

Research Article
Revolutionizing Patient Care: Unveiling the Potential of Enhanced Recovery After Surgery (ERAS) Pathway in Enhancing Recovery and Quality of Life for Lower Limb Necrotizing Fasciitis Patients
- Mounika Basani 1
- Nemi Chandra J 1*
- Heena Parveen 1
- Sri Saran Manivasagam 2
- Vivek Belsariya 1
- Vaibhav Khuraria 1
- Hinduja Raju 1
- Madhuri Singamsetty 1
- Sandeep Rao Kordcal 3
1 General Surgery, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
2 General Surgery, Maulana Azad Medical College, New Delhi, India.
3 General Surgery, All India Institute of Medical Sciences, New Delhi, India.
*Corresponding Author: Nemi Chandra J, General Surgery, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
Citation: Basani M, Nemi C J, Parveen H, Sri S Manivasagam, Belsariya V, et al. (2024). Revolutionizing Patient Care: Unveiling the Potential of Enhanced Recovery After Surgery (ERAS) Pathway in Enhancing Recovery and Quality of Life for Lower Limb Necrotizing Fasciitis Patients. Journal of Clinical Surgery and Surgical Research, BioRes Scientia publishers. Publishers. 3(1):1-11. DOI: 10.59657/2992-9989.brs.24.019
Copyright: © 2024 Nemi Chandra J, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 30, 2023 | Accepted: December 15, 2023 | Published: January 05, 2024
Abstract
Background: A subtype of severe skin and soft tissue infections (SSTIs) known as necrotizing fasciitis (NF) results in the necrosis of subcutaneous tissues and muscle fascia. Necrotizing fasciitis has a 50% death rate in the absence of adequate resuscitation and prompt surgical intervention. Enhanced Recovery After Surgery (ERAS) programs alter the physiological reactions of the body to major surgeries and promote early recovery. The objective of this study is to study the role of the Enhanced Recovery After Surgery (ERAS) pathway in the management of patients with lower limb necrotizing fasciitis in terms of time taken for healthy granulation after radical debridement and negative pressure wound therapy (NPWT) and length of hospital stay.
Materials and Methods: A prospective observational cohort study was conducted to include 150 patients with lower limb necrotizing fasciitis, aged more than 12 years, who presented to the Surgery outpatient department of VMMC and Safdarjung Hospital, New Delhi, between January 2022 and January 2023. After a detailed history and clinical, biochemical, and radiological examination, patients were adequately resuscitated and managed according to the ERAS protocol. They underwent radical debridement followed by NPWT dressings in multiple sittings until the formation of healthy granulation tissue. They were regularly assessed by the Bates Jensen Wound Assessment Tool (BWAT) score. Once healthy granulation tissue is formed, wound coverage is done with skin grafting. The primary endpoint of the study was the achievement of early granulation and early wound coverage. Categorical variables were presented in numbers and percentages (%), and continuous variables were presented as mean ± SD and median. The normality of the data was tested by the Kolmogorov-Smirnov test. Quantitative variables were compared using a paired t-test or Wilcoxon signed rank test (when the data sets were not normally distributed) across follow-up within mildly severe and moderately severe groups. A p-value of <0.05 was considered statistically significant.
Results: The mean age was 46.63 years. 73.3% of the participants were male, while 26.7% were female. The mean BMI was 22.61 kg/m². The majority of patients (66.70%) had no co-morbidities. 20% of patients were diabetic, and 6.7% were hypertensive. 63.3% (n = 95) of the participants belonged to the ‘Mild severity’ group (BWAT Score: 20 to 30), while 36.7% (n = 55) of the participants belonged to the ‘Moderate severity’ group (BWAT Score: 31 to 40). The mean time for ambulation was 1.17 days. The most common organism in the study population was Staphylococcus aureus (40%), followed by polymicrobials at 26.7%. The mean time for granulation in the mild severity group was 15.68 days, and in the moderate severity group, it was 23.56 days. Ten patients (6.6%) who had wound complications had to undergo amputation as a lifesaving procedure for control of ongoing sepsis. Rest 140 patients got adequate wound coverage. The mean length of stay for the mild severity group was 17.21 days, and the moderate severity group was 24.91 days.
Conclusion: ERAS pathways can be safely implemented in patients with lower limb necrotizing fasciitis to improve postoperative outcomes such as reduced length of hospital stay, early wound granulation, reduced wound-related complications, and the need for amputation.
