

case report
Recurrent Ceot of Maxilla- A Case Report
1Head and Professor of Department of Oral and Maxillofacial Surgery, KVG Dental College and Hospital Sullia, Karnataka.
2Professor of Department of Oral And Maxillofacial Surgery, KVG Dental College and Hospital Sullia, Karnataka.
3Consultant in oral and maxillofacial surgery VSM Multi-speciality Hospital Allappey, Kerala.
*Corresponding Author: Madhuri G Palekar,Oral and Maxillofacial Surgery in Dr.Kamal and R.N.Nayak Hospital Ankola
Citation: Kumar P, Mahabaleshwara, Sahya S Lal, Madhuri G Palekar. (2023). Recurrent Ceot of Maxilla- A Case Report. Dentistry and Oral Health Care, BRS Publishers 2(2); DOI: 10.59657/2993-0863.brs.23.009
Copyright: © 2023 Madhuri G Palekar, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 20, 2023 | Accepted: July 02, 2023 | Published: July 05, 2023
Abstract
CEOT is a rare benign, locally aggressive odontogenic neoplasm, that affects the jaw. This slow-growing neoplasm occurring as intraosseous (94%) and extraosseous (6%) variants and with a frequency of 1-2%. The presentation of both intraosseous and extraosseous types is similar and both have similar histological features. Intraosseous CEOT is more aggressive, with a reported recurrence rate of 14%. The intraosseous CEOT shows a maxilla: mandible site ratio of 1:2 and are mainly located in the premolar/molar region. Even though, maxillary neoplasms should be treated more aggressively because of their close proximity to vital structures than mandibular lesions. Treatment modalities varies depends on the tumour size, location and histology. This case report emphasizing the importance of treatment modalities for a rare recurrent case of CEOT of maxilla.
Keywords: neoplasm; jaw; mandibular lesions; tumour; maxilla
Introduction
There are 23 odontogenic tumors listed in the 4th edition of WHO classification of Head and Neck tumors. Among these, CEOT remains the benign epithelial odontogenic tumors subtypes. It is a rare benign odontogenic tumor that affects the jaw and with a variable biologic behavior ranging from mild to moderate invasiveness. In 1955, CEOT was described by a Dutch pathologist Jens Jorgen Pindborg. Later, pindborg tumor was first introduced to the literature in1967 to further describe this interesting and unique odontogenic tumor. It is a rare benign odontogenic tumor of locally aggressive behavior; it represents 1% of all odontogenic tumors. In 1971, the term “CEOT” was adopted by the WHO1. About 52% of cases are typically associated with an unerupted or impacted tooth.It shows a slow and asymptomatic growth and has more frequent in the posterior mandible.2,3. Mandible is affected 2 to 3 times more frequently than the maxilla, molar region of the maxilla/mandible being the commonly affected site. Recurrence rates for CEOT vary from 10% to 15% requiring periodic clinical and radiographic follow up. In this article we present clinical, radiological, histological and diagnostic findings and treatment modality of a rare case of recurrent CEOT in maxillary region with 10 years follow up.
Case Report
A 33-year-old female, presented to our institution with a diffuse swelling of right maxilla. Patient complaints of an asymptomatic swelling with approximately 4 months evolution, which was slowly increasing in size. Her past medical history was unremarkable with no evidence of systemic diseases. Extraoral examination revealed no facial asymmetry with absence of lymphadenopathy. Intra oral examination revealed a diffuse swelling extending from maxillary right first premolar to tuberosity and also extending in the vestibular-palatine direction of hard consistency, measuring approximately 4*3cm. Laterally the swelling obliterated the buccal vestibule and palatally did not cross the midline (Fig.1).

