

Research Article
Self-care Ability among Elderly Patients with Osteoarthritis
- Sadia Ishfaq
- Bakhtyar Ali Shah
- Muhammad Anwar *
- Shala Arshad
- Asad Ullah
Nursing Officer, Pakistan.
*Corresponding Author: Muhammad Anwar, Nursing Officer, Pakistan.
Citation: Ishfaq S., Bakhtyar A. Shah, Anwar M., Arshad S., Ullah A. (2023). Self-Care Ability among Elderly Patients with Osteoarthritis. Journal of BioMed Research and Reports, BioRes Scientia Publishers. 2(5):1-9. DOI: 10.59657/2837-4681.brs.23.034
Copyright: © 2023 Muhammad Anwar, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 10, 2023 | Accepted: August 23, 2023 | Published: August 30, 2023
Abstract
Objective: The objective of this study was to assess the level of self-care ability and activity of daily living ≥ 60 years’ elderly having osteoarthritis and determine their association with socio demographic variables.
Method: This cross-sectional study was conducted in 2019 in the OPDs of tertiary care hospitals of Peshawar, Pakistan. Total 384 elderly individuals were recruited through consecutive sampling Data were collected through validated questionnaire Self-care items and Activity of daily living. Descriptive statistics like mean, and standard deviation were calculated. Chi square was applied to see an association.
Result: Among the 384 participants of the study, Majority of the patient was 68% of them were females. The mean BMI was 28.37 with a standard deviation ± 4.005. Using the ADL checklist majority of the participants were moderately affected (41.7%) followed by the intact patient (30.7%), while the percentage of highly affected patient were (27.3%). The self-care activities of majority of the participants self-care were poor (71.6%), while the remaining (28.4%) patients were intact. A significant association of self-care ability was found with age, duration of osteoarthritis, type of osteoarthritis, grading of osteoarthritis, income level. Moreover, a significant association was also found between activity of daily living with age, gender, duration of osteoarthritis, type of osteoarthritis, grading of osteoarthritis, marital status with activities of daily living, and residence.
Conclusion: The study found that majority of the patient self-care practices and activity of daily living was poor, while highly significant association was found with socio demographic variables. Therefore, strategies shall be made to work on all those variables which are modifiable to make the life of these patients comfortable.
Keywords: self-care; osteoarthritis; risk factors; quality of life
Introduction
Osteoarthritis is the degenerative disease and chronic musculoskeletal condition of aging that limits the patient’s ability of self-care. Pain due to osteoarthritis caused decreased sleep, isolation and impaired movement specially in elders that makes them difficult to perform daily routine tasks [2,10,11,1,2,3]. With aging water content of cartilage become low that gradually thins the cushion of joints resulting less flexible and prone to degradation and narrowing the joint space. Globally 10 to15% of the world population has osteoarthritis including 9% of men & 18% of women above the age of 60 years [4,5]. The WHO [2003] reported 80% have restricted mobility while 25% were not capable to execute their daily activities [6,7]. Knee osteoarthritis is 4th most prevalent factor of disability among women and 8th in men in the world. [5,6].
Chronic diseases like osteoarthritis negatively affect the individual self-care ability to perform daily activities of life. These activities were affected by degenerative or anatomical and physiological changes occurred in osteoarthritis patients.[8] Self-care ability is the practice of activities that individuals initiate on their own behalf in maintain promote, restore or improve health and well-being [9, 1]. Individual would be able to utilize his physical energy which is sufficient for execution of self-care operations [10]. According the WHO, self-care activities are undertaken by lay people on their own behalf, either separately or in participative collaboration with professionals [11, 12].
Self-care is effectively learned throughout life by interaction within physical, psychological, emotional realities. Self-care is shaped by values and beliefs learned in specific culture and elder’s experiences [2, 13]. Losing self-care ability means losing independent care that affects individual quality of life. Elderly’s need in illness and health reflected in their developmental stage. Weakened physically [pain in chronic diseases impacts on ADL], psychologically [depression, fear, anxiety], emotionally [demotivated to strive healthy, poor decision making] socially [loneliness] culturally impact on level of self-care ability resulting poor health maintenance, deficit in self-care activities and disability in geriatric population [3, 12, 8].