Keywords: enhanced recovery after surgery (eras); necrotizing fasciitis (nf); radical debridement; laboratory risk indicator for necrotizing fasciitis (lrinec) score; bates jensen wound assessment tool (bwat) score
Introduction
A subtype of severe skin and soft tissue infections (SSTIs) known as necrotizing fasciitis (NF) results in the necrosis of subcutaneous tissues and muscle fascia. There is minimal blood flow in the fascial plane, which is where this condition usually spreads. Therefore, the underlying tissues are not damaged at first, which might delay diagnosis and surgical intervention. Rapid progression of the infectious process can lead to infection of the skin, soft tissue, and muscle directly below, as well as the fascia and peri-fascial planes. Necrotizing fasciitis is possible after surgery, any invasive technique, or even an elementary one like phlebotomy [1]. Patients may exhibit fever, erythema, vesicles, bullae, oedema, and crepitus in addition to cellulitis. Their complaints of pain are frequently exaggerated; however, as the infection worsens, their pain usually decreases. Laboratory results might demonstrate coagulopathy, acidosis, anaemia, electrolyte imbalance, increased white blood cell count, and anaemia [2]. Necrotizing fasciitis has a 50
Material and Methods
A prospective observational cohort study was conducted to include 150 patients with lower limb necrotizing fasciitis, aged more than 12 years, who presented to the Surgery outpatient department of VMMC and Safdarjung Hospital, New Delhi, between January 2022 and January 2023
Study Design: Prospective open label observational study
Study Location: This was a tertiary care teaching hospital-based study done in Department of General Surgery, at VMMC and Safdarjung Hospital, New Delhi.
Study Duration: January 2022 and January 2023
Sample size: 150 patients.
Sample size calculation: The study of Wen-Shyan Huang13, observed that the mean length of hospital stay was 32.1. Taking this value as reference and assuming standard deviation of 8, the minimum required sample size with estimate to be within 10% of mean value and 5% level of significance is 24 patients. To reduce margin of error, total sample size taken is 30.
Subjects & selection method: The study population was drawn from 150 patients with lower limb necrotizing fasciitis, aged more than 12 years, who presented to the Surgery outpatient department of VMMC and Safdarjung Hospital, New Delhi, between January 2022 and January 2023
Inclusion criteria
All adult patients diagnosed with lower limb necrotizing fasciitis having the following: (FIGURE 1)
A. Modified LRINEC score of 6-10.
B. Wound score (BWAT SCORE-Bates Jensen Wound Assessment Tool) of 21-40.
C. Age more than 12
Exclusion criteria
A. SOFA (Sequential Organ Failure Assessment) score more than 10,
B. Soft tissue involvement over 2 or more joints,
C. Pregnancy,
D. BMI (Body Mass Index) greater than 35,
E. Diabetic Charcot’s arthropathy
F. Paraplegic patients.
Procedure methodology
Every patient was subjected to a detailed clinical history and thorough clinical examination. Essential investigations including Complete Blood Count, Renal and Liver function tests, Serum electrolytes, Serum protein and albumin levels, Random Blood sugar levels, Coagulation profile, x-ray of the part involved, HbA1c (in case of chronic diabetic mellitus), PCT and CRP test were carried out After informed and written consent, the patient was managed according to the ERAS protocol. It involves a set of preoperative, intraoperative, and postoperative interventions (Table 1). The primary endpoint of the study was the achievement of early granulation and early wound coverage. In the postoperative period, patients were followed while in the hospital or after discharge for 30 days for wound and non-wound-related complications. Wound-related complications such as persistent ongoing peri-wound tissue necrosis, bleeding, and surgical site infections. Non-wound-related complications such as pulmonary, cardiac, and renal.
Statistical analysis
The data was entered in a Microsoft Excel spreadsheet, and analysis was done using Statistical Package for Social Sciences (SPSS) version 28.0. Categorical variables were presented in numbers and percentages (%), and continuous variables were presented as mean ± SD and median. The normality of the data was tested by the Kolmogorov-Smirnov test. If normality is rejected, then a nonparametric test is used. Quantitative variables were compared using a paired t-test or Wilcoxon signed rank test (when the data sets were not normally distributed) across follow-up within mildly severe and moderately severe groups. A p-value of <0>

Figure 1: Necrotizing fasciitis of a middle-aged male diabetic patient medial view.
