

Case Report
Prominent Eustachian Valve Complicated by Thrombus
- S. Lehachi
- M. Chettibi
- H. Kalkoul *
Cardiology department of Benimessous, Algiers, Algeria.
*Corresponding Author: H. Kalkoul, Cardiology department of Benimessous, Algiers, Algeria.
Citation: H. Kalkoul, S. Lehachi, M. Chettibi. (2023). Prominent Eustachian Valve Complicated by Thrombus. Clinical Case Reports and Studies, BRS Publishers. 2(6):1-3. DOI: 10.59657/2837-2565.brs.23.058
Copyright: © 2023 H. Kalkoul, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 17, 2023 | Accepted: July 31, 2023 | Published: August 07, 2023
Abstract
The Eustachian valve is an embryological remnant of the valve of the inferior vena cava. It may be prominent in some individuals, but the echocardiographic appearance of a divided right atrium (RA) as a result of a large Eustachian valve is rare. Sometimes it presents a problem of differential diagnosis with other embryonic remnants of the right atrium, such as the Chiari network. It may be complicated by thrombosis or infective endocarditis. Cardiac imaging plays an important role in diagnosis.
The aim of this review is to discuss a rare form of Eustachian valve complicated by thrombosis.
Keywords: eustachi valve; thrombus; embolic complication; cardiac imaging; anticoagulant treatment
Introduction
The Eustachian valve is an embryological vestige of the valve of the inferior vena cava (IVC). It is usually absent or inconspicuous and has no known function in normal adults. However, in rare cases, a persistent eustachian valve may be associated with thrombus, infective endocarditis or tumor [1, 2].
We report here a case of recurrent pulmonary embolism of an adherent thrombus on a prominent Eustachian valve.
Observation
Mrs F. R aged 48, followed for uterine fibroma (minimal metrorrhagia) treated with progestogen and dicone. In 2021, dyspnea with cough appeared, which prompted the patient to consult a private practitioner, who treated her as having a pulmonary infection. A month later, the patient had not seen any clinical improvement, especially the persistence of dyspnea, she reconsulted a pulmonologist who did a D-dimer test which was positive. In this context, a pulmonary Angio scan showed a left segmental and sub-segmental pulmonary embolism (PE) at high intermediate risk. She was treated with heparin therapy, followed by anti-vitamin K (AVK), and she refused oral anticoagulants ("OACs"). Transthoracic Echocardiography (TTE) performed during hospitalization revealed a floating mass in the right atrium (RA) suggestive of a benign tumor, thrombus, metastasis, Chiari network, or just a prominent eustachian valve (Figure 1). The investigation was completed with a transesophageal echocardiography (TEE) which showed a prominent Eustachian valve on which a thrombus had been inserted (Figure 2). For a better tissue analysis, a cardiac MRI was performed, which showed an intra-RA mass suggestive of a thrombus on the eustachian valve. Surgery vs anticoagulant treatment was discussed, but it was decided to maintain the anticoagulant treatment with regular TTE/TEE checks every 03 months. A follow-up TEE after one year's treatment (TRT) showed a clear disappearance of the thrombus. better visualized in 3D TEE. The final diagnosis was a voluminous Eustachian valve complicated by thrombus.
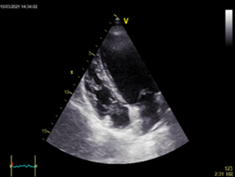
Figure 1: TTE section 04 cavities shows the mass at the level of the RA.

Figure 2: Objective TEE image of Eustachi's valve with thrombus.
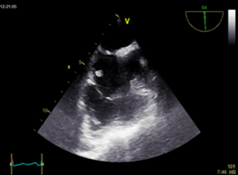
Figure 3: TEE image shows disappearance of the thrombus after one year of TRT, with persistence of a prominent Eustachian valve.
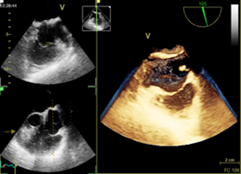
Figure 4: An objective 3D TEE image of the Eustachian valve and its spatial relationships.
