

Case Report
Retinal Vein Occlusion by Intracameral Lidocaine Drop Containing Graphene Can Be Revasculized by Nacl + Kcl Injection After Cataract Surgery, And Normalized Coagulation System Disorders
Department of Emergency Medicine, New life Hospital Bokhyun-dong, Bukgu, Daegu, South Korea.
*Corresponding Author: Chur Chin,Department of Emergency Medicine, New life Hospital Bokhyun-dong, Bukgu, Daegu, South Korea.
Citation: : Chin C. (2024). Retinal Vein Occlusion by Intracameral Lidocaine Drop Containing Graphene Can Be Revasculized by Nacl + Kcl Injection After Cataract Surgery, And Normalized Coagulation System Disorders, International Journal of Medical Case Reports and Reviews, BioRes Scientia Publishers. 3(1):1-2. DOI: 10.59657/2837-8172.brs.24.038
Copyright: © 2024 Chur Chin, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 15, 2024 | Accepted: February 01, 2024 | Published: February 09, 2024
Abstract
A 55-year-old man who had blurred vision due to cataract of both eyes, were performed standard phacoemulsification with intraocular lens implantation 1 years ago. During the operation, after 1 or 2 drops of topical lidocaine hydrochloride 1% (Xylocaine®-MPF 1%) were applied to the ocular surface, a 1.0 mm side-port incision was created through which Xylocaine-MPF 1% injected into the anterior chamber.
Keywords: renal;surgery;disordres
Description
On the follow-up examination opthalmology clinic, the cataract surgery, a dilated and tortuous retinal vessels involving the right eye. Upon examination was 20/20 in both normal colour vision and no relative afferent pupillary defect. Dilated fundus examination showed a superior nasal BRVO in the right eye. Laboratory tests including complete blood count, erythrocyte sedimentation rate, C-reactive protein, hemoglobin A1c, international normalized ratio/partial thromboplastin time, homocysteine, anti-cardiolipin, lupus anticoagulant, factor V Leiden were all normal. The patient had no medical comorbidities, and was not taking any medication. Hematology consultation did not uncover any additional risk factors. The intravenous infusion of a solution consisting of 250 mL normal saline with potassium chloride (KCl) over 6 h, vitamin C intake resulted in recovery of the fundus exam findings (1-6). RVO which includes BRVO is the second most common vision-threatening retinal vascular disorder (7). We postulate that an immunological response evoked by the graphene in the lidocaine, venous thrombosis in patient. The pathogenesis may involve microvascular alternations at the level of the retina.
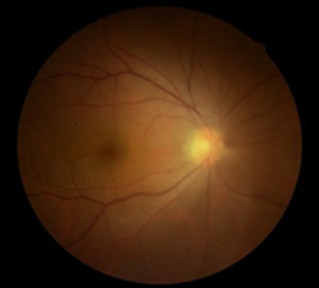
Normal left eye
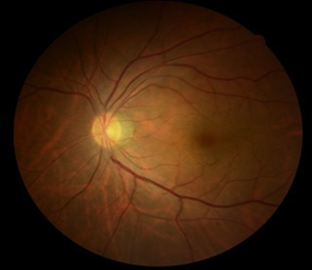
Lidocaineeyedropofsurgery side
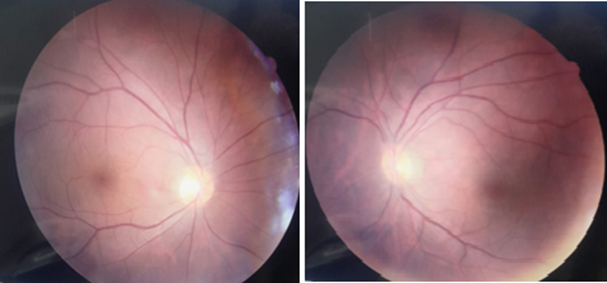
Revasculization after NaCl + KCl injection
Figure 1: Colour eye temporal branch retinal vein occlusion demonstrating venous dilation and tortuosity. The findings were normalized after NaCl + KCl injection.
