

Case report
QRS Alternans During Treadmill Testing in A Case of Angina
Department of Cardiology, Mittal Hospital & Research Centre, Pushkar Road, Ajmer, India.
*Corresponding Author: S. R. Mittal, Department of Cardiology, Mittal Hospital & Research Centre, Pushkar Road, Ajmer, India.
Citation: S.R. Mittal. (2023). QRS Alternans During Treadmill Testing in A Case of Angina. Journal of Clinical Cardiology and Cardiology Research, BRS Publishers. 1(2); DOI: 10.59657/2837-4673.brs.23.007
Copyright: © 2023 S.R. Mittal, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 17, 2023 | Accepted: March 15, 2023 | Published: March 27, 2023
Abstract
A case of QRS alternans during immediate recovery phase of treadmill testing is reported. QRS alternans was associated with angina, significant ST-segment depression in multiple leads and ST-segment elevation in leads aVR & V1. Possible mechanisms are discussed.
Keywords: coronary artery disease; exercise electrocardiographic testing; electrocardiographic exercise testing; electrical alternans; qrs alternans; treadmill test
Introduction
Electrical alternans is an electrocardiographic finding defined as a change in the electrical activity of the heart in alternate beats in the presence of a regular rhythm [1]. All components of the P-QRS-TU complex can show alternans. QRS alternans is the commonest. It is frequently seen in the presence of sinus tachycardia and usually presents as aberrant (slow) conduction in the right bundle branch in alternate beats [2]. It does not have any clinical significance [3]. QRS alternans with sinus tachycardia, low voltage and nonspecific flattening of the T waves is a specific (but not sensitive) marker of pericardial effusion with tamponade physiology [4,5]. Paroxysmal tachycardia with narrow QRS complex and fast ventricular rate can also show QRS alternans. In such a clinical setting, QRS alternans is usually seen in atrio-ventricular reciprocating tachycardia. However, it can be seen in other narrow QRS tachyarrhythmias with fast ventricular rate. This finding does not have any independent clinical significance [6]. In the presence of acute ischemia, alternans usually affects repolarization [4] (ST-segment, T wave or U wave). T wave alternans preceding diagnostic ST-segment changes has been reported during treadmill stress testing [7]. We are reporting a case of QRS alternans during treadmill stress testing. To the best of our knowledge, this finding is not reported in the literature on exercise electrocardiography [8,9,10,11,12].
Case Report
A 73 years male presented for treadmill stress electrocardiography. He had history suggestive of angina on effort. Resting supine heart rate was 63 beats per minute. Resting supine blood pressure was 140/80 mm Hg. Resting supine electrocardiogram (Fig.1) was within normal limits except shallow inversion of the T wave in lead aVL (marked as ) and counter clockwise rotation in horizontal plane (RS configuration with positive T wave in lead V2). Patient could exercise only for five minutes (4.1 METs) because of development of chest pain. Peak heart rate was 130 beats per minutes (88% of the age predicted maximal heart rate using the formula of 220-age). Immediate recovery electrocardiogram in supine position showed more than 2mm ST-segment depression in leads I, II, aVF, V3, V4, V5 and V6 (Fig.2 and 3, marked as ). QRS amplitude showed alternans in leads I, II, III, aVL, aVF, V3, V4, V5 and V6 (Fig.2 and 3, marked as ‘a’ and ‘b’). ST-segment was elevated in lead aVR and V1 (Fig.2 and 3, marked as ).
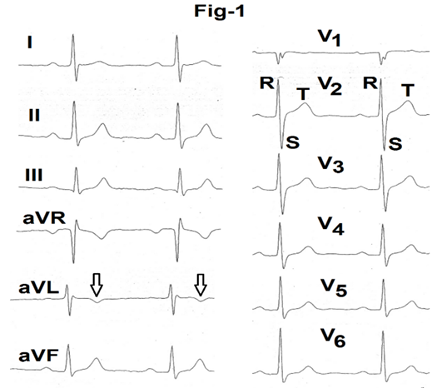
Figure 1: Resting supine electrocardiogram showing shallow inversion of the T wave in lead aVL (marked as ) and RS configuration with positive T wave in lead V2.