Figure: 1
Overlying mucosa was normal and both sensory and motor functions were preserved. FNAC and incisional biopsy were done. The histopathological analysis of the specimen was compatible with CEOT. Histopathology revealed polyhedral cells with hyperchromatic nucleus, prominent intercellular bridges, amyloid-like surrounding material and liesegang ring calcification were also seen. CT report showed well defined hyperdense region along with surrounding hypodense region extending to the right palatine and alveolar region. Also, expansion of the right buccal cortical plate with destruction is noted. Based on the clinical evaluation and histopathological findings,it was diagnosed as Calcifying Epithelial Odontogenic Tumor. Considering the age, esthetic concern and benign appearance, we proceeded with enucleation and curettage under GA. Interoperate, we noticed that lesion was not infiltrating too adjacent bone. After 12 months, patient presented with a diffuse swelling of right maxilla, which caused a moderate tumefaction of the right cheek and also complains of nasal obstruction and tearing. We repeated a biopsy and CT report showed an expansile hyper density seen in relation to right maxillary sinus with multiple focal areas of calcification, with obliteration of the right maxillary sinus and also it was extending to alveolar process (Fig.2).
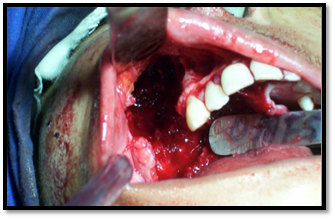
Figure: 2
Based on the previous history, clinical finding, radiographic imaging and histopathology we diagnosed it as a recurrent CEOT of right maxilla. Under GA, a subtotal maxillectomy was performed through weber Fergusson incision followed by defect reconstruction done with split thickness skin graft (Fig.3).
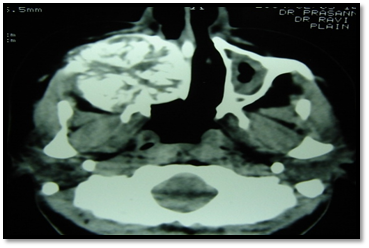
Figure: 3
Temporary obturator was prepared after initial healing of the surgical wound. Regular 10 years of follow up was done and there was no recurrence was noted.
Discussion
It is a well-known statement that CEOT can be locally aggressive and exhibit upto 15% recurrence rates, especially in cases treated by conservative approach. At first visit of our patient, she presented usual clinical features of painless, intraosseous slow growing mass. However, symptoms of maxillary tumor include pain, nasal obstruction, epistaxis, headache and proptosis. After 12 months of follow up, patient gave a history of nasal obstruction after the first conservative approach for the same. In our case, tumor arose from the anterior maxilla and then expanded to the maxillary sinus by the least path of resistance. Treatment options ranges from a simple enucleation to radical and extensive resection4. Even though, maxillary neoplasms should be treatFed more aggressively because of their close proximity to vital structures than mandibular lesions. Mandibular lesions could be approached more conservatively.5 Those treated with enucleation and curettage procedures showed recurrence rate after just 2-4 years of treatment and it was ranging from 15-30%. But patients treated with the resection approaches showed less recurrence when compared to the above mentioned. Therefore, the CEOT is best treated with resection using 1-1.5cm margins in the bone. It is always better when treatment options depend on size, site, histological features of the neoplasm and health status of the patient. Other investigations such as biomarkers can also be included. Cristina et al stated biomarkers helps in assessing the degree of local aggressiveness and even the malignant potential of odontogenic tumors. It also helps to choose the most efficient type of therapeutical approach.6 The forecast of the probable outcome requires minimum of 5 years and as many as 10 years may be necessary because of very slow growth of this tumor. Our case emphasizing the importance of regular follow up after a conservative approach even though CEOT is a benign tumor. If we neglect the follow up it can lead to serious intracranial involvement, that could severely complicate the life of patients.

Figure: 4

Figure: 5
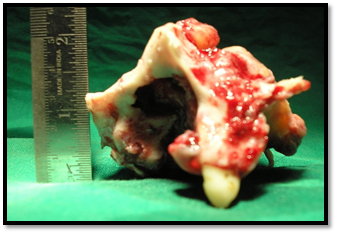
Figure: 6

Figure: 7
Conclusion
More recent reports have suggested that CEOTs are less aggressive. Conservative surgical resection with removal of a narrow rim of bone has recently been the recommended treatment. However, the size and extent of tumor determines the appropriate surgical procedure to be employed. It is also recommended to have tumors free margins in all directions.
References
- Pindborg JJ, Kramer IRH, Torloni H. (1971). Histological typing of odontogenic tumours,Jaw cysts, and allied lesions. International histological classification of tumours. 1st ed. Geneva: World Health Organization.
Publisher | Google Scholor - C.B. More, R. Vijayargiya. (2015). Intraosseous calcifying epithelial odontogenic (Pindborg) tumor: a rare entity, J. Oral Maxillofac. Pathol, 19:269.
Publisher | Google Scholor - O.H.G. Pereira, L.P.B. Carvalho, V.L. Brasileiro Júnior, C.R.L.V. (2013). Figueiredo, Calcifying epithelial odontogenic tumor, Case Rep. Pathol, 725380.
Publisher | Google Scholor - Franklin CD, Pindborg JJ. (1976). The calcifying epithelial odontogenic tumor. A review and analysis of 113 cases. Oral Surg Oral Med Oral Pathol, 42(6):753-765.
Publisher | Google Scholor - Nelson SR, Schow SR, Read LA, Svane TJ. (1992). Treatment of an extensive calcifying epithelial odontogenic tumor of the mandible. J Oral Maxillofac Surg, 50:1126-1131.
Publisher | Google Scholor - Lee CYS, Mohammadi H, Mostofi R, Hadidi A. (1992). Calcifyingepithelial odontogenic tumor of the maxillary sinus. J Oral Maxillofac Surg, 50:1326-1328.
Publisher | Google Scholor - Munteanu C, Pirici D, Stepan AE, Camen A, Margaritescu C. (2016). Maxillary calcifying epithelial odontogenic tumor with sinus and buccal vestibule extension: a case report and immunohistochemical study. Diagn Pathol. 11(1):134.
Publisher | Google Scholor











