

Research Article
Prevalence of Dental Malocclusion and Its Gender Distribution Among Dental Students at Kabul University of Medical Science
- Hedayatullah Ehsan *
- Mashal Azami
- Shamila Azimi
Orthodontics Department, Kabul University of Medical Sciences, Kabul, Afghanistan.
*Corresponding Author: Hedayatullah Ehsan, Orthodontics Department, Kabul University of Medical Sciences, Kabul, Afghanistan.
Citation: Ehsan H, Azami M, Azimi S. (2023). Prevalence of Dental Malocclusion and Its Gender Distribution Among Dental Students at Kabul University of Medical Science. Dentistry and Oral Health Care, BRS Publishers 2(1); DOI: 10.59657/2993-0863.brs.23.004
Copyright: © 2023 Hedayatullah Ehsan, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 29, 2023 | Accepted: April 12, 2023 | Published: April 19, 2023
Abstract
Aim: The current study aims to provide quantitative and qualitative information about the prevalence of dental malocclusions among dental students of Kabul University of Medical Sciences (KUMS) in the orthodontics department of Ali Abad Teaching Dental Clinic that evaluates the relationship of malocclusion between gender and the major causes of malocclusion in society among genders and the tendency of the community toward the treatment of dentoalveolar anomalies.
Methodology: This study was a cross-sectional survey which has been done randomly among 133 students, 68 male (51.12%) and 65 female (48.87%); in an age range of (18-25) years old at Kabul University of Medical Sciences, Ali Abad teaching dental clinic faculty of Dentistry.
Results: It displays the different "Angle" grades of dental malocclusion for males and girls. For men, the classifications are Class I (48.33%) Class II (6.66%) Class III (43.33%). Males experienced crowding at a rate of 33% while females experienced it at a rate of 43%. Dental caries (53.84%) was shown to be the most prevalent oral condition in females after extensive research and analysis. No one in our survey (65 female participants) reported having periodontitis, compared to men who had dental plaque at rates of 28.97% and 6%, respectively, and gingivitis.
Conclusions: The most significant contributing factor to dental malocclusion in boys may be dental trauma, while in girls it may be inheritance. Because girls tend to value beauty more than boys do, they were more interested in orthodontic procedures. Moreover, participants' rates of crowding, deep, open bites, and edge-to-edge bites were highest.
Keywords: malocclusion; Angle’s classification; dental caries; dental plaque; gingivitis
Introduction
The contact of the upper and lower teeth in all mandibular postures and movements is known as occlusion. Angle formerly given various categories, of which classification based on the connection between the first permanent molars is currently employed. This classification allows for the division of occlusion into three groups: The usual alignment of the upper and lower first permanent molars is Class I. The lower first permanent molar in this class is positioned anterior to the corresponding upper tooth by roughly a tooth width. The lower first permanent molar and additional lower teeth are positioned more anteriorly in class III than they are in class II, where both positions are more posterior. Although malocclusion is not a life-threatening disorder, it can negatively impact a patient's social connections and psychological well-being. Because to its great prevalence, malocclusion is now regarded as the third-highest oral health priority due to its impact on public health [1,2]. “An irregularity of the teeth or an abnormal relationship between the dental arches that goes beyond what is considered to be normal is referred to as a malocclusion” [3]. Malocclusion is one of the most common dental problems as well as dental caries, periodontal disease, and dental fluorosis [4]. Malocclusion has a multifaceted etiology that includes environmental influences like oral habits, social traits, and diet in addition to inherited elements like certain stimulation during the formation and development of orofacial structures [7,8,9].
In the majority of investigations, a range of 20% to 80% malocclusion has been recorded. Due to the many ethnic groups, age groupings, and registration processes, there is such a vast variation[10,11]. In the study conducted by Proffit et al., in the USA, almost 30% of people have normal occlusion, and the prevalence of Class I malocclusion was between 50–55%. The majority of Class II and Class III malocclusion is about 15% and <1 href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5090996/#ref12">12]. Another study in Denmark has reported the prevalence of typical malocclusion as 14%, Class I malocclusion at 58%, Class II malocclusion at 24%, and Class III malocclusion at 4% [13]. The majority of typical malocclusion was reported to be 7.1%, Class I malocclusion was 58.8%, Class II malocclusion was 21.5%, and Class III malocclusion was 12.6% among Chinese people living in Australia [14].
Malocclusion is currently the third most prevalent dental condition worldwide, after periodontal and dental cavities. Malocclusion is a multifactorial issue as a result of various factors, including; In mixed and permanent dentitions, caries and the early loss of primary teeth are thought to be risk factors for occlusal and spacing irregularities [15].