Table 1: ERAS Protocol components
| Pre-Operative Interventions |
| 1. Pre admission information and counselling. |
| 2. Early resuscitation and optimization for surgery |
| 3. Preoperative fasting: 2 hours for liquids, 6 hours for solids. |
| 4. High carbohydrate drink 2 hours before surgery |
| 5. Antibiotic Prophylaxis- Empirical broad-spectrum antibiotics started and later modified based on each culture and sensitivity report. |
| Intra-Operative Interventions |
| 1. Radical debridement under appropriate anesthesia. |
| 2. Strict Intraoperative fluid management. |
| 3. Routine use of warmers. |
| Post-Operative Interventions |
1. Deep Vein Thrombosis (DVT) prophylaxis - Low Molecular Weight Heparin 40mg OD |
| 2. Per urethral catheter removal at the earliest. |
| 3. Multimodal analgesia for Pain management. |
| 4. Post operative nausea and vomiting prophylaxis |
5. Nutritional support with high calorie and protein diet. (25 kcal and 1.5g protein per kg body weight) |
| 6. Chest care with incentive spirometry and chest physiotherapy |
| 7. Early mobilization on POD1 and physiotherapy of involved limb and joint. |
8. Negative pressure wound therapy was applied on POD1. Wound was reassessed every 4th day. |
| 9. At each change, wound score calculation, debridement of the wound and obtaining tissue for culture sensitivity. |
| 10. Antibiotics changed according to culture sensitivity report |
| 11. Split skin graft or flap reconstruction, once wound granulates. |
Result
The prospective observational study was conducted to include a total of 150 patients diagnosed with necrotizing fasciitis of the lower extremity based on clinical and surgical findings (Figure 1), a modified LIRNEC score between 6 and 10, and a BWAT score between 21 and 40. Patients were predominantly in their 5th and 6th decades of life (23.3 percentage each), followed by the 4th decade (20%). The mean age was 46.63 years, and the median age was 48 years. 73.3% of the participants were male, while 26.7% were female. 63.3% of the participants had BMI in the range 18.5 to 22.9 kg/m². The mean BMI was 22.61 kg/m² and the median BMI was 22.40 kg/m². The BMI (kg/m²) ranged from 18.6 to 26.5. The majority of patients (66.70 %) had no co-morbidities. 20 % of patients were diabetic, 6.7% were hypertensive and 3.3% were asthmatic. 63.3% of the participants had a BWAT Score of 20 to 30. (Mild severity). (Table 2).
Table 2: Distribution of Age, Gender, BMI and Comorbidities
| Age | Frequency | Percentage | 95% CI |
| 21-30 Years | 25 | 16.7% | 6.3% - 35.5% |
| 31-40 Years | 30 | 20.0% | 8.4% - 39.1% |
| 41-50 Years | 35 | 23.3% | 10.6% - 42.7% |
| 51-60 Years | 35 | 23.3% | 10.6% - 42.7% |
| 61-70 Years | 20 | 13.3% | 4.4% - 31.6% |
| 71-80 Years | 5 | 3.3% | 0.2% - 19.1% |
| Age (years) | |||
| Mean (SD) | 46.63 (15.12) | ||
| Median (IQR) | 48.5 (36.5-54) | ||
| Range | 21 - 80 | ||
| Gender | Frequency | Percentage | 95% CI |
| Male | 110 | 73.3% | 53.8% - 87.0% |
| Female | 40 | 26.7% | 13.0% - 46.2% |
| BMI | Frequency | Percentage | 95% CI |
| 18.5-22.9 Kg/m2 | 95 | 63.3% | 43.9% - 79.5% |
| 23.0-24.9 Kg/m2 | 30 | 20.0% | 8.4% - 39.1% |
| 25.0-29.9 Kg/m2 | 25 | 16.7% | 6.3% - 35.5% |
| BMI (Kg/m²) | |||
| Mean (SD) | 22.61 (2.05) | ||
| Median (IQR) | 22.4 (21.33-23.92) | ||
| Range | 18.6 - 26.5 | ||
| Co-morbidities | Frequency | Percentage | 95% CI |
| None | 100 | 66.7% | 47.1% - 82.1% |
| Asthma | 5 | 3.3% | 0.2% - 19.1% |
| Diabetic | 30 | 20.0% | 8.4% - 39.1% |
| Hypertension | 10 | 6.7% | 1.2% - 23.5% |
| DM+HTN | 5 | 3.3% | 0.2% - 19.1% |
All patients were classified into two groups based on BWAT score (Bates Jensen Wound Assessment Tool). 63.3% (n=95) of the participants belonged to the ‘Mild severity’ group (BWAT Score: 20 to 30), while 36.7% (n=55) of the participants belonged to the ‘Moderate severity’ group (BWAT Score: 31 to 40). (Table 3). Before the debridement, the mean BWAT score in the ‘Mild severity’ group was 25.68 and the median was 26. The mean BWAT score in the ‘Moderate severity’ group was 35.27 and the median was 36. The mean SOFA score of the mild severity group was 1.95 and in the moderate severity group is 3.36. The mean procalcitonin (PCT) level in the mild severity group was 1.00ng/mL, and in the moderate severity group was 1.32ng/mL. The mean C-reactive protein (CRP) value in the mild severity group was 1.95mg/L, and in the moderate severity group was 3.36mg/L. (Table 3).
