

Case Report
Rickets Secondary to Distal Renal Tubular Acidosis: A Case Report
1Professor Emeritusat University of Medicine 2, Yangon. Consultant Endocrinologist at Grand Hantha International Hospital, Yangon, Myanmar.
2Consultant Endocrinologist, Department of Endocrinology, North Okkalapa Generaland Teaching Hospital, University of Medicine 2, Yangon, Myanmar.
3Senior MedicalOfficer at Grand Hantha International Hospital, Yangon, Myanmar.
*Corresponding Author: Kyaw Swar Thet, Senior Medical Officer at Grand Hantha International Hospital, Yangon, Myanmar.
Citation: Than T. Aye, K.N.S. Myint, Kyaw S. Thet. (2024). Rickets Secondary to Distal Renal Tubular Acidosis: A Case Report. International Clinical Case Reports and Reviews, BioRes Scientia Publishers. 2(1):1-5. DOI: 10.59657/2993-0855.brs.24.008
Copyright: © 2024 Kyaw Swar Thet, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 22, 2024 | Accepted: May 08, 2024 | Published: May 20, 2024
Abstract
Rickets is a common condition that affects pediatric patients and is usually secondary to a nutritional deficiency of vitamin D. However, there are also some rare types of rickets that are seen as secondary to renal defects. These types include distal renal tubular acidosis (dRTA), proximal renal tubular acidosis (pRTA), vitamin D-dependent rickets, and hypophosphatemic rickets. Among these causes, hypercalciuria and phosphate wasting are common in distal RTA due to bone resorption, which increases as a buffer against metabolic acidosis. This can result in intractable rickets. Early diagnosis and management are required in these cases. Here, we present the case of a 14-year-old girl who came to us with difficulty walking, failure to thrive, polyuria, hypokalemia, and bone changes. Eventually, the patient was found to have rickets secondary to distal renal tubular acidosis.
Keywords: RTA; rickets
Introduction
Renal tubular acidosis results from the impairment of tubular acid transport in the kidneys. The distinguishing characteristics of renal tubular acidosis include a normal anion gap and hyperchloremic metabolic acidosis [1]. There are three types of renal tubular acidosis: Distal RTA (Type I), Proximal RTA (Type II), and aldosterone insensitivity (Type IV). Distal RTA is characterized by the failure of H+ secretion in the distal nephron [2]. This failure to secrete H+ ions is primarily responsible for the inability to acidify the urine to an acidic pH. Since the excretion of H+ ions by the kidneys are the main mechanism for eliminating them from the body, impaired H+ excretion leads to acidosis. Untreated cases of RTA often result in rickets due to the leaching of minerals from the bones in an attempt to buffer the acidosis. Acidosis increases bone resorption by osteoclasts [3]. RTA can manifest in children with various presentations, including failure to thrive, growth retardation, vitamin D-resistant rickets (VDDR), polyuria, hypokalemia, and nephrocalcinosis/nephrolithiasis (only in Type I) [4].
Case presentation
A 14-year-old girl from a remote area of Rakhine district of Myanmar was referred to the Endocrine clinic of a private hospital in Yangon with a possible diagnosis of rickets. Her parents noticed difficulty in walking and standing since she was 5 years old. Her symptoms have progressively worsened, with her legs bending at the knees since the age of 8, requiring support for walking. This weakness has prevented her from attending school for the past 2 years. She was born full-term, breastfed, and had a normal perinatal history and developmental milestones (social, motor, and verbal). She is currently attending 8th Standard. She denies any abnormalities in tooth formation, tetany, or convulsions, although she experiences aches and pains throughout her body most of the time.
She has one elder sister who does not have similar problems. She has not yet started her menarche and shows no secondary sex characteristics. On examination, she exhibits short stature and height of 110 cm (- 6 SD for age and sex), and her body weight is only 15 kg (-3 SD for age and sex). The patient has obvious genu valgum (refer to figure 1), widening of the ankle joint (refer to figure 1, b), and a rickety rosary (refer to figure 1, c).
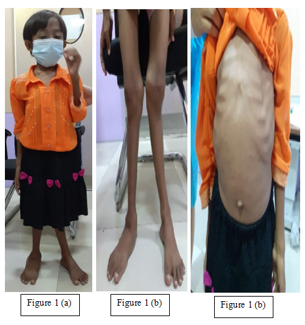
Figure 1: Patient presenting with short stature (a), genu valgum, widening of ankle joint (b) and rickety rosary(c).