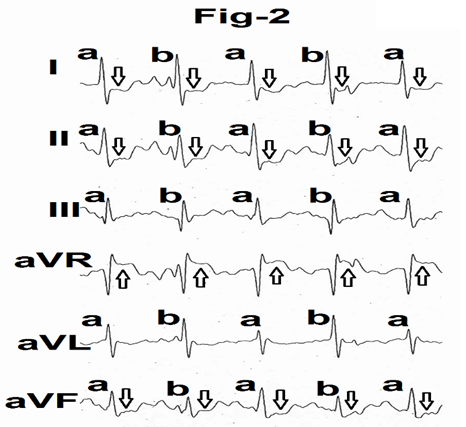
Figure 2: ECG (limb leads) recorded during immediate recovery showing ST-segment depression in leads I, II, aVF (marked as ) and ST-segment elevation in leads aVR with alternans in QRS amplitude in leads I, II, III, aVL, aVF (marked as ‘a’ and ‘b’ ).
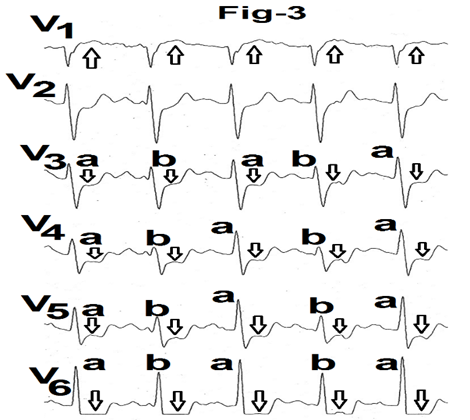
Figure 3: ECG leads V1 to V6 recorded simultaneously with limb leads showing QRS alternans with ST-segment depression in leads V3 to V6 and ST-segment elevation in lead V1.
Discussion
Significant ST-segment depression in more than six leads with elevation of the ST-segment in leads aVR and V1 at low workload and development of angina strongly suggest significant left main or multivessel disease [10,13-17]. ST-segment changes appearing only during recovery have some predictive power of angiographic coronary artery disease as ST-segment changes occurring during exercise [18,19]. It is, thus, clear that our patient had significant extensive myocardial ischemia.
There is no literature on QRS alternans during treadmill stress electrocardiography. It has been suggested that this electrocardiographic finding in the presence of an underlying organic heart disease may be accompanied by pulsus alternans [2] i.e., change in the volume of arterial pulse in alternate beats. Pulsus alternans generally occurs in severe heart failure and has been attributed to cyclic changes in intracellular calcium and action potential duration [20] (Figure 4). It is possible that severe extensive ischemia during exercise resulted in exercise induced left ventricular failure and consequent QRS alternans.
Another possibility is that severe ischemia results in ‘stunning’ of a large part of the myocardium [21] Such myocardium could take longer period to repolarise and may be excitable only at the time of alternate QRS complex (Figure 5). This may result in large QRS in alternate beats.
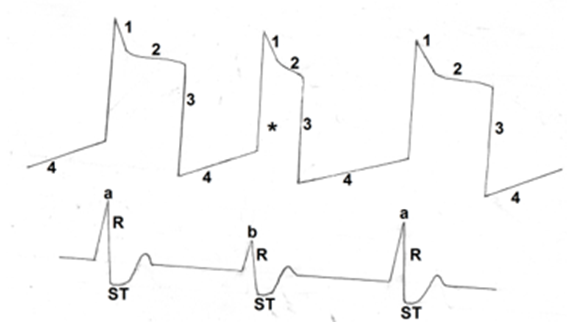
Figure 4: Line diagram of action potentials in alternate beats showing reduction in duration of action potential (marked as) as a cause of QRS alternans (marked a,b,a).
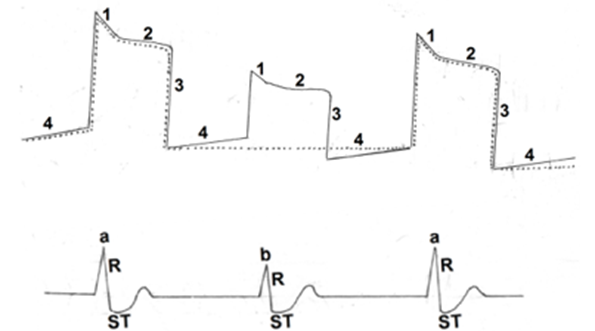
Figure 5: Line diagram of action potentials of all myocytes only in alternate beats (marked as ....) as a cause of QRS alternans.
Conclusion
QRS alternans with ST-segment depression in multiple leads could be suggestive of extensive myocardial ischemia and exercise induced left ventricular dysfunction.
References
- Chung DK, Chung EK. (1971). Ventricular electrical alternans. WV Med J, 67:99-100.
