

Research Article
Recurrence of Cardiac Myxoma in Familial vs Sporadic Cases
Harrington Heart and Vascular Institute, University Hospitals Cleveland Medical Center, Cleveland, OH, United States.
*Corresponding Author: Michel G Farah, Harrington Heart and Vascular Institute, University Hospitals Cleveland Medical Center, Cleveland, OH, United States.
Citation: Michel G Farah. (2024). Recurrence of Cardiac Myxoma in Familial vs Sporadic Cases, International Clinical Case Reports and Reviews, BioRes Scientia Publishers. 2(2):1-6. DOI: 10.59657/2993-0855.brs.24.019
Copyright: © 2024 Michel G Farah, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 10, 2024 | Accepted: August 26, 2024 | Published: August 28, 2024
Abstract
To evaluate recurrence of cardiac myxoma (CM) in familial and sporadic cases, serial echocardiograms were performed on 33 patients following surgical excision of cardiac tumors. There were 26 sporadic cases ages 20 to 78 and 7 familial cases ages 23 to 51 from two families. Follow up 1 to 20 years (average 8.8 years) revealed no recurrence in the sporadic cases. Recurrence occurred in 6 familial patients (88%) in 2 to 18 years. After 20004 and until the present time the study was extended to follow up of the familial patients with annual echocardiograms. Two familial patients had 2 recurrences and two had 5 recurrences each. In most familial patients the site of recurrence was in a different cardiac chamber. All CM were surgically excised successfully with no mortality.
Conclusion: Recurrence of CM is very rare in sporadic cases and very common in familial cases, often many years later and usually in a different cardiac chamber. Annual echocardiograms are recommended for follow up of familiar CM patients for life. Echocardiograms may be considered at longer intervals in sporadic cases.
Keywords: cardiac myxoma; sporadic cases; echocardiograms; cardiac chamber
Introduction
To study the incidence and characteristics of recurrence of cardiac myxoma (CM) in sporadic and familial cases serial echocardiograms were performed in both groups 1974-2004. After 2004 familial CM patients were followed annually for recurrence.
Methods
Between 1974 and 2004 33 patients at University Hospitals of Cleveland were followed up after excision of CM. Family members of the patients (parents, siblings or children) had echocardiograms performed to look for CM. Patients who had no family member with CM were classified as sporadic. Patients who had one or more family members with CM were classified as familial. Both groups were followed by serial echocardiograms on an annual basis at times based on availability. After 2004 and until 2022 the familial patients were followed on annual basis to detect the frequency and rate of recurrence of CM.
Results
There were 26 sporadic cases ages 20-78 years old (mean = 51 years). 22 had left atrial myxoma, 2 with right ventricular myxoma, one with left ventricular myxoma and one with tricuspid valve myxoma. All patients were operated successfully with no operative mortality. Follow up for 1-20 years (mean 8.8 years) revealed no recurrence of CM in the sporadic cases (Fig1). There were 7 familial CM patients ages 23-51 years old (mean = 28 years old). In Family I: a brother had right atrial myxoma and his siter had left atrial myxoma. In Family II the mother had biatrial myxomas, a daughter had biatrial myxoma, a son had left atrial myxoma, a son had right atrial myxoma and a second daughter had left atrial myxoma. Recurrence occurred in 6 familial patients (86%) in 1-18 years (mean 6.4 years) (Fig1). Tables I and II summarize the date and location of the recurrence in both families. In the familial patients, the site of recurrence was different from the original tumor and often in a different chamber in the majority of cases. All original and recurrent myxomas were surgically excised successfully with no mortality. Two familial patients were operated on 6 times. Figures 2 and 3 show the pedigree of Family I and Family II with number of original tumors plus recurrences and number of operations to remove the tumors.
Fig 4 shows the number of recurrences in familial cases and Fig 5 shows the interval between occurrence and recurrence of the tumors.
Fig 6 a (M-mode of LA tumor), b (TEE of RA tumor), and c (TEE of RV tumor) show the original tumor and recurrences of CM in the mother from Family II.