Discussion
The Eustachian valve is named after the famous Italian anatomist Bartolomeo Eustachi, who described it for the first time in the mid-sixteenth century [1]. In the majority of adults, the Eustachian valve is either barely visible or appears as a thin, crescent-shaped endocardial fold originating at the orifice of the IVC [2]. This valve directs blood flow in the fetal circulation from the vena cava through the foramen oval into the left atrium. The persistence of this valve in adults is rare. However, there is great variability in the size, shape, thickness, texture, length and extent of the persistent eustachian valve [2, 3]. Whatever its size, a persistent eustachian valve is generally non-pathological and does not need to be treated in the absence of associated cardiac abnormalities [1, 2]. Rarely, a prominent Eustachian valve may cause obstruction at the IVC-RA junction or increase right-to-left shunting in infants with atrial septal defects. Eustachian valve thrombosis is extremely rare but has been reported in rare cases [1, 2].The thrombus may arise in situ or may result from adhesion of embolic material from a distant source. In both cases, the risk of embolization is significant [1, 2] [as in our patient's case]. Endocarditis of the eustachian valve is extremely rare, usually seen in intravenous drug users [4, 5, 6]. A review of the English literature using Medline from 1966 to the present revealed only 5 cases of Eustachian valve endocarditis [4]. Myxoma of the right atrium is uncommon, accounting for around 15-20% of cases. Generally, these tumors arise from the atrial septum. Very rarely, they arise either from the IVC or its junction with the right atrium, or from the Eustachian valve [7]. Although transthoracic echocardiography is still considered the most important diagnostic imaging method for cardiac tumor, it most often fails to confirm the diagnosis [3], hence the need to complement this examination with TEE. TEE appears to be superior to TTE in detecting Eustachian valve pathology and should be considered in all such patients [5, 6]. Analysis of the Eustachian valve using 3D TEE offers better spatial resolution [8]. Other imaging tests such as cardiac MRI can confirm the diagnosis.
Conclusion
The Eustachian valve can present voluminous forms in certain individuals, complications such as thrombus formation on the Eustachian valve are rare. Thrombus can form directly on the valve, with the risk of embolization. Anticoagulant treatment in these situations resolves this problem. The role of cardiac imaging, particularly TEE and cardiac MRI, in diagnosing and monitoring this type of complication is crucial.
Conflicts of Interest
No conflicts of interest
References
- Jolly N, Kaul UA, Khalilullah M. (1991). Right atrial thrombus on eustachian valve - successful lysis with streptokinase. Int J Cardiol., 30(3):354-356
Publisher | Google Scholor - Maddury J, Alla VM, Misra RC, Maddavapeddi A. (2009). Thrombus on the eustachian valve leading to recurrent pulmonary embolism: a rare problem requiring aggressive management. Can J Cardiol., 25(12):e422-423.
Publisher | Google Scholor - Limacher MC, Gutgesell HP, Vick GW, Cohen MH, Huhta JH. (1986). Anatomie échocardiographique de la valve d'Eustache. Am J Cardiol, 57:363-365.
Publisher | Google Scholor - Bowers J, Krimsky W, Gradon JD. (2001). The pitfalls of transthoracic echocardiography. A case of eustachian valve endocarditis. Tex Heart Inst J., 28(1):57-59.
Publisher | Google Scholor - James PR, Dawson D, Hardman SM. (1999). Eustachian valve endocarditis diagnosed by transoesophageal echocardiography. Heart, 81(1):91.
Publisher | Google Scholor - Palakodeti V, Keen WD Jr, Rickman LS, Blanchard DG. (1997). Eustachian valve endocarditis: detection with multiplane transesophageal echocardiography. Clin Cardiol., 20(6):579-580.
Publisher | Google Scholor - Teoh KH, Mulji A, Tomlinson CW, Lobo FV. (1993). Right atrial myxoma originating from the eustachian valve. Can J Cardiol., 9(5):441-413.
Publisher | Google Scholor - Takahiro Yonekawa, Yoshihide Mitani. (2010). Three-Dimensional Echocardiographic Imaging of a Giant Eustachian Valve in an Infant with Reversed Cyanosis. Pediatr Cardiol, 31:1114-1115.
Publisher | Google Scholor