Health promotion is significant factor for active aging that makes people to control themselves in order to improve their health. For implementing self-care activities, one should have knowledge about self-care [5]. [10] One of the Chinese studies declared disease rate of elder population were. greater than rest of population in term of chronic diseases with physical and mental in- capabilities of elders that further leads to decline in ability to do their self-care by themselves [1, 11].
Numerous studies have proven about progression of illness impact on self–care activities in later stage of life [10, 12, 15]. Most prevalent illnesses among Pakistani elders are hypertension, diabetes and arthritis. [16] Chronic conditions like osteoarthritis adversely influenced on activities of daily living [ADLs] and instrumental activities of daily living [IADLs] that make the person dependent and disable [2,15]. This study endeavored to expanded nurse’s knowledge and their understanding regarding self-care practices. This study attempted to investigate the level of self-care ability among elder patients having osteoarthritis, and take action according to the level of deficit in self-care.
Methodology Materials and method
This Study was conducted in Out Patient Departments (OPDs) of orthopedic units of Hayatabad Medical Complex, Khyber Teaching Hospital and Lady Reading Hospital Peshawar using cross-sectional study design. The study population was elder patient’s ≥ 60 years having bilateral osteoarthritis at least from last 6 months. This Study was conducted from May 2019 to October 2019. Sample Size was calculated through open Epi calculator, with 5% margin of error and 95% CI. Sample size was calculated on the prevalence of self-care ability that was 50%. After calculation of the sample size came to be three hundred and eighty-four (384) patients Risk of drop out was 10%, using consecutively sampling technique.
The inclusion criteria for this study were: All patients (Male and Female) who were ≥ 60 years, and Patients who had bilateral osteoarthritis at least from last 6 months. While patient who were cognitively impaired, unconscious. unwilling to participate, paralyzed patients and had language barrier were excluded from the study.
Study Tool
The data were collected from the patients through pre-tested and validated two questionnaires. The questionnaire consisted of two parts; demographic variables and statements against Likert and dichotomous scale. Demographic variables have been put according to the need and nature of the study. The questionnaire which was about self-care ability and daily activities of osteoarthritis patients was used to determine the extent of self-care ability among elderly patients. Primary questionnaire “self-care items” has been taken from Iranian study among the elder patients having Osteoarthritis which was designed by Gerayllo, S. and Karimiankakolak, Z (2015). Formal permission has been taken from the author of Questionnaire “Self-care” through email. Osteoarthritis Self-care items consisted of 12 items on 5-points Likert type scale 1 for not at all, 2 for, seldom; 3 for sometimes, 4 for often and 5 for always. On the basis of median (30), two categories were made less than 30 and more than 30, whose responses were <30>30 represented decreased self-care ability [17].
Another questionnaire was Content of this questionnaire was Activities of Daily Living (ADLs) that consisted of 19 items on dichotomous scale reliable with an average Chronbach Alpha “0.79”. This questionnaire has four major dimensions of activities which was designed by Stamm et al. Statements of this questionnaire shown having or no deficit in activities of daily living regarding osteoarthritis patients. In the validated questionnaire; Activities of Daily Living, initial seven questions YES indicated “1” show increased self-care ability while “NO” indicated “0” decreased self-care ability. From eighth question to onwards it becomes in reversed order “NO” indicated “1” no deficit in self-care ability while YES indicated “0” having deficit in self-care ability. According to this study, different ranges in above mentioned questionnaire from elder are responses for Activities of Daily Living. These ranges show increased or decreased self-care ability by following categories; highly affected self-care ability 0-6, while moderately affected 7-13 and intact showed by14-19 [15].
Data Collection Procedure
In this cross-sectional study, all patients who had osteoarthritis and came to (OPDs) of orthopedic units of Hayatabad Medical Complex, Khyber Teaching Hospital and Lady Reading Hospital Peshawar were consecutively selected.
Questionnaire has been translated into Urdu and question’s relevance and translation has been validated by educational experts. Self-care ability was measured through the patient’s responses to the questionnaire. Structure of questionnaire depicted its intactness and having deficit among osteoarthritis patients.
Data Analysis
Data were analyzed through Statistical Package for Social Sciences (SPSS) version 22. In descriptive statistics mean and standard deviations were calculated for continues data whereas percentages were calculated for categorical data. In inferential statistics chi square was applied to see any significant association between outcome variables i.e., activities of daily living, self-care ability and demographic variables.