She is able to walk only for short distance and needed support to stand, most of the time she had to depend on care giver to walk.
Table 1: biochemical Investigations
| Test | At presentation | Recheck tests |
| Urea | 22 | 20 |
| Na | 136 | 139 |
| K | 2.4 | 2.9 |
| Cl | 110 | 111 |
| HCO3 | 16 | 18 |
| Anion gap | 12.4 | 12.9 |
| Albumin | 4.5 | |
| Cr mg/dl | 0.5 | |
| Mg | 2.8 | |
| PO4 mg/dL(2.5-4.5) | 2.4 | 0.77 |
| PTH (15-65)pg/ml | 34.53 | 17.22 |
| Alkaline Phosphate | 1075 | 937 |
Investigations showed persistence hypokalemia, metabolic acidosis and good renal function.
Urinalysis showed pH- 7.5, SG – 1.003, pH more than 5.5 in presence of hyperchloraemic metabolic acidosis.
Vitamin D was 87.59 nmol/L (normal range 50- 125 nmol/L), 1, 25 dihydroxy Vit D3 was 91 pg/ml (normal range 24-86 pg/ml) and exclude the vitamin D dependent rickets.
Thyroid function and pituitary function tests are normal.
Table 2: urinary excretion of calcium, phosphate and urine anion gap
| Sport Urinary Ca (2.50 to 7.50) | Urinary PO4 24 hr | S: CR μmol/L | U: Cr mmol/L | S: Pi mmol/L | U: Pi mmol/L | |
| 2.2 mg/dL | 12.1 mmol (15-50) | 32 | 1 | 0.6 | 1.45 | |
TRP 92.27% TmP/GFR = 0.6 mmol (0.91 -1.23 for 13 – 15 year) | ||||||
Urinary Ca 24 hr (100-300) mg/day | Urinary K 24 hr (25-125) mmol/L | Urinary Creatinine (720-1510) mg/day | Urinary Chloride mmol/day | Urinary Na | ||
| 286 (> 4mg/kg/day) | 33 mmol/day | 298 | 105 | 133 | ||
Hypercalciuria can be diagnosed when 24-hr calcium excretion exceeding 4 mg/kg/day [5]. Calculated urine net charge (anion gap) was 61 which is higher than urinary chloride level.
Special laboratory tests
FGF 23 Gene by PCR amplification and direct DNA sequencing test revealed no pathogenic FGF 23 mutation is detectable and FGF 23 level was less than 14 (reference less than 52).
Imaging results
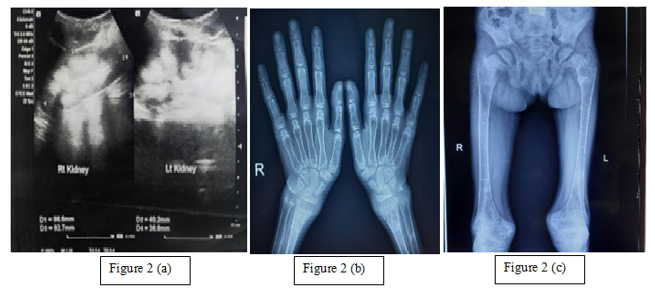
USG Abdomen showed deposition of calcium are seen in medulla of the both kidney and Bilateral renal medullary nephrocalcinosis (Figure 2, a). X ray both leg AP and both knee joint showed generalized osteopenia is noted. Splaying and cupping of metaphysis and more evident knee joints, Triradiate pelvis noted. Stress fracture at left side lower third of shaft of femur, lesser trochanter and proximal tibia (Figure x2, b). X ray Hand (AP & oblique) showed metaphyseal fraying and cupping noted. Widening of growth plates noted. Stress fracture noted at distal radius noted on both sides (Figure 2, c).
X ray Lumbar spine (AP & lateral) showed reduced curvature and slight scoliosis noted and finding likely due to paravertebral muscle spasm, there was generalized osteopenia with mild biconcave vertebral changes, with concomitant medullary nephrocalcinosis noted at bilateral kidneys (Figure 4).