Table 3: Pre-operative Distribution of BWAT score, SOFA score, PCT and CRP
| BWAT Score | Frequency | Percentage | 95% CI | |
| <20> | 95 | 63.3% | 43.9% - 79.5% | |
| >31 to 40(Moderate severity) | 55 | 36.7% | 20.5% - 56.1% | |
BWAT Score (Pre-Operative) | BWAT Score | Wilcoxon-Mann-Whitney U Test | ||
| <20> | >31 to 40 | W | p value | |
| Mean (SD) | 25.68 (2.29) | 35.27 (2.28) | 0.000 | <0> |
| Median (IQR) | 26 (24-28) | 36 (33.5-37) | ||
| Range | 22 - 30 | 32 - 38 | ||
| SOFA Score | BWAT Score | |||
| <20> | >31 to 40 | |||
| Mean (SD) | 1.95 (0.71) | 3.36 (1.36) | ||
| Median (IQR) | 2 (1.5-2) | 3 (2-4) | ||
| Range | 1 - 3 | 2 – 6 | ||
| PCT** | BWAT Score | |||
| <20> | >31 to 40 | |||
| Mean (SD) | 1.00 (0.18) | 1.32 (0.29) | ||
| Median (IQR) | 0.96 (0.89-1.07) | 1.25 (1.08-1.49) | ||
| Range | 0.74 - 1.37 | 0.98 - 1.86 | ||
| **Procalcitonin (PCT) in ng/mL | ||||
| CRP*** | BWAT Score | |||
| <20> | >31 to 40 | |||
| Mean (SD) | 2.30 (0.29) | 3.01 (0.40) | ||
| Median (IQR) | 2.31 (2.14-2.39) | 2.97 (2.77-3.26) | ||
| Range | 1.85 - 2.86 | 2.39 - 3.68 | ||
| ***C Reactive Protein (CRP) in mg/L | ||||
All 150 patients with lower limb necrotizing fasciitis underwent surgical debridement within 24 hours of admission (Figure 2). They were treated on the lines of ERAS protocol. All patients were resuscitated before being shifted to the operation theater. Patients were preoperatively counselled about the nature of the disease and the course of their hospital stay. The mean operative time in the mild-severity group was 82.74 minutes. The mean operative time in the moderate-severity group was 90.18 minutes. A total of 40 (26.7%) out of 150 patients required blood transfusions, of which 35 (63.6%) were from the moderate severity group and 5 (5.3%) from the mild severity group (Table 4). Five (3.3%) out of 150 patients required oxygen supplementation, and eventually oxygen support was weaned off by post-operative day 4. The rest of the 145 patients were not on any oxygen supplementation or ventilation. 135 (90%) of the study population were able to do in-room ambulation on POD1. 10 patients were able to do this by post-operative day (POD) 2 due to high pain scores and raw wounds near the joints. 5 patients who were on oxygen support were able to do so by POD 4. The mean time for ambulation was 1.17 days. The most common organism in the study population was Staphylococcus aureus (40%), followed by polymicrobial 26.7%. 52.6% of patients of mild severity are positive for Staphylococcus aureus. 36.4% of patients of moderate severity were positive for polymicrobial organisms. (Table 4).