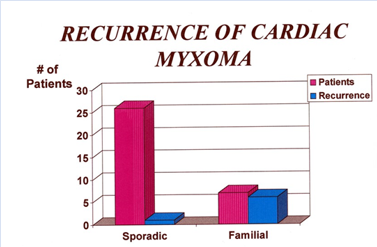
Figure 1: Recurrence of Cardiac Myxoma
Table 1: Family 1
| Date | Patient | Tumor Location | Recurrence | Operations |
| 1964 | Brother | Right atrium | 0 | 1 |
| 1975 | Sister | Left atrium | 0 | 1 |
| 1980 | Brother | Right atrium | 1 | 2 |
| 1983 | Sister | Left atrium | 1 | 2 |
Table 2: Family 2
| Date | Patient | Tumor Location | Recurrence | Total operations |
| Oct 1976 | Mother | Biatrial | 0 | 1 |
| Jun 1984 | Daughter 1 | Biatrial | 0 | 1 |
| Oct 1987 | Son 1 | Right atrium | 0 | 1 |
| Apr 1988 | Daughter 1 | Right atrium | 1st | 2 |
| Nov !988 | Mother | Right atrium, IVC | 1st | 2 |
| Nov 1988 | Son 2 (older) | Left atrium | 0 | 1 |
| Nov 1992 | Son 2 | Left atrium | 1st | 2 |
| Apr 1996 | Daughter 1 | Left atrium | 2nd | 3 |
| Aug 1996 | Son 2 | Right atrium | 2nd | 3 |
| Aug 1997 | Daughter 2 | Left atrium | 0 | 1 |
| Apr 1998 | Mother | Right ventricle | 2nd | 3 |
| Sep 1998 | Daughter 2 | Left ventricle | 1st | 2 |
| May 2000 | Daughter 1 | Left atrium | 3rd | 4 |
| Sep 2005 | Daughter 2 | Right ventricle | 2nd | 3 |
| Mar 2007 | Daughter 2 | Left atrium | 3rd | 4 |
| Nov 2010 | Daughter 1 | Right atrium | 3rd | 4 |
| Apr 2011 | Daughter 2 | LV lateral wall | 4th | 5 |
| Apr 20013 | Daughter 2 | LV inferior wall | 5th | 6 |
| Apr 20017 | Daughter 1 | Left atrium | 5th | 6 |
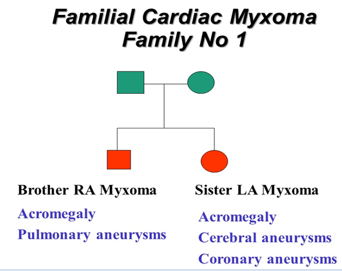
Figure 2: Pedigree of Family I
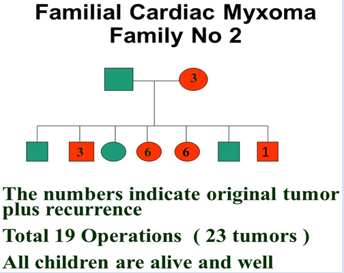
Figure 3: Pedigree of Family II
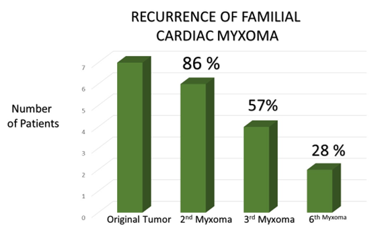
Figure 4: Number of recurrences in Familial cardiac myxoma
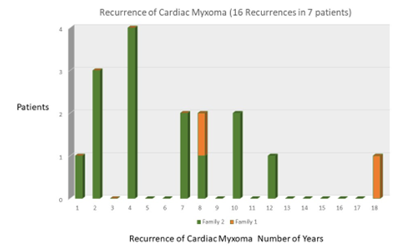
Figure 5: Interval of recurrence of familial cardiac myxoma
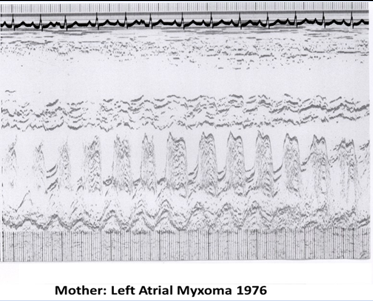
Figure 6a: Initial M-Mode echocardiogram of Mother
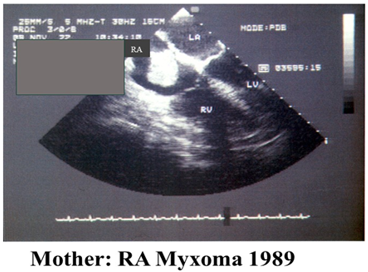
Figure 6b: Transesophageal echocardiogram of Mother
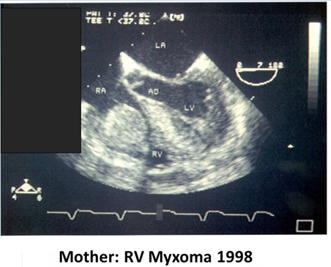
Figure 6c: Transesophageal echocardiogram of Mother
Discussion
Cardiac myxoma (CM) is the most common primary cardiac tumor and is benign if surgically removed before complications and usually fatal if untreated due to valve obstruction or embolic event. Familial cardiac myxoma is seen in younger individuals with more frequent right sided and multichambered involvement with occasional endocrine or skin disorder (1-4) In general recurrence in sporadic cases is rare and more frequent in familial cases (5-12) Recurrence in the same chamber in sporadic cases may also be due unsuccessful excision or seeding of the tumor. Recurrence in familial cases is more likely to be genetic since it commonly involves a different chamber and recurs after long intervals.