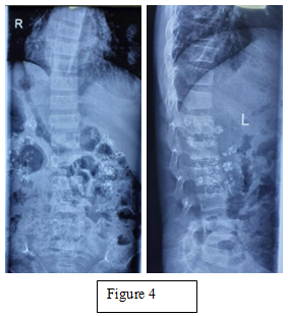
Table 3: Follow up improvement of the patient
| Height (cm) | Weight (kg) | K (mmol/L) | HCO3 | Phosphate | Alkaline Phosphatase | |
presentation (pre- treatment) | 110 | 15 | 2.9 | 16 | 2.4 | 1075 |
4 months (Post- treatment) | 115 | 20 | 3.8 | 24 | 2.9 | 1030 |
| 8 months later | 121 | 22.7 |
After the alkali treatment, the patient able to stand, walk and can do normal daily activities. After treatment, her height raised 10 cm and gained 7.7 kg from baseline. High alkaline phosphatase level may be due to her recent fracture and healing stage at the time of blood test.
Discussion
The possible differential diagnoses of rickets in this child include vitamin D deficiency (nutritional rickets), vitamin D-dependent rickets, renal tubular acidosis, and hypophosphatemic rickets. Typically, the serum concentration of parathyroid hormone (PTH) is elevated in calcipenic rickets, but PTH concentrations are usually normal or slightly elevated in phosphopenic rickets [6]. Normal levels of serum calcium, 25-OH-D, and parathormone effectively ruled out nutritional rickets in this child, but there may still be abnormalities in vitamin D metabolism or vitamin D resistance. However, the level of 1,25 dihydroxy Vit D3 is just above the upper normal limit, which also rules out Vitamin D-dependent Rickets types 1 and 2.
In the presence of hypophosphatemia, the tubular reabsorption of phosphate (TRP) was calculated to be 92.27% (85 - 95%), indicating no phosphate wasting. However, TRP is not reliable for excluding renal phosphate wasting because it does not account for the amount of filtered phosphate. In fact, TRP can falsely appear normal even in the presence of renal phosphate wasting. To account for the amount of filtered phosphate, the measurement of TmP/GFR (the ratio of tubular maximum reabsorption of phosphate to glomerular filtration rate) can be used [4]. A reduced TmP/GFR value of 0.6 mmol (0.91 - 1.23 for 13 - 15 years) indicates some renal wasting of phosphate.
The next step is to measure the level of intact fibroblast growth factor 23 (FGF23) in the presence of renal phosphate wasting, which was not high (less than 14 pg/ml, reference less than 52). Circulatory FGF23 is elevated in all forms of hypophosphatemic rickets except for hereditary hypophosphatemic rickets with hypercalciuria (HHRH). This rule out hypophosphatemic rickets.
Renal tubular acidosis (RTA) occurs when the kidneys are unable to maintain a normal plasma acid-base balance due to defects in tubular function, specifically in either acid excretion or bicarbonate ion reabsorption [7]. Hypercalciuria and hyperphosphaturia may also develop as a result of the release of calcium phosphate from the bones to counteract excess hydrogen ions during acidosis, as well as the direct effects of acidosis on tubular reabsorption of these ions [5].
Additionally, chronic hypokalemia can cause various pathological changes in renal proximal tubular cells, leading to secondary proximal tubulopathy. In distal RTA, phosphate depletion caused by secondary tubulopathy can be completely normalized by correcting acidosis using alkali solutions [4].
For the diagnosis of renal tubular acidosis (RTA), the initial step involves determining the plasma anion gap. RTA leads to a normal anion gap range of 8-12 mEq/L, which is attributed to hyperchloremic metabolic acidosis, as observed in our patient.
The subsequent step is assessing the fasting urinary pH. In the presence of systemic metabolic acidosis, a urinary pH higher than 5.3 indicates defective hydrogen ion H+ secretion, pointing towards distal RTA [8]. This is followed by the calculation of the urinary anion gap (urinary anion gap UAG = UNa + UK+ - UCl-). The urine anion gap is an indirect measurement of the urinary ammonia excretion in response to metabolic acidosis. A consistently positive anion gap, in the presence of metabolic acidosis, indicates a renal acidification defect [9]. Under normal circumstances, the UAG is positive due to the presence of dissolved anions. Metabolic acidosis with normal mechanism of renal acidification causes the UAG to become negative due to an increase in the NH4+ synthesis and excretion with the Cl- ion. Therefore, in patients with hyperchloremic metabolic acidosis with preserved mechanism of renal acidification a negative UAG implies adequately increased NH4 + excretion. Whereas a positive UAG indicates inappropriately low renal NH4+ excretion, which was seen in RTA [5]. In distal RTA (type 1), a positive urinary anion gap within 24 hours exceeds the urinary chloride level. In our case, in the presence of systemic metabolic acidosis, a urinary pH higher than 5.3 and the urine net charge (anion gap) was 61, surpassing urinary NH4+ excretion altogether favors distal RTA.