Figure 2: Post Debridement wound
Table 4: Peri-operative Variables
Operative Time (minutes) | BWAT Score | ||
| <20> | >31 to 40 | ||
| Mean (SD) | 82.74 (3.60) | 90.18 (7.21) | |
| Median (IQR) | 82 (80-85) | 90 (85.5-96) | |
| Range | 78 - 89 | 78 - 99 | |
| Blood Transfusion | BWAT Score | ||
| <20> | >31 to 40 | Total | |
| Yes | 5 (5.3%) | 35 (63.6%) | 40 (26.7%) |
| No | 90 (94.7%) | 20 (36.4%) | 110 (73.3%) |
| Total | 95 (100.0%) | 55 (100.0%) | 150 (100.0%) |
| Culture Sensitivity | Frequency | Percentage | 95% CI |
| E.Coli | 10 | 6.7% | 1.2% - 23.5% |
| Enterobacter | 5 | 3.3% | 0.2% - 19.1% |
| Klebsiella | 5 | 3.3% | 0.2% - 19.1% |
| MRSA | 5 | 3.3% | 0.2% - 19.1% |
| Polymicrobial | 40 | 26.7% | 13.0% - 46.2% |
| Proteus | 5 | 3.3% | 0.2% - 19.1% |
| Pseudomonas | 5 | 3.3% | 0.2% - 19.1% |
| Staph Aureus | 60 | 40.0% | 23.2% - 59.2% |
| Streptococcus | 15 | 10.0% | 2.6% - 27.7% |
| Day of normalisation of TLC | BWAT Score | ||
| <20> | >31 to 40 | ||
| Mean (SD) | 3.42 (0.69) | 6.45 (1.37) | |
| Median (IQR) | 3 (3-4) | 6 (6-7) | |
| Range | 2 - 5 | 4 – 9 | |
The mean number of days for normalisation of TLC was 3.42 days in the mild severity group and 6.45 days in the moderate severity group. Serial application of negative pressure wound therapy (NPWT) or vacuum (VAC) dressing was done (Figure 3). In the mild severity group, the mean BWAT score after the first VAC application was 19.89, and the median was 20. In the moderate severity group, the mean was 29.55 and the median was 26 (Figure 4). In the mild severity group, the mean BWAT score after the second VAC application was 16.89, and the median was 17.5. In the moderate severity group, the mean was 24.10 and the median was 24 (Figure 5). In the mild severity group, the mean BWAT score after the third VAC application was 16.15, and the median was 16. In the moderate severity group, the mean was 21.10 and the median was 21 (Table 5). In the course of treatment, 140 patients (93%) had no wound complications. 5 (3.3%) had peri-wound necrosis, and 5 (3.3%) had persistent sepsis. 140 patients (93%) showed granulation tissue without any wound complications. From the day of granulation, patients didn’t require any further bedside minor debridement, and a wound bed was prepared for wound coverage. The mean time for granulation in the mild severity group was 15.68 days, and in the moderate severity group, it was 23.56 days. 140 patients (93%) had granulated wounds prepared for wound coverage. The wound coverage was done either by grafting in 125 patients (83.4%) (Figure 6), delayed primary closure in 5 patients (3.3%), or shoelace technique in 10 patients (6.6%) (Figure 7). Ten patients (6.6%) who had wound complications had to undergo amputation as a lifesaving procedure for control of ongoing sepsis. The mean length of stay for the mild severity group was 17.21 days, and the moderate severity group was 24.91 days. The mean number of minor or major debridements after radical surgical debridement in the mild severity group was 1.53, ranging from 0-3, and in the moderate severity group was 2.64, ranging from 2-4. All patients’ wounds were managed by serial negative pressure wound therapy (NPWT) or vacuum therapy (VAC) starting in the immediate postoperative period. The mean number of VAC dressings required before the wound bed was prepared for coverage in the mild severity group was 3 and in the moderate severity group was 4.55. (Table 5).