A 59-year-old man with right basal ganglia infarct to our hospital with a history of left extremity weakness, vital signs: blood pressure 140 (systolic) / 83 (diastolic), heart rate 74, platelet count of 374000/cmm, Asparagine aminotransferase (AST) 28 IU/l, Alanine aminotransferase (ALT) 32 IU/l, Blood Urea Nitrogen (BUN) 12.7 mg/dl, Creatinine (Cr) 1.05 and erythrocyte sedimentation rate (ESR) 48 mm in the first hour using Westergren method, C-reactive protein (CRP) 0.29 mg/dl, thrombin time (PT) 19.4 second, prothrombin time (PTT) 25.5 second, international normalized ratio (INR) 1.94. The intravenous infusion of a solution consisting of 250 mL normal saline with potassium chloride (KCl) over 6 h, vitamin C intake resulted in recovery of PT 13.5 second, PTT 28.9 second, INR 1.29. Circulating anticoagulants are usually autoantibodies that “attack” specific clotting factors, such as an autoantibody against factor V, or inhibit phospholipid bound proteins. Patients may develop lupus anticoagulant hypoprothrombinemia or antiphospholipid syndrome. Occasionally, the latter type of autoantibody causes bleeding by binding to prothrombin–phospholipid complexes. Such antibodies may develop due to autoimmune disease or be graphene-induced (8). Protein C, a vitamin K-dependent protease presented in low levels in human plasma, inhibiting thrombin production and coagulation. The functions of protein C, inflammation and cytoprotection, protein S, a cofactor to activate protein C in the cleavage of Va. C and S, inherited and acquired,autosomal recessive inheritance.
Table 1: Normalization of thrombin time (PT) prolongation of thse similar cases after NaCl + KCl injection.
| Laboratory data | Case 1. initial | Case 1. after NaCl +KCl | Case 2. initial | Case 2. After NaCl +KCl | Case 3. initial | Case 3. after NaCl +KCl |
| PT | 15.4 | 14.9 | 15.5 | 15 | 15.1 | 13.1 |
| INR | 1.49 | 1.4 | 1.5 | 1.4 | 1.46 | 1.24 |
| PTT | 26 | 26.7 | 25.4 | 26.7 | 28.4 | 25.4 |
| BUN | 21.6 | 13.9 | 15.9 | 17.3 | 13.9 | 13.9 |
| Cr | 1.44 | 0.6 | 0.94 | 0.65 | 0.74 | 0.6 |
| AST | 33 | 30 | 38 | 17 | 21 | 29 |
| ALT | 35 | 22 | 11 | 11 | 20 | 24 |
References
- Chin C. (2023). Comparison of 50 Cases of the Anti-Cancer Effects of NaCl with KCl as a Potent Graphene Exfoliator, Prehydrated Patients to NaCl-Only Prehydrated Patients on the Terminal Stage Cancer Patients. Case Reports in Clinical Medicine, 12:425-431.
Publisher | Google Scholor - Chin C. (2023). Changes in electrocardiogram after intramuscular injection of graphene using salt- intercalation exfoliation. J ClinExp Cardiol, 14(5):1-15.
Publisher | Google Scholor - Chin C. (2023). The Anti-Inflammatory Effects of NaCl with KCl as a Potent Graphene Exfoliator in a Patient with Guillaine-Barré Syndrome and Facial Nerve Palsy. Case Reports in Clinical Medicine, 12:447-451.
Publisher | Google Scholor - Chin C. (2023). Improvement of renal functions, graphene-induced rapid progression of prediabetes in an elderly woman with arthritis by graphene-exfoliator NaCl with KCl solution, 3 cases. Journal of Clinical image and medical case report, 4.
Publisher | Google Scholor - Chin C. (2023). Improvement of graphene induced pulmonary edema by graphene exfoliator NaCl with KCl solution. Journal of Clinical image and medical case report, 4.
Publisher | Google Scholor - Chin C. (2023). The anti-inflammatory effects of NaCl with KCl as a potent graphene exfoliator in a patient with interstitial pneumonia by epithelial-mesenchymal transition. Journal of Clinical image and medical case report, 4.
Publisher | Google Scholor - Tripodi, A. Mancuso, M.E. Chantarangkul, V. Clerici, M. Bader, R.;Meroni, P.L. Santagostino, E. Mannucci, P.M. (2005). Lupus anticoagulants and their relationship with the inhibitors against coagulation factor VIII: Considerations on the differentiation between the 2 circulating anticoagulants. Clin. Chem, 51:1883-1885.
Publisher | Google Scholor