Ethical Considerations
Current study has been approved by Graduate Committee of the Institute of Nursing Sciences at Khyber Medical University, Advanced Studies and Research Board (ASRB), Khyber Medical University (KMU) and Ethics board Committee of KMU. For data collection, permission was taken from nursing directors of respective hospitals and Ethical Committee Review Board of Hayatabad Medical Complex Peshawar as well. The study participants were informed about the study through written paper that included questionnaire; participants were guaranteed confidentiality and anonymity. Operational meaning of the terms used in the study was explained to the participants.
Results
Demographic data of the patients
Data of the current study collected from 385 participants in orthopedic OPD of three tertiary care hospitals of KPK. Out of 385, 130 were from HMC, 130 were from LRH and the rest of participants were from KTH. The number of female participants was higher (68%) compared to male, the age group 60-70 years was in majority (82.03%), while married patient was also high (87.7%) compared to single patients (see table 1).
Table 1: Demographic data of the participants
| Frequency n=384 | Percentage | ||
| Gender | Male | 123 | 32% |
| Female | 261 | 68% | |
| Age | 60 – 70 Years | 315 | 82.03 % |
| 71- 80 Years | 45 | 11.71 % | |
| >80 Years | 24 | 6.25 % | |
| Residence | Rural | 245 | 63.8% |
| Urban | 139 | 36.2 % | |
| Marital status | Married | 337 | 87.76% |
| Single | 47 | 12.23% | |
| Income level | 10,000 - 20,000 | 63 | 16.40% |
| 21,000 - 40,000 | 190 | 49.47% | |
| 41,000 - 60,000 | 96 | 25% | |
| > 60,000 | 35 | 9.11% | |
| Occupation | Housewives | 229 | 59.63% |
| Farmer/Gatekeeper/Labor | 47 | 12.23% | |
| Shopkeeper | 32 | 8.33% | |
| Retired | 43 | 11.19% | |
| Employed | 24 | 6.25% | |
| Jobless | 9 | 2.3% | |
| Level of Education | Illiterate | 239 | 62.2% |
| 1 - 10 grades | 69 | 18.0 % | |
| > 10 grades | 76 | 19.8% | |
| Family History | Yes | 152 | 39.58% |
| No | 232 | 60.41% | |
| Duration of OA | 6 months - 2 years | 154 | 40.1 % |
| > 2 years | 230 | 59.9% | |
| Type of Arthritis | Bilateral knee | 229 | 76.04% |
| Bilateral Knee & Hips | 16 | 4.16% | |
| Bilateral Knee +Hands | 32 | 8.33% | |
| Bilateral Knee +Spine | 11 | 2.86% | |
| Bilateral Hands | 8 | 2.08% | |
| Spine | 8 | 2.08% | |
| Knee + others | 17 | 4.42% | |
| Grading | Grade I | 118 | 30.72% |
| Grade II | 151 | 39.32% | |
| Grade III | 90 | 23.43% | |
| Grade IV | 25 | 6.51% | |
| Height | Mean and SD | 163.16 ± 8.38 cm | |
| Weight | Mean and SD | 75.20 ± 9.41 kg | |
| BMI | Mean and SD | 28.37 ± 4.00 | |
Activity of daily living scores
Table 2 explains the activity of daily living score of the participants that were responded in the form of Yes and No by the arthritis patients (see table 2).
Table 2: Activity of daily living score of the participants.