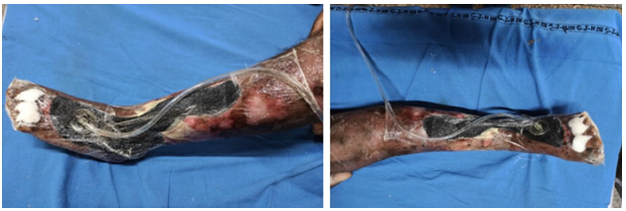
Figure 3: NPWT or VAC dressing

Figure 4: Wound after removal of First VAC dressing

Figure 5: Wound after removal of second VAC dressing

Figure 6: Split skin graft coverage of wound

Figure 7: Shoe-lace technique
Table 5: Statistical analysis of Results
| BWAT Score (VAC 1) | BWAT Score | ||
| <20> | >31 to 40 | ||
| Mean (SD) | 19.89 (2.88) | 29.55 (3.62) | |
| Median (IQR) | 20 (18-21.5) | 28 (26-32) | |
| Range | 15 - 26 | 26 - 36 | |
| BWAT Score (VAC 2) | BWAT Score | ||
| <20> | >31 to 40 | ||
| Mean (SD) | 16.89 (1.78) | 24.10 (2.64) | |
| Median (IQR) | 17.5 (15-18) | 24 (22.25-26) | |
| Range | 15 - 20 | 20 - 28 | |
| BWAT Score (VAC 3) | BWAT Score | ||
| <20> | >31 to 40 | ||
| Mean (SD) | 16.15 (1.21) | 21.10 (2.60) | |
| Median (IQR) | 16 (15-17) | 21 (19.25-22) | |
| Range | 14 - 18 | 18 - 26 | |
| Wound Complication | Frequency | Percentage | |
| None | 135 | 90.0% | |
| Peri-wound necrosis | 10 | 6.7% | |
| Sepsis | 5 | 3.3% | |
| Days for Granulation | BWAT Score | ||
| <20> | >31 to 40 | ||
| Mean (SD) | 15.68 (2.73) | 23.56 (3.32) | |
| Median (IQR) | 16 (14.5-17) | 22 (22-26) | |
| Range | 9 - 20 | 19 - 28 | |
| Management | BWAT Score | ||
| <20> | >31 to 40 | Total | |
| Amputation | 0 (0.0%) | 10 (18.2%) | 10 (6.7%) |
| Delayed Primary Closure | 5 (5.3%) | 0 (0.0%) | 5 (3.3%) |
| Grafting | 80 (84.2%) | 45 (81.8%) | 125 (83.3%) |
| Shoelace Technique | 10 (10.5%) | 0 (0.0%) | 10 (6.7%) |
| Total | 95 (100.0%) | 55 (100.0%) | 150 (100.0%) |
| Days of Hospital Stay | BWAT Score | ||
| <20> | >31 to 40 | ||
| Mean (SD) | 17.21 (2.44) | 24.91 (7.09) | |
| Median (IQR) | 18 (15.5-18.5) | 23 (22-28) | |
| Range | 13 – 22 | 11 - 38 | |
| No. of Redebridment | BWAT Score | ||
| <20> | >31 to 40 | ||
| Mean (SD) | 1.53 (0.77) | 2.64 (0.67) | |
| Median (IQR) | 1 (1-2) | 3 (2-3) | |
| Range | 0 - 3 | 2 - 4 | |
| No of VAC Dressing | BWAT Score | ||
| <20> | >31 to 40 | ||
| Mean (SD) | 3.00 (1.05) | 4.55 (1.21) | |
| Median (IQR) | 3 (2-4) | 4 (4-5.5) | |
| Range | 1 - 5 | 2 - 6 | |
Discussion
Every surgeon encounters necrotizing fasciitis as a surgical emergency while completing their residency. Sepsis is frequent among patients, and more than half of them are at risk of barely recovering if wound care and rehabilitation are not undertaken together. Even with prompt sepsis treatment, patients who are out of sepsis have a longer hospital stay [2]. The Enhanced Recovery After Surgery (ERAS) protocol has been shown to improve postoperative recovery for patients undergoing emergency surgeries. So, we have implemented these ERAS pathways and observed outcomes in our patients. Age groups 41-50 and 51-60 years old accounted for the majority of the study population in the study group (23.3%), followed by age groups 31-40 years old (20.0%). The age group over 60 accounted for about 16.6% of the overall study population. Similar findings were found in a study by Misiakos et al., which showed that while the disease affects all age groups, middle-aged and elderly people have a higher risk of infection [7]. While necrotizing fasciitis can affect people of any age, 40 (26.7%) of the study group's participants were female, and 110 (73.3%) were male. This finding aligns with a study conducted by Sadasivan et al., which revealed a noticeable male predominance in 54 scenarios [8]. Thirty-three percent of the patients in the study had comorbidities. The most frequent comorbidity (20.0%) was diabetes mellitus, which was followed by hypertension (6.7%). According to a study by Shukla et al., diabetes mellitus is one of the main risk factors that affects 70 out of 107 patients [9]. In a different study by Elliot et al., 110 of the 198 individuals with necrotizing fasciitis also had diabetes mellitus [10]. Patients in the 21-40 BWAT score range were chosen. BWAT scores were assessed following each NPWT/VAC dressing as well as on the day of the patient's admission. The research population showed improvement in their wounds following each VAC dressing, and their wound score was trending downward. Two patients had wound complications.