Publisher | Google Scholor - Mittal SR. (2005). Electrical alternans. Cardiology Today, 9:297-298.
Publisher | Google Scholor - Marriot HJL, Conover MB. (1998). Aberrant ventricular conduction. In: Marriot HJL and Conover MB (ed). Advanced concepts in arrhythmias. Mosby, St Louis, 215-236.
Publisher | Google Scholor - Mirvis DM, Goldberger AL. (2019). Electrocardiography. In: Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF. (eds). Braunwald’s Heart Disease, Philadelphia, 117-151.
Publisher | Google Scholor - De Luna GJ, Goldwasser D, Fiol M, Bayes-Genis A. (2017). Surface electrocardiography. In: Fuster V, Harrington RA, Narula J, Eapen ZJ. (eds). Hurst’s The Heart. Mc Graw Hill, New York, 252-317.
Publisher | Google Scholor - Surawicz B. (2008). QT interval, U wave abnormalities and cardiac alternans. In: Surawicz B (ed). Chou’s Electrocardiography in clinical practice. Saunders, Philadelphia, 569-585.
Publisher | Google Scholor - Mittal SR, Mittal G. (2022). T wave alternans preceding ST-segment depression as a sign of myocardial ischemia during treadmill test. I J Cardio & card diso, 3:1-4.
Publisher | Google Scholor - Thomas GS, Samtani SR, Ellestad MH. (2018). Interpretation of the ECG during exercise and recovery. In: Thomas GS, Wann LS, Ellestad MH. (eds). Ellestad’s Stress Testing. Oxford, UK, 160-198.
Publisher | Google Scholor - Schamroth L. (1988). Coronary insufficiency. In: Schamroth C. (ed). An introduction to Electro Cardiography. Blackwell Science. France, 157-185.
Publisher | Google Scholor - Surawicz B, Tavel M. (2008). Stress Test. In: Surawicz B. (ed). Chou’s Electrocardiophy in clinical practice. Saunders, Philadelphia, 157-185.
Publisher | Google Scholor - Balady GJ, Morise AP. (2019). Exercise electrocardiographic testing. In: Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF. (eds). Braunbwald’s Heart Disease. Elsevier, Philadelphia, 154-173.
Publisher | Google Scholor - Thomas GS, Ellestad MH. (2017). Electrocardiographic exercise testing. In: Fuster V, Harrington RA, Narula J, Eapen ZJ. (eds). Hurst’s The Heart. Mc Graw Hill, New York, 318-334.
Publisher | Google Scholor - Vorobiof G, Ellestad MH. (2011). Lead aVR: dead or simply forgotten? JACC- Cardiovasc Imag, 4:187-190.
Publisher | Google Scholor - Halon DA, Mevorach D, Rodeanu M, Lewis BS. (1994). Improved criteria for localization of coronary artery disease from the exercise electrocardiogram. Cardiology, 84:331-338.
Publisher | Google Scholor - Weiner DF, Mc Cabe C, Hueter RC, Ryan TJ, Hord WB Jr. (1978). The predictive value of anginal chest pain as an indicator of coronary disease during exercise testing. Am Heart J, 96:458-462.
Publisher | Google Scholor - Colby J, Hakki AH. Iskandrian AS, et al. (1983). Hemodynamic, angiographic and scintigraphic correlates of positive exercise electrocardiograms: emphasis on strongly positive exercise electrocardiograms J Am Coll Cardiol, 2:21-29.
Publisher | Google Scholor - Blumenthal DS, Weise JL, Mellitis ED, et al. (1981). The predictive value of a strongly positive stress test in patients with minimal symptoms. Am J Med, 70:1005-1010.
Publisher | Google Scholor - Goldschlager N, Selzer A, Coha K. (1976). Treadmill stress test as indicators of presence and severity of coronary artery disease. Ann Intern Med, 85:277-286.
Publisher | Google Scholor - Lachterman B, Lehmann HG, Abrahamson D, Froelicher VF. (1990). Recovery only ST-segment depression and the predictive accuracy of the exercise test. Ann Intern Med, 112:11-16.
Publisher | Google Scholor - Fong JC, O’ Gara PT. (2019). History and physical examination: An evidence-based approach. In: Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF. (eds). Brauwald’s Heart Disease, Philadelphia, 83-101.
Publisher | Google Scholor - Udelson JE, Dilsizian V, Bonow RO. (2019). Nuclear cardiology. In: Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF. (eds). Braunwald’s Heart Disease, Philadelphia, 261-300.
Publisher | Google Scholor