| SN | Items | YES | NO |
| 1 | Are you able to walk without walking aids for 500 m? | 239 (62.2%) | 145 (37.8%) |
| 2 | Are you able to climb stairs up and down without walking aids? (Walking aids here included also the use of side rails) | 129 (33.6%) | 255(66.4%) |
| 3 | Can you use your fingers to grab and use small things like a pencil without problems? | 335 (87.2%) | 49 (12.8%) |
| 4 | Can you turn on a tap without problems? | 340 (88.5%) | 44 (11.5%) |
| 5 | Are you able to stretch your hand that you can shake hands without problems? | 336 (87.5%) | 48 (12.5%) |
| 6 | Are you able to bend or kneel down without problems? | 42 (10.9%) | 342 (89.1%) |
| 7 | Are you able to lift and carry a shopping bag with 5 kg without a problem? | 227 (59.1%) | 157 (40.9%) |
| 8 | Do you usually have any problem to eat independently? | 81 (21.1%) | 303 (78.9%) |
| 9 | Do you usually have any problem to sit down on the bed or on a chair and stand up without help? | 221 (57.6%) | 160 (41.7%) |
| 10 | Do you usually have problems to put on or take off clothes? | 219 (57%) | 165 (43%) |
| 11 | Do you usually have problems to go to toilet? (Sit down and get up from the toilet, keep clean or manage a urinary catheter, urostomy, or colostomy)? | 198 (51.6%) | 186 (48.4%) |
| 12 | Do you usually have any problems to take a bath or shower? | 212 (55.2%) | 172 (44.8%) |
| 13 | Do you usually have problems to prepare your food independently? | 178 (46.4%) | 206 (53.6%) |
| 14 | Do you usually have problems to use your telephone independently? | 56 (14.6%) | 328 (85.4%) |
| 15 | Do you usually have problems to manage your shopping independently? | 253 (65.9%) | 131 (34.1%) |
| 16 | Do you usually have problems to wash clothes independently? | 268 (69.8%) | 116 (30.2%) |
| 17 | Do you usually have problems to do light house work independently? | 175 (45.6%) | 209 (54.4%) |
| 18 | Do you usually have problems to do some times heavy house work independently? eg. for heavy house work were sliding heavy furniture, cleaning, washing up the floor). | 364 (94.8%) | 20 (5.2%) |
| 19 | Do you usually have problems to manage your financial affairs independently? (Included withdrawal money/filling in a payment form). | 156 (40.6%) | 228 (59.4%) |
Overall Activity daily living score of the participants
Figure 1 shows that majority of the participants were moderately affected (41.7%) followed by the intact patient (30.7%), while the percentage of highly affected patient were (27.3%) (see figure 1).
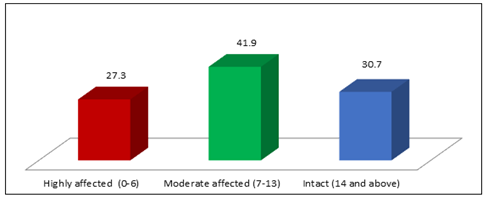
Figure 1: ADL Score of the participants
Participants Responses Regarding Self Care Items
Table 3: illustrates the self-care analysis of the participants (see table 3).
| SN | ITEMS | Not at all N% | Seldom N% | Sometimes % | Often % | Always % |
| 1 | Using Suitable shoes | 148 (38.5%) | 55 (14.3%) | 41 (10.7 %) | 42 (10.9%) | 98 (25.5%) |
| 2 | Taking medication regularly according to doctor order | 2 (5%) | 42 (10.9%) | 211 (54.9%) | 35 (9.1%) | 94 (24.5%) |
| 3 | Seeing a doctor regularly | 83 (21.6%) | 113 (29.4%) | 92 (24.0 %) | 36 (9.4%) | 60 (15.6%) |
| 4 | Praying in a sitting status | 68 (17.7%) | 90 (23.4%) | 20 (5.2%) | 54 (14.1%) | 152 (39.6%) |
| 5 | Avoiding use of squat toilet | 122 (31.8%) | 12 (3.1%) | 7 (1.8%) | 47 (12.2%) | 196 (51.0%) |
| 6 | Doing rest if needed | 1 (3%) | 27 (7.0%) | 69 (18%) | 119 (31%) | 168 (43.8%) |
| 7 | Using sofa or chair for sitting | 9 (2.3%) | 34 (8.9%) | 33 (8.6%) | 87 (22.7%) | 221 (57.6%) |
| 8 | Avoiding long time standing | 55 (14.3%) | 68 (17.7%) | 43 (11.2%) | 79 (20.6%) | 139 (36.2%) |
| 9 | Doing recommended exercises | 276 (71.9%) | 69 (18.0%) | 20 (5.2%) | 15 (3.9%) | 4 (1.0%) |
| 10 | Asking for help from family and friends | 15 (3.9%) | 42 (10.9%) | 62 (16.1%) | 93(24.2%) | 172 (44.8%) |
| 11 | Using cane during walking | 247 (64.3%) | 46 (12%) | 25 (6.5%) | 21(5.5%) | 45 (11.7%) |
| 12 | Going for swimming | 383 (99.7%) | _ | _ | 1(0.3%) | _ |
Overall self-care score of the participants
Figure 2 shows that majority of the participants self-care was poor (71.6%), while the remaining (28.4%) patients were intact (see figure 2).