In our study none of the sporadic cases had recurrence yet it was very frequent in the familial cases (86%) Fig 1. Vascular aneurysms are reported in both sporadic and familial cases and are due to embolic events (13-17). In Family I the sister had left atrial myxoma with cerebral and coronary artery aneurysms and the brother had right atrial myxoma with pulmonary artery aneurysms. None of the patients in Family II had vascular aneurysms. This may also be due to the fact that the tumors were operated on as discovered in the study before any complications can occur. Also, no endocrine nor skin abnormalities were seen in Family II, Genetic evaluation of cardiac myxoma is limited by genetic heterogeneity (18.19) and at present has not been reported to detect recurrence of the myxoma tumors.
Recurrence in Family I occurred in the sister with left atrial myxoma 8 years later and in the brother with right atrial myxoma 16 years later, both in the same chamber (Table I). Recurrence in Family II occurred as follows: the mother presented with biatrial myxoma and congestive heart failure due to valve obstruction in 1976, recurrence occurred twice about 11 years apart involving different chambers, recurrence in the right atrium in 1988 and recurrence in the right ventricle in 1999 Fig 6 a, b, and c. She died at age 87 from noncardiac causes. One son had 2 recurrences, another son had none. Two daughters each had 5 recurrences in different chambers, and each had 6 operations to excise the tumors (Table II).
Recurrences in Family II were very frequent only discovered by annual echocardiograms as part of the study. Annual echocardiograms were normal between the detection of recurrence. Recurrence in familial CM in our study was in 1-18 years (Fig5). All Family II patients with recurrence were operated on when tumors were detected before any complications. Annual echocardiograms in Family II allowed detection of new cases and recurrences, Table II summarizes the dates and location of the original tumors and recurrences in Family II.
Conclusions
Recurrence of CM is very rare in sporadic cases and very common in familial cases. Recurrence in familial cases can occur many years later (in our patients 1-18 years) usually at a different site or chamber. Annual 2D echocardiograms in familial cases recommended to detect new cases and recurrence. Since the familial patients were studied annually the tumors were relatively smaller in size and were surgically removed before they grew to cause obstruction or embolization
Limitations
The study is limited by lack of previous large study on recurrence of cardiac myxoma for comparison and the literature is limited to case reports. It is also limited to not having a longer follow up of sporadic cases although to the best of our knowledge there were none. Further studies may be helpful to identify methods of detection of recurrent myxoma.