Hypocalcemia, hypophosphatemia, and metabolic acidosis, either alone or in combination, impede proper mineralization of the growth plate, leading to the development of rickets [4]. A child should be suspected renal tubular acidosis (RTA) when there are symptoms of growth retardation, failure to thrive, polyuria, polydipsia, and refractory rickets [5]. Although we did not perform the NH4 loading test, the presence of nephrocalcinosis and persistent urinary pH > 5.5 despite metabolic acidosis can help differentiate distal RTA from proximal RTA. Although genetic testing was not possible, there is no history of similar diseases in the family, suggesting a sporadic form.
The aim of distal RTA treatment in children is not only correcting biochemical abnormalities, but also improving growth and preventing kidney stones and skeletal abnormalities. The basis of the treatment is alkali replacement. Potassium citrate or sodium citrate is preferable to bicarbonate because citrate salt can correct hypocitraturia and prevent nephrolithiasis. If the distal RTA is accompanied by rickets, calcium, and vitamin D replacement are required [10].
Our patient has shown positive biochemical and physical responses, shown by improved growth and development, following the administration of bicarbonates and potassium citrate supplementation.
Conclusion
Rickets is a commonly encountered clinical problems especially affecting the pediatric patients. The most common cause of rickets is nutritional deficiency in childhood although there are some rare cases rickets secondary to renal tubular acidosis, hypophosphatemic rickets or vitamin D resistant rickets. In patients who do not respond to usual doses of calcium and vitamin D, or in cases where vitamin D deficiency has been ruled out, further tests should be conducted to exclude these conditions. The presence of metabolic acidosis with normal anion gap points towards RTA Further differentiation between types 1 and 2 can be made based on urinary pH and urinary anion gap. Potassium citrate can be used as a treatment to normalize acidosis and hypokalemia in dRTA, as well as acquired hypophosphatemia without the need for concomitant phosphate therapy. Early diagnosis and management are crucial for the resolution of rickets, emphasizing the importance of a thorough evaluation.
References
- Buckalew VM Jr. (1989). Nephrolithiasis in renal tubular acidosis. J Urol, 141(3 Pt 2):731-737.
Publisher | Google Scholor - Sahay M, Sahay R. (2013). Renal rickets-practical approach. Indian J Endocrinol Metab, 17(Suppl 1):S35-44.
Publisher | Google Scholor - Lemann J Jr, Litzow JR, Lennon EJ. (1966). The effects of chronic acid loads in normal man: further evidence for the participation of bone mineral in the defense against chronic metabolic acidosis. J Clin Invest, 45(10):1608-1614.
Publisher | Google Scholor - Agrawal SS, Mishra CK, Agrawal C, et al. (2020). Rickets with hypophosphatemia, hypokalemia and normal anion gap metabolic acidosis: not always an easy diagnosis. BMJ Case Rep, 13:e233350.
Publisher | Google Scholor - Bagga A, Sinha A. (2007). Evaluation of renal tubular acidosis. Indian J Pediatr, 74(7):679-686.
Publisher | Google Scholor - Manisha Sahay, Rakesh Sahay. (2013). Renal rickets-practical approach: Indian Journal of Endocrinology and Metabolism, 17(1).
Publisher | Google Scholor - Palmer BF, Kelepouris E, Clegg DJ. (2021). Renal Tubular Acidosis and Management Strategies: A Narrative Review. Adv Ther, 38(2):949-968.
Publisher | Google Scholor - Bagga A, Bajpai A, Menon S. (2005). Approach to renal tubular disorders. Indian J Pediatr, 72(9):771-776.
Publisher | Google Scholor - Reddy S, Kamath N. (2020). Clinical approach to renal tubular acidosis in children. Karnataka Paediatr J, 35(2):88-94.
Publisher | Google Scholor - Lee JH, et al. (2013). Refractory rickets caused by mild distal renal tubular acidosis. Annals of Pediatric Endocrinology & Metabolism, 18(3):152-155.
Publisher | Google Scholor













