

Research Article
Reduction of Pain in PsA (Psoriatic Arthritis) With WBC Treatment: Changing Quality of Life
Medical Anthropology, Fondazione di Noopolis, Rome, Italy.
*Corresponding Author: Raimondo Leone, Medical Anthropology, Fondazione di Noopolis, Rome, Italy.
Citation: Leone R. (2023). Reduction of Pain in PsA (Psoriatic Arthritis) With WBC Treatment: Changing Quality of Life, Journal of Clinical Rheumatology and Arthritis, BRS Publishers. 1(1); DOI: 10.59657/ 2993-6977.brs.23.002
Copyright: © 2023 Raimondo Leone, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 04, 2023 | Accepted: May 17, 2023 | Published: May 26, 2023
Abstract
In this short article we will address the case of the application of WBC in combination with drug therapy in a patient with psoriatic arthritis. Through the analysis of objective improvement (inflammatory indices) and subjective improvement (improvement of the social dimension), the anthropological approach shows how the cure passes first of all from the achievement of the patient's well-being, understood as "being well" with oneself and with others. This emotional, psychological and relational improvement also leads to an improvement in the clinical picture, as the tables show.
Keywords: pain; rheumatologist; medical anthropology; cryotherapy; WBC; psoriatic arthritis
Introduction
Since ancient times, we have had the use of treatments to improve people's well-being and health through temperature changes. The use of cold in medical treatments is attested in ancient Greece, Persia, and the Roman Empire, in the form of ice-water mixtures and cold water applied to treat a wide range of diseases. We speak of hot saunas (Whole Body Hyperthermia), the use of cold water with ice (Cold Water Immersion or CWI) or, as we currently refer to it, PBC (Partial Body Cryotherapy) or WBC (Whole Body Cryotherapy). Today, cold application remedies are being developed in the medicine, health, and sport domains. This brief article primarily focuses on the whole-body cryotherapy (WBC), explaining the application in rheumatological diseases with a specific focus on the improvement of the quality of life of patient in pain. This perspective subverts the classic way of assessing the effectiveness of therapy: whereas generally only objective parameters (clinical analyses) are evaluated in improving the patient's condition, medical anthropology starts with a goal (reduction of pain and improvement of quality of life) and evaluates every element that contributes to the achievement (even subjective factors, such as the patient's perception of treatment). This is the best way to implement humanized, personalized treatment plans that involve the patient, without reducing him or her to a passive object of therapy.
The Cryotherapy and Whole-Body Hyperthermia (WBH)
During the 1970s the first country in which the Whole-body cryotherapy was used for therapeutic scope was Japan, while in Europe, it has been used since 1984–1985, first in Germany. In WCB patients wearing minimal clothing are exposed to very cold and dry air (from −110 °C even to −160 °C for 1–3 min). The most important achievement was the decrease of pain and the amelioration of mobilization and rehabilitation. WBH, used as an add therapy to control the level of inflammation in rheumatic diseases, mitigates pain, and allows the patient to increase physical activity. Cryotherapy seems to downregulate the level of pro-inflammatory cytokines and consequently could be used in RA and other joint inflammatory diseases as an additional therapy to conventional or biological disease-modifying antirheumatic drugs (DMARDs), as well to corticosteroids, and nonsteroidal anti-inflammatory drugs (NSAIDs) in order to decrease the dosage of systemic pharmacological treatments minimizing the likely of severe related side effects. The effect of WBC on oxidative stress in healthy people and AS patients is under investigation, especially to establish and standardize treatment protocols. The WBC is composed by a cryochamber with a liquid nitrogen divided in two compartments connected by a door. Individuals are entirely exposed in WBC chambers, and the devices require a way to communicate visually and orally with the individuals. Moreover, there must be emergency stop buttons and exits. Cryotherapy has been used in the comprehensive treatment of patients with rheumatic diseases (especially arthritis, fibromyalgia, and ankylosing spondylitis) reducing pain and inflammatory symptoms through the regulation of the expression of cytokines. It is assumed that exposure to cold can stimulate the hypothalamic-pituitary-adrenal gland and sympathetic nervous system and increase the secretion of cortisol and catecholamines. An important role between neuroendocrine and immune system is played by cytokines; the interaction between hormones and cytokines may affect the immune response an important result in changing pain derives from the study of Klemm (fig 1).
Figure 1: Table Klemm. Serial WBC in fibromyalgia is effective and alters cytokine profiles.