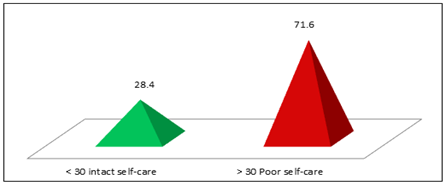
Figure 2: Self-care score of the participants
Association of ADL and self-care with selected demographic variables
A significant association of self-care ability was found with age, duration of osteoarthritis, type of osteoarthritis, grading of osteoarthritis, income level. Moreover, a significant association was also found between activity of daily living with age, gender, duration of osteoarthritis, type of osteoarthritis, grading of osteoarthritis, marital status with activities of daily living, and residence (see table 4).
Table 4: Association of ADL and self-care with selected demographic variables.
| Percentage | ADL P-Value | Self-care P-Value | ||
| Gender | Male | 32% | 0.001 | 0.086 |
| Female | 68% | |||
| Age | 60 – 70 Years | 82.03 % | 0.001 | 0.001 |
| 71- 80 Years | 11.71 % | |||
| >80 Years | 6.25 % | |||
| Residence | Rural | 63.8% | 0.004 | 0.003 |
| Urban | 36.2 % | |||
| Marital status | Married | 87.76% | 0.024 | 0.820 |
| Single | 12.23% | |||
| Income level | 10,000 - 20,000 | 16.40% | 0.003 | 0.042 |
| 21,000 - 40,000 | 49.47% | |||
| 41,000 - 60,000 | 25% | |||
| > 60,000 | 9.11% | |||
| Occupation | Housewives | 59.63% | 0.004 | 0.006 |
| Farmer/Gatekeeper/Labor | 12.23% | |||
| Shopkeeper | 8.33% | |||
| Retired | 11.19% | |||
| Employed | 6.25% | |||
| Jobless | 2.3% | |||
| Level of Education | Illiterate | 62.2% | 0.119 | 0.353 |
| 1 - 10 grades | 18.0 % | |||
| > 10 grades | 19.8% | |||
| Family History | Yes | 39.58% | 0.60 | 0.843 |
| No | 60.41% | |||
| Duration of OA | 6 months - 2 years | 40.1 % | 0.001 | 0.001 |
| > 2 years | 59.9% | |||
| Type of Arthritis | Bilateral knee | 76.04% | 0.001 | 0.001 |
| Bilateral Knee & Hips | 4.16% | |||
| Bilateral Knee +Hands | 8.33% | |||
| Bilateral Knee +Spine | 2.86% | |||
| Bilateral Hands | 2.08% | |||
| Spine | 2.08% | |||
| Knee + others | 4.42% | |||
| Grading | Grade I | 30.72% | 0.001 | 0.001 |
| Grade II | 39.32% | |||
| Grade III | 23.43% | |||
| Grade IV | 6.51% | |||
Discussion
Present study has shown that the mean BMI were 28.37± 4.005; most of study participants were females i.e., (68%) among them, (59.63%) were housewives, more than half participants were illiterate (62.2%) whereas Iranian study brought similar finding which was conducted on 87 older individuals, found the mean BMI of respondents were 28.37±4.4, while (88.6%) were female, (57.6%) were illiterate, (74.4%) were housewives [17]. Result of this study indicated that 62.2 % older individuals were able to walk without walking aids for 500 meters. A study from Austrian found significant finding 32.3% aged people having osteoarthritis were able to walk without walking aids for 500 meters. Previous studies bared the fact that regular physical activities or moderate level exercises not only decreased the level of dependency, pain and disability among older patients of osteoarthritis but also increased muscle strength, flexibility resulting in low prevalence of chronic diseases [18-20]. Systematic review revealed that older with knee osteoarthritis were less likely to follow recommendation for physical activity 10.2 minutes/day (P=0.011) than without osteoarthritis in six European countries [21]. Moreover, Nott off and his colleagues emphasized on physical activity that it enhances life expectancy by 0.68 years worldwide [22].
Furthermore, detail analysis revealed that daily living (18.8%) was highly affected while (44.1%) was moderately affected elders who had bilateral knee osteoarthritis. Moreover, (4.1%) patients having bilateral knee with hip osteoarthritis also caused disability in old age. Consistent findings of existent research with American studies have been found in term of severity of disease by Kellgren and Lawrence radiographic classification. Creamer, P and his fellow’s notified grade I (16.1%), grade II (33.9%), grade III (33.9%) and grade IV (16.1%) in knee osteoarthritis [23]. Additionally, present study also found those elderly whose job required kneeling, squatting and prolong standing or heavy lifting stuff getting knee and hip osteoarthritis. Prior literature supported the findings of present study regarding individuals whose occupation entailed kneeling, squatting or loading for longer period of time resulting worsening of knee and hip osteoarthritis [24, 19]. whereas people who were mostly engaged in manual dexterity having hand osteoarthritis [25].