73.3% of the 150 patients had monomicrobial infections, while 26.7% of the patients had polymicrobial infections. The majority of individuals with monomicrobial infections tested positive for Staphylococcus aureus (43.3%) and Streptococcus (10%). The findings align with a 2018 study conducted by Nautiyal HK et al., which found that Staphylococcus aureus was the most isolated organism within the necrotizing fasciitis study group, followed by polymicrobials [11]. The antibiotic response was satisfactory in almost all patients except for five patients who continued to be in sepsis even after radical surgical debridement and antibiotic modification and required amputation. Throughout the patient's hospital stay, measurements of procalcitonin (PCT) and C-reactive protein (CRP) were taken both before surgery and following each VAC dressing. Almost all patients showed a downward trend in both PCT and CRP values throughout the study, except ten patients who had to undergo amputation due to surrounding tissue necrosis and sepsis, despite having appropriate debridement on many occasions. Hence, these can be used as efficient prognostic markers. After preliminary resuscitation, all patients had surgical debridement within 24 hours of admission. Under a subarachnoid block, radical surgical debridement was carried out. According to a metaanalysis by Nawijn et al., early surgical debridement reduces the death rate for necrotizing fasciitis by about 50% [3]. In our study, the mean operating time for the group with mild severity was 82.74 ± 3.60 min, and for the group with moderate severity, it was 90.18 ± 7.21 min. In our study, blood transfusions were necessary for 26.7% of the patients. Patients who underwent blood transfusions and anaemia at the time of admission experienced delayed wound healing and extended hospital stays. These findings corroborated an analysis by Lieberman et al. in which anaemia was found to be a risk factor for a poor prognosis in patients with necrotizing fasciitis [12].
In the mild severity group, the average hospital stay was 17.21 ± 2.44 days, while in the moderate severity group, it was 24.91 ± 7.09 days. Ten patients in the moderate severity group required more bedside debridement and had comorbidities, high PCT and CRP levels, and older ages. These patients also required a longer stay. The mean length of hospital stay for patients with necrotizing fasciitis in our study was 19.7 days, which was comparable to the results of a study by Misiakos et al. However, the patients in that study weren't discharged with their wounds covered. A 13-day stay in the hospital was the minimum7. Research by Huang et al. revealed a 32.1-day average hospital stay [13]. In our study group, the average time to ambulate was 1.17 ± 0.59 days. By the first day, most of them could walk around in their rooms. Due to pain, ten patients were able to accomplish it on day two following appropriate analgesic coverage and counseling. Five oxygen-dependent individuals were able to perform by day four. Patients with lower limb necrotizing fasciitis typically prefer not to move the affected leg at all. To encourage ambulation within the research population, adequate analgesic coverage and counseling were provided. Dietary changes were made in accordance with the comorbidities and condition of the patient. All patients received nutrition supplements in the form of soluble powder in addition to their usual diet. 135 individuals did not lose any weight while they were in the hospital. Despite receiving enteral and parenteral feeding, five patients with chronic sepsis experienced weight loss. Malnutrition was found to be a modifiable factor that impedes wound healing in a patient with necrotizing fasciitis in a study by Hakkarainen TW et al [14]. In our study, 140 patients were discharged with either a wound-covered or wound bed prepared for grafting without any wound- or nonwound- related complications. Five patients with comorbidities on oral steroids had persistent periwound necrosis and had to undergo amputation as a lifesaving procedure. Another five patients with sepsis didn’t respond to antibiotic modification or debridement and had to undergo amputation. In a study by Nautiyal et al., 16.7% of the study population's wounds were managed by amputation [11].