Pain at the 12-week follow-up remained significantly below baseline values in the IG. Disease activity and functional capacity showed statistically and clinically meaningful improvement after intervention but were not significant at the 12-week follow up. TNF and IL-6 levels changed significantly in the IG. Eighteen of 31 (58%) patients of the IG reduced or discontinued analgesics at the 12-week follow-up. No WBC-related side effects were observed. Conclusions: The results seem to suggest that WBC in RA is able to reduce pain and disease activity significantly and in a clinically meaningful manner, as well as to decrease analgesic intake.
Intervention–WBC in a patient with Psoriatic Arthritis
Psoriatic arthritis is a chronic, immune-mediated, inflammatory arthropathy that presents with inflammation of the joints and entheses, including those of the axial skeleton, and is associated with increased mortality from cardiovascular disease. It affects the 30% of people psoriasis ant the 10% of the general population. Diagnosis is primarily based on clinical phenotype because of the diversity of the associated features, which can include skin and nail disease, dactylitis, uveitis, and osteitis. Cytokine inhibitors have been highly successful in the treatment of disease manifestations in several different tissues. However, the precise mechanisms underlying the pathogenesis of psoriatic arthritis-which include genetics, environmental factors, and immune-mediated inflammation are complex, and the relationship between disease of the joint and that of other domains is poorly understood.
The WBC is composed by a cryochamber with a liquid nitrogen divided in two compartments connected by a door, and the patient is dressed in shorts, t-shirt, gloves, woolen earmuffs, without any jewels, glasses, and contact lenses, standing in front of the specialist in direct visual contact through the glass of the chamber. The specific case studied on this trial, is a woman, 55 years old, affected by psoriatic arthritis. At the moment of clinical observation, she had 65 ESR (Erythrocyte Sedimentation Rate) and CRP (C-reactive protein), a positivity to anti-SSA/Ro (with a Sjogren Syndrome) and a deficiency of D vitamin. She was treated with MTX (methotrexate), that interferes with the normal functioning of cells, stopping them from dividing; it is a disease-modifying antirheumatic drug (DMARD) because it reduces joint inflammation. The MTX was given in 10mg every 10 days (30mg every month) combined with 5mg of cortisone, reduced to 2mg. In addition to the pharmacological therapy, she did 13 sessions of WBC (fig. 2).
Table 1: WBC treatment in 13 sessions.
| Sessions 1-2 | Time | Temperature |
| Compartment 1/pre-chamber | 1 min. | -25 C° |
| Compartment 2/ chamber | 3 min. | -80 C° (perceived -120 C°) |
| Sessions 3-13 | Time | Temperature |
| Compartment 1/pre-chamber | 30 sec. | -25 C° |
| Compartment 2/ chamber | 4 min. | -80 C° (perceived -120 C°) |
This integrative therapy improved the patient’s condition over 70%, with an objective and subjective improvement: the first one is attested by the stabilization of phlogosis indices, disappearance of symptoms and consequent reduction of drug treatment; the second one is the reduction of asthenia and improvement of the perception of quality of life.
Changing Pain
The contribution of WBC, combined with drug therapy, in the dialogue with the patient is of particular importance, both at the psycho-somatic and clinical level. First of all, one must look at the objective parameters (observable from the outside, fig.3): a change in ESR from 65 to 21, with a consequent lowering of the PCR, the almost total disappearance of the skin lesions and the consequent reduction of the pharmacological intake: MTX from 15mg to 10mg and cortisone from 5mg to 2mg.
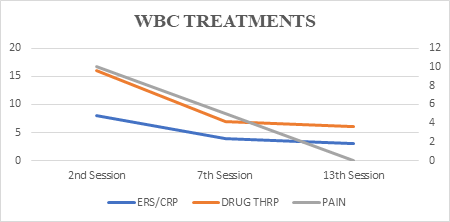
Figure 2: Objective parameters.