Recommendations
Annual 2D echocardiograms are recommended in familial cases to detect new cases and recurrence for life. Annual echocardiograms result in early detection of the tumors before symptoms and complications. Echocardiograms may be performed at longer intervals in sporadic cases, possibly 2-5 years.
References
- Carney JA. (1985). Differences between non-familial and familial cardiac myxoma. Am J Surg Path, 9:53-55.
Publisher | Google Scholor - Farah MGF. (1975). Familial atrial myxoma. Ann of Int Med, 83:858-860.
Publisher | Google Scholor - Farah MGF. (1994). Familial cardiac myxoma. A study of relatives of patients with myxoma. Chest, 105:65-68.
Publisher | Google Scholor - VanGelder HM, O’Brien DJ, Staples ED, Alexander JA. (1992). Familial cardiac myxoma. Ann Thorac Surg, 53:419-424.
Publisher | Google Scholor - Bjessmo S, Ivert T. (1997). Cardiac myxoma. 40 years’ experience in 63 patients. Ann Thorac Surg, 63:697-700.
Publisher | Google Scholor - Centofanti P, DiRose E, DeorsolaL, Dato GM Patane F, La Torre M et al. (1999). Primary cardiac tumors: early and late results of surgical treatment in 91 patients. Ann Thorac Surg, 6:1236-1241.
Publisher | Google Scholor - Pinede L, Dahout P, Loire R. (2001). Clinical presentation of left atrial myxoma. A series of 112 consecutive cases, Medicine (Baltimore), 80:159-172.
Publisher | Google Scholor - Smith JA, Davis BB, Stirling GR, Cooper E, Shardey GC, Goldstein J, Esmore DS, Monagle JP. (1993). Clinicopathological correlates of cardiac myxomas: a 30-year experience. Cardiovas Surg, 1(4) 399-402.
Publisher | Google Scholor - Loire R. (1996). Myxoma of the left atrium, Clinical outcome of 100 operated patients. Arch Mal Coeur Vaiss, 89(9):1119-1125.
Publisher | Google Scholor - St John Sutton MG, Mercier LA, Guiliani ER, Lie JT. (1980). Atrial myxomas: a review of clinical experience in 40 patients, Mayo Clin Proc, 55(6):371-376.
Publisher | Google Scholor - Mc Carthy PM, Piehler JM, Schaff HV, Pluth JR, Orezulak TA, Vidaillet HJ Jr, Carney JA. (1986). The significance of multiple recurrent and “complex” cardiac myxoma. J Thorac Cardiovasc Surg, 91:389-396.
Publisher | Google Scholor - Grauer K, Grauer MC. (1983). Familial atrial myxoma with bilateral recurrence. Heart Lung, 12:600-602.
Publisher | Google Scholor - Burton, C, Johnson J. (1970). Multiple cerebral aneurysms and cardiac myxoma. N Eng J Med, 282:35-36.
Publisher | Google Scholor - New PFJ, Price, DL, Carter B. (1970). Cerebral angiography in cardiac myxoma. Radiology, 96:335-345.
Publisher | Google Scholor - Geddes DM, Kerr IH. (1976). Pulmonary arterial aneurysms with right ventricular myxoma. Br J Radiol, 49:374-376.
Publisher | Google Scholor - Stock K. (2004). Multiple cerebral aneurysms in a patient with recurrent cardiac myxoma. Interventional Neuroradiology, 10:335-340.
Publisher | Google Scholor - Berbst M, Wattjies, MD et al. (2005). Cerebral embolism and left atrial myxoma leading to cerebral and retinal aneurysms. Am J Neuroradiology, 26:666-669.
Publisher | Google Scholor - Basson CT, MacRae CA, Korf B, Merliss A. (1997). Genetic heterogeneity of familial atrial myxoma syndrome (Carney Complex). Am J Cardiology, 79:994-995.
Publisher | Google Scholor - Milunsky J, Huang XL, Baldwin CT, Farah MG, Milunsky A. (1998). Evidence for genetic heterogeneity of the Carney complex (familial atrial myxoma syndromes). Cancer Genet Cytogenet, 106:173-176.
Publisher | Google Scholor