We tried to bring about as many changes as possible in patients with lower limb necrotizing fasciitis by implementing the ERAS pathway, beginning with preoperative resuscitation and counselling to postoperative pain management along with nutritional supplementation, rehabilitation, and wound care, with an emphasis on meticulous and radical operative procedures. The limitations of our study were: (A). The sample size of the study was smaller. (B). Our study was not a randomised control trial that could compare the outcomes with the control. (C). Wound-related complications like the development of contracture, graft acceptance rate, phantom limb pain, and neuropathic pain could not be studied due to a shorter study period. Hence, a larger randomised study with a longer follow-up period is required to validate the results.
Conclusion
Necrotizing fasciitis is a common surgical emergency, often associated with comorbidities. With 100% control of comorbidities, non-wound-related complications can be avoided. Implementation of the ERAS protocol in the postoperative period can lead to a reduction in wound-related complications and the need for amputation. Radical debridement and negative pressure wound therapy can reduce the time for granulation tissue formation and the length of hospital stay. ERAS pathways can be safely implemented in patients with lower limb necrotizing fasciitis to improve postoperative outcomes such as reduced length of hospital stay, early wound granulation, reduced wound-related complications, and the need for amputation.
References
- Lange JH, Cegolon L. (2018). Comment on: Early clinical manifestations of vibrio necrotising fasciitis. Singapore Med J, 59:449.
Publisher | Google Scholor - Wong CH, Chang HC, Pasupathy S, et al. (2003). Necrotizing fasciitis: clinical presentation, microbiology, and determinants of mortality. J Bone Joint Surg Am, 85:1454-1460.
Publisher | Google Scholor - Nawijn F, Smeeing DPJ, Houwert RM, et al. (2020). Time is of the essence when treating necrotizing soft tissue infections: a systematic review and meta-analysis. World J Emerg Surg, 15:4.
Publisher | Google Scholor - Wong CH, Khin LW, Heng KS, et al. (2004). The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med, 32:1535-1541.
Publisher | Google Scholor - Bates-Jensen BM, McCreath HE, Harputlu D, et al. (2019). Reliability of the Bates-Jensen wound assessment tool for pressure injury assessment: The pressure ulcer detection study. Wound Repair Regen, 27:386-395.
Publisher | Google Scholor - Chestovich PJ, Lin AY, Yoo J. (2013). Fast-track pathways in colorectal surgery. Surg Clin North Am, 93:21-32.
Publisher | Google Scholor - Misiakos EP, Bagias G, Papadopoulos I, et al. (2017). Early Diagnosis and Surgical Treatment for Necrotizing Fasciitis: A Multicenter Study. Front Surg, 4:5.
Publisher | Google Scholor - Sadasivan J, Maroju NK, Balasubramaniam A. (2013). Necrotizing fasciitis. Indian J Plast Surg, 46:472-478.
Publisher | Google Scholor - Shukla A, Sharma A. (2017). Clinical study of necrotizing fasciitis and its management. Int Surg, 19647.
Publisher | Google Scholor - Elliott DC, Kufera JA, Myers RA. (1996). Necrotizing soft tissue infections. Risk factors for mortality and strategies for management. Ann Surg, 224:672-683.
Publisher | Google Scholor - Nautiyal, Hemant, Agarwal, et al. Clinicopathological profile and management outcome of skin and soft tissue infections at tertiary care centre of sub-Himalayan region. International Surgery Journal. 5:946-1010.
Publisher | Google Scholor - Lieberman JA, Stansbury LG, Kufera JA, et al. (2018). Red Blood Cell Transfusions and Anemia on Admission Are Associated with Poor Outcomes in Necrotizing Soft Tissue Infections. J Appl Lab Med, 3:250-260.
Publisher | Google Scholor - Huang WS, Hsieh SC, Hsieh CS, et al. (2006). Use of vacuum-assisted wound closure to manage limb wounds in patients suffering from acute necrotizing fasciitis. Asian J Surg, 29:135-139.
Publisher | Google Scholor - Hakkarainen TW, Kopari NM, Pham TN, et al. (2014). Necrotizing soft tissue infections: review and current concepts in treatment, systems of care, and outcomes. Curr Probl Surg, 51:344-362.
Publisher | Google Scholor