In current study’s finding regarding management of shopping independently; 65.9% older reported that they had problem. Contrary, only 15.1% elderly with osteoarthritis in Austrian study facing problem to manage shopping freely. In Pakistan specially Pashtun culture mostly women were not working outside, specifically females of rural areas were confined to their homes and not permitted to go for shopping or getting grocery from market. Literature revealed that similar findings where 48% disabled were unable to perform daily works specifically higher risk were found in aged females [1]. Existent study found (59.63%) sedentary life style was in line with global studies that have been conducted across six European countries. Aged people with knee osteoarthritis found in the United Kingdom (UK) and Spain [21]. had walked for short period of time comparatively without osteoarthritis which has shown strong association between inactivity or sedentary life style with progression of knee osteoarthritis [19,18].
Author of existent study has found exclusively 94.8% older faced problems in doing heavy housework, in contrast Austrian study declared that 34.6% older faced problems in doing heavy house work [9]. However, supported by previous researchers that heavy work for four hours/day by geriatrics increase risk of knee osteoarthritis [25].
Author of present study surprisingly noticed that out of 261 females only 3 subjects were able to do exercises on regular basis while (9) women did often. Findings of local research on elderly females having osteoarthritis depicted 30% subjects exercised daily were comparatively high percentage with existent study (1%) which also indicated lack of knowledge about exercise laid influence on progression of osteoarthritis [26] Furthermore, Asian study declared 26.5% elder patients with osteoarthritis exercised daily [27]. Regarding self-care item, it has been identified that among (118) elders with grade I only (1) subject always used cane during walking whereas among (151) elders with grade II few of them (8) subjects always used cane while among (90) elders with grade III only (15) subjects always used cane. Author of present study has noticed that elderly patients were reluctant to use cane during walking. They felt shy and it created feeling of disability among them. In Iranian study11.5% respondents have used cane during walking. Existent study declared through self-care item among (292) elders of bilateral knee osteoarthritis (110) always prayed in sitting position while among (16) elderly having bilateral knee with hip osteoarthritis (14) always prayed in sitting position. It is evident from literature that 82.2% patients always prayed in sitting position [27].
In this context, it has been identified through “self-care item” among 384 geriatrics; 71.6% have shown poor ability to self-care whereas in “activities of daily living”; 27.3% subject’s activities of daily living were highly affected while 41.9% were moderately affected. Furthermore, 50
References
- Prior Y. (2013). An epidemiological study of self-care restriction and joint pain in community-dwelling older people.
Publisher | Google Scholor - Koç Z. (2015). The investigation of factors that influence self-care agency and daily life activities among the elderly in the northern region of Turkey. Collegian, 22(3):251-258.
Publisher | Google Scholor - Baird C. (2003). self-caring of women with osteoarthritis living at different levels of independence. Health care for women Int, 24(7):617-634.
Publisher | Google Scholor - Ashiq U,Amir ZA. (2017). The rising old age problem in pakistan. J Res Soc Pakistan, 54(2).
Publisher | Google Scholor - Jahan I, Sima S H, Khalil M, Sohel MD, Hassan MH. (2017). Survey on prevalence, risk factors and treatment pattern of osteoarthritis in Bangladesh: retrospective study, 7(4).
Publisher | Google Scholor - Patel S, Heine PJ, Ellard DR, Underwood M. (2016). Group exercise and self-management for older adults with osteoarthritis: a feasibility study, 17(3):252-264.
Publisher | Google Scholor - Zhang Y, Niu J. (2016). Editorial: Shifting gears in osteoarthritis research toward symptomatic osteoarthritis. arthritis rheumatoly (Hoboken, NJ), 68(8):1797.
Publisher | Google Scholor - McDonough CM, Jette AM. (2010). The contribution of osteoarthritis to functional limitations and disability. Clin Geriatr Med, 26(3):387-399.