A survey in India revealed that the prevalence of crowding is 50.4% in boys and 51.4% in girls. Relevant research was conducted in different nations to investigate the majority of dental malocclusion and its similar features in terms of gender. In both boys and girls, cross-bite was found at 17.8% and 18.3%, respectively. 78.4% of boys and 80.2% of girls reported having class I malocclusion. 21.5% of boys and 19.8% of girls were found to have class II malocclusion, and 0.1% of boys had class III malocclusion. The most frequent symptom was crowding, which was followed by an enhanced overjet, a deep bite, and an anterior open bite in that order. Nevertheless, the most frequent trait in a different survey conducted by Pakistan's Agha Khan University was increasing overjet. According to this study, women were expected to have more class 1 students than men. The survey revealed that the treatment of malocclusion enhances oral health-related quality of life.
Furthermore, the lack of sufficient studies and research on oral health, particularly dental malocclusion that takes gender into account, is a major problem in Afghanistan because these conditions—poverty, conflict, and social inequality in terms of living standards—are known to have a negative impact on oral health.
Research objectives
- To find out the prevalence of dental malocclusion in both gender males and females.
- To identify the significant causes and problems of dental irregularities.
- To demonstrate the tendency of both genders for treatment of dental malocclusion.
Methodology
The study and approval to survey dentistry students were approved by Kabul University of Medical Sciences' ethical committee. Also, the University Hospital's management and employees gave their consent.
This cross-sectional survey was conducted in 2020 at Kabul University of Medical Sciences' faculty of dentistry among 133 students, 68 males (51.12%) and 65 females (48.87%), ranging in age from 18 to 25.A survey with both qualitative and quantitative questions served as the research methodology. At Kabul University of Medical Sciences, 140 questionnaires were distributed to dentistry students from 20 September to 20 November as part of the data collection process. Twelve multiple-choice and two-point scale questions made up each questionnaire. The surveys were given to the participants once they had given their consent.
To prevent inter-examiner differences, only one examiner evaluated the students. The Orthodontics department at Ali-Abad Teaching University provided clinical calibration training for the examiner and record assistant prior to the survey. Also, under the supervision of orthodontics professionals, their mouths and teeth were inspected for the presence of dental malocclusion class I, class II, and class III categorization based on angle's definition in students.
The observation was written down on the evaluation form and then entered into the computer. Based on the data in the files, dental bites and other oral data associated to participants were extracted.
The dataset underwent preprocessing to remove outliers and missing values before analyses. Excel is the program used for all charts and analytics.
Inclusion criteria
- Age group between 18-25 years.
- Students who have enough teeth in their jaws.
- Students who are willing to participate in the research and are satisfied.
- Students of dentistry faculty. This criterion was related to the research objective because conducting the survey was easier on dental students than on other faculties' students.
Exclusion criteria
- Age group out of 18- 25 years.
- Students who have lost their teeth for various reasons.
- Students who are not satisfied with the research.
- Students of other faculties except for dentistry faculty.
Result
Among the 133 individuals who met the requirements for the sample and were approved to take part in the study, "68" of them were men, "and 65" were women with ages ranging from 18 to 25.
Table 1: Gender distribution
| Total no. of subjects (N) | N (%) | |
| Male | 68 | 51.12 |
| Female | 65 | 48.87 |
| Total | 133 | 100 |
There were 51.1%, 14.3%, and 33.9%, respectively, of Angle's class I, II, and III malocclusions. There was a statistically significant difference in the malocclusion. (Table 2)
According to research, males' class I (48.33%), class II (6.66%), and class III (43.33%) dental malocclusion classes are classified according to "angle" in females' class I (53.48%), class II (21.4%), and class III (23.07%) while it is classified according to "angle" in males' class I (48.33%), class II (6.66%), and class III (43.33%).Table 2: Distribution of angles’ classes due to gender
| Angle’s Classes | |||
|---|---|---|---|
| Gender | Class 1 | Class 2 | Class 3 |
| Male | 48.33% | 6.66% | 43.33% |
| Female | 53.84% | 21.53% | 23.07% |
| Total | 51.1% | 14.3% | 33.9% |
The results are then evaluated in terms of "causes (hereditary, trauma), gender, blood types, the psychological and aesthetic impact of malocclusion, and interest in treatment.
A number of contributing factors, including crowding, concussion, inheritance, gender, blood types, harmful oral behaviors (including mouth breathing, bruxism, nail-chewing, thumb-sucking, and tongue- thrusting), and oral issues, were documented and discovered in this study. It has been demonstrated that malocclusion is related to each of these elements both directly and indirectly. The following figures and tables each provide a description of one of these key factors. For instance, the connection between the ABO blood group system and malocclusions, which will be covered in depth in the blood groups factor, is one of the most fundamental aspects of human genetics.
