigerian primary school teachers. Nig Dent J, 20:37-40.
Publisher | Google Scholor - Yasmin, R., Gyeltshen, T., & Islam, R. E. (2018). Knowledge, Attitude and Practice of Antibiotics Usage among patients attending OPD of a Dental College Hospital in Dhaka, Bangladesh. Journal of Medicine, 19(2),84-90.
Publisher | Google Scholor - Folabi AO, Akinmoladun VI, Adebose IJ, Elekwachi G. (2010). Self-medication profile of dental patients in Ondo State, Nigeria. Niger J Med, 19:96-103.
Publisher | Google Scholor - Agbor MA, Azodo CC. (2011). Self-medication for oral health problems in Cameroon. Int Dent J. 61:204-209.
Publisher | Google Scholor - Uguru N, Onwujekwe O, Uguru C, Ogu U, Okwuosa C, Okeke C. (2021). Oral health-seeking behavior among different population groups in Enugu Nigeria. PLoS One, 16(2): e0246164.
Publisher | Google Scholor - Banu B, Akter N, Chawdhury SH, Rahim Z, Hossain SM, Zerin FF, Rahman S. (2021). Hygiene behavior among Female Garment Workers: A Pre-COVID-19 Cross-Sectional Study in Bangladesh. Indian Journal of Public Health Research & Development, 12(4).
Publisher | Google Scholor