Publisher | Google Scholor - Guo L, Zauszniewski JA, Ding X, Zhang L, Gao H, Guo Q, et al. (2017). The Appraisal of Self-Care Agency Scale-Revised (ASAS-R): Reliability and Validity Among Older Chinese People. Western journal of nursing research, 39(11):1459-1476.
Publisher | Google Scholor - Sundsli K, Söderhamn U, Espnes GA, Söderhamn O. (2014). Self-care telephone talks as a health-promotion intervention in urban home-living persons 75+ years of age: A randomized controlled study.Clinical Intervention in Aging, 9:95-103.
Publisher | Google Scholor - Nelson-McEvers JA. (1995). Measurement of Self-Care Agency in a Noninstitutionalized Elderly Population.
Publisher | Google Scholor - Wiebe VM. Examining self-care among the elderly using orems self care framework.
Publisher | Google Scholor - Koirala J. The knowledge and practices of self-care capabilities among geriatric population. Int J Biochem Physiol, 4(1):1-9.
Publisher | Google Scholor - Sullivan TJ, Munroe DJ. (1986). A self‐care practice theory of nursing the elderly. Educ Gerontol, 12(1):13-26.
Publisher | Google Scholor - Stamm TA, Pieber K, Crevenna R, Dorner TE. (2016). Impairment in the activities of daily living in older adults with and without osteoporosis, osteoarthritis and chronic back pain: a secondary analysis of population-based health survey data. BMC musculoskelet disorder, 17(1):139.
Publisher | Google Scholor - Qidwai W. (2009). Ageing population: status, challenges and opportunities for health care providers in Pakistan Vol. 19, Journal of the College of Physicians and Surgeons Pakistan.
Publisher | Google Scholor - Gerayllo S, Karimiankakolaki Z. (2015). Self-care activities and behavioral intention toward self-care in older adults suffering from knee osteoarthritis in Yazd, Iran. Elder Heal J, 1(1):36-41.
Publisher | Google Scholor - Chmelo EA, Nicklas B, Berry M, Davis C, Legault C, Miller G. (2010). physical activity habits in older adults with knee osteoarthritis.
Publisher | Google Scholor - Garver MJ, Focht BC, Taylor SJ. (2015). Integrating lifestyle approaches into osteoarthritis care. J Multidiscip Healthc, 8:409-418.
Publisher | Google Scholor - Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. (2007). Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association, 39(8):1423-1434.
Publisher | Google Scholor - Herbolsheimer F, Schaap LA, Edwards MH, Maggi S, Otero A, Timmermans EJ, et al. (2016). Physical Activity Patterns Among Older Adults With and Without Knee Osteoarthritis in Six European Countries. Arthritis Care & Research, 68(2):228-236.
Publisher | Google Scholor - Notthoff N, Reisch P, Gerstorf D. (2017). Individual Characteristics and Physical Activity in Older Adults: A Systematic Review. Gerontology, 63(5):443-459.
Publisher | Google Scholor - Creamer P, Lethbridge-Cejku M, Hochberg MC. (2000). Factors associated with functional impairment in symptomatic knee osteoarthritis. Rheumatology, 39(5):490-496.
Publisher | Google Scholor - Palazzo C,Nguyen C, Lefevre-Colau M-M, Rannou F, Poiraudeau S. (20163).Risk factors and burden of osteoarthritis. Ann Phys Rehabil Med, 59(3):134-138.
Publisher | Google Scholor - Zhang Y, Niu J, Kelly-Hayes M, Chaisson CE, Aliabadi P, Felson DT. (2002). Prevalence of symptomatic hand osteoarthritis and its impact on functional status among the elderly: The framingham study. American Journal of epidemiology, 156(11):1021-1027.
Publisher | Google Scholor - Saeed F, Humayun A, Fatima SM, Junaid V, Imtiaz H, Zehra M, et al. (2019). The Pressing need to raise awareness about osteoarthritis care among elderly females in Pakistan: A Cross-sectional Study. Cureus, (8):1-9.
Publisher | Google Scholor - Gerayllo S, Karimiankakolaki Z. (2015). Self-care activities and behavioral intention toward self-care in older adults suffering from knee osteoarthritis in Yazd, Iran. Elder Heal J, 1(1):36-41.
Publisher | Google Scholor - Morrongiello BA, Gottlieb BH. (2000). Self-care among older adults. Candian Journal on Aging/ La Revue Can du Vieil, 19(S1):32-57.
Publisher | Google Scholor