Regarding the subjective parameters, where 'subjective' does not mean a minor parameter, but concerns the point of view of the observer, which in this case is the patient, one must reflect on the question of pain and the impact it has on the patient. Pain becomes the element on which to focus in order to try to understand its complexity and function, especially in the economy of the patient's life and not only its symptomatology. Pain in rheumatology can have a mixed genesis, as happens for example when several problems are associated, not only rheumatological, or even nociplastic, which presents an alteration of nociception (the neurobiological systems involved in pain perception. The study in clinical observation needs to pay attention to the psycho-somatic experience, characterized by biological, affective, relational, spiritual, and cultural elements that are inseparably linked. Each person learns to express pain with categories derived from their own personal experience. Although pain is an experience shared by everyone, there is no exhaustive definition of it, even more so because it is not a simple neurophysiological response to a stimulus, but the result of the interaction of multiple factors: physiological, physiopathological, psychological, social, cultural, environmental, and memory (which inevitably plays a decisive role in modifying the algic sensation). On the basis of this complex conception of pain we move on to observe the specific case, from the inside, from the patient's point of view. It emerges from the conversation that the difficulty in walking, linked to psoriatic arthritis, introduces the patient into a gradual path of distancing herself from the world. This begins with the patient's estrangement from work, which is very often the primary place of sociability, the source of personal satisfaction, fulfilment, and social recognition. The long absence from work, the acute and persistent pain and the forced rest, introduce the patient into a state of isolation that interrupts social nourishment, creates a break in that circle of construction and reinforcement of one's own identity that is generated by social interaction. The relationship with others nourishes our identity because it is with what others send us back about ourselves that we know ourselves. Work, each person's creative capacity, and the allocation of a place in society somehow grants us a recognition of our existence; through work, society tells us and others that we exist. With the start of WBC sessions, the patient, already after the second session, reports "regaining life and energy". This experience (WBC) should first be observed in its most basic steps: the cryochamber is initially frightening, because it is an enclosed place, because it is beyond our control, because the cold is biting and penetrates our interior without any possibility of defence on our part. At the same time, however, the visual contact with the physiotherapist, the vocal stimulation telling us what movements to make, and the hope of improvement play a fundamental role. At the end of the cryotherapy, the patient says that she feels motivated again to resume first of all work and then the rest of her social relationships, so that WBC becomes the springboard to get out of the depressive state and start living again. Pain, the patient reports, has taken a back seat, it has become one of many elements to live with, it no longer becomes an illness, it is acceptable to such an extent that it no longer constitutes a problem. This point becomes fundamental from an anthropological point of view because it shows how clinical improvement and patient well-being do not always go hand in hand. In this specific case, then, the achievement of well-being was a key element in making the patient respond positively to treatment to the point of also achieving significant clinical improvement. In conclusion, this case study, in addition to the clinical evidence and therefore the objective improvement, helps us to understand how WBC, combined with drug therapy, can be a valid treatment tool. Cure becomes the sole objective of both medicine and medical anthropology, if it is understood not only as the statistical efficacy of the prescribed therapy, not only as the re-establishment of the inflammation indexes, but as the improvement of the patient's quality of life, as the ability to live with pain (which in rheumatology is often chronic), as the ability to return to "being well" (which does not always coincide with the absence of the disease).
References
- R. Bouzigon, F. Grappe, G. Ravier, and B. (2016). Dugue, “Whole- and partial-body cryostimulation/cryotherapy: current technologies and practical applications” Journal of Thermal Biology. (61)67-81.
Publisher | Google Scholor - Stanek A, Cholewka A, Gadula J, Drzazga Z et al. (2015). “Can whole-body cryotherapy with subsequent kinesiotherapy procedures in closed type cryogenic chamber improve BASDAI, BASFI, and some spine mobility parameters and decrease pain intensity in patients with ankylosing spondylitis?” Biomed Res Int.
Publisher | Google Scholor - Slattery K, Bentley D, Coutts AJ (2015). “The role of oxidative, inflammatory and neuroendocrinological systems during exercise stress in athletes: implications of antioxidant supplementation on physiological adaptation during intensified physical training”. Sports Med. 45(4):453-471.
Publisher | Google Scholor - Lubkowska, Z. Szyguła, D. Chlubek, and G. Banfi, (2011). “The effect of prolonged whole-body cryostimulation treatment with different amounts of sessions on chosen pro- and antiinflammatory cytokines levels in healthy men,” Scandinavian Journal of Clinical and Laboratory Investigation. (71) 5:419-425.
Publisher | Google Scholor - R. Bouzigon, F. Grappe, G. Ravier, and B. (2016). Dugue, “Whole- and partial-body cryostimulation/cryotherapy: current technologies and practical applications,” Journal of Thermal Biology. (61)67-81.
Publisher | Google Scholor - K. P. Braun, S. Brookman-Amissah, K. Geissler, D. Ast, M. May, and H. Ernst, (2009). “Whole-body cryotherapy in patients with inflammatory rheumatic disease. A prospective study”, Medizinische Klinik. (104) 3:192-196.
Publisher | Google Scholor - Veale DJ, Fearon U, (2018). “The pathogenesis of psoriatic arthritis”, Lancet. 391(10136):2273-2284.
Publisher | Google Scholor - M.AUGÉ – C. HERZLICH, (1986). Il senso del male: antropologia, storia e sociologia della malattia. Milano.
Publisher | Google Scholor - F.E. AGRÒ, (2000). Il trattamento del dolore: Atlante teorico-pratico. Roma.
Publisher | Google Scholor - F.E. AGRÒ, (1998). The semeiology of pain. Firenze.
Publisher | Google Scholor