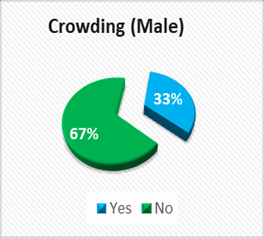
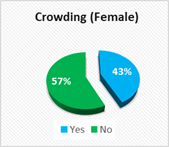
Pie Chart 1&2: show the speed of crowding in males (33%) and females (43%).
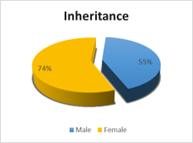
Pie Chart 3
Shows the existence of dental malocclusion among their family members and relatives, which describes the role of inheritance (74%) in girls and (55%) boys, the 23% difference indicates that inheritance in females is one of the significant factors in causing dental malocclusion because more than one member of the family has the same condition.
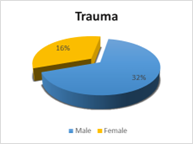
Pie Chart 4
Explains trauma during childhood in primary teeth of both genders. It describes the incidence of trauma in deciduous teeth during their childhood (16%) in females and (32%) in males.
It has been studied and analyzed for Oral problems separately. In females, the most oral problem was dental caries (53.84%). In males, the most common problem was dental plaque (28.97%) and the least were Gingivitis (6%) in females, and (4.67%) in males, respectively Table (3).
Table 3: Oral problems
| Oral Problems | Male | Female |
|---|---|---|
| Calculus | 16.82% | 21.53% |
| Caries | 28.04% | 53.84% |
| Dental plaque | 28.97% | 20% |
| Gingivitis | 4.67% | 6% |
| Periodontitis | 8.41% | 0% |
| Non-Existing Oral Problems | 9.34% | 24.61% |
Each gender's prevalence of these poor oral habits has been investigated and assessed independently. Bruxism (18.46%) was the most prevalent negative habit among girls. Mouth breathing (14.06%) was the unhealthy practice that affected men the most frequently Table (4).
Table 4: Bad oral habits
| Bad Oral Habits | Male | Female |
|---|---|---|
| Mouth breathing | 14.06% | 7.69% |
| Bruxism | 7.81% | 18.46% |
| Nail chewing | 3.125% | 1.53% |
| Thumb sucking | 1.56% | 3.07% |
| Tongue thrust | 0% | 1.53% |
| Nothing | 73.437% | 73.84% |
In the population that was investigated, a normal bite (2-4 mm) was observed in 63.9% of the males and 64.61% of the females. Similar to deep bites and increasing bites, open bites were observed in 10.5% of patients and 15.3% of cases, respectively. Statistics showed that the data was significant Table (5).
Table 5: Dental bites
| Dental Bites | Male | Female |
|---|---|---|
| Normal bite | 63.33% | 64.61% |
| Deep bite | 11.66% | 18.46% |
| Open bite | 10% | 7.69% |
| Crossbite | 0% | 1.53% |
| Edge to Edge Bite | 15% | 0% |
Also, based on the study's findings, it is determined that blood group types O and B in both sexes are important contributing factors to malocclusion, or that there is a connection between them. In reality, table (6) simply shows the prevalence of blood groups among participating pupils; more information about how these blood groups relate to malocclusion is covered in the discussion section Table (6).
Table 6: Blood groups
| Blood Groups | Male | Female |
|---|---|---|
| A | 22.7% | 15.3% |
| B | 34.8% | 30.7% |
| O | 36.3% | 36.9% |
| AB | 6% | 10.7% |
The impact of malocclusion on people of both sexes should be considered as a separate problem. Males experience extremely high impact (33.3%), medium impact (33.3%), and shallow impact (33.3%) in comparison to females' very high impact (26%), medium impact (40%), and very low effect (34%) rates.
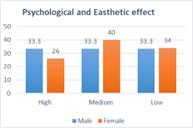
Graph 1
Graph (1) describes the percentage of psychological and aesthetic Effects of dental malocclusion on both genders.
Based on our study, it has shown that each gender has its inclination for treatment of this teeth irregularity. 64.4% out of 65 females, wanted to be treated immediately without any financial consideration – a valuable issue for them, (7.6%) were not interested to seek treatment, and (4.6%) didn't want to treat this irregularity means that it is not essential for themselves. While in males, 45.4% out of 68 wanted to treat this teeth irregularity as soon as possible – a valuable issue for them, (9%) were not very interested in treatment. It has cleared based on this finding that a high percentage of girls are willing in seeking treatment without any financial problems or anything else rather than boys Graph (2).
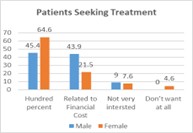
Graph 2: Shows the interest of participants in treatment in a percentage
Discussion
In each country, the majority of malocclusion is different. For example; in Saudi Arabia, its prevalence is 62.4%, in Colombia 88.1%, and in the United States, the prevalence is 20-43%. [26] While the range of this prevalence in India is 20–43% [27]. So, these variations will help us to find the leading factors of malocclusion.
The prevalence of each Angle’s class is also different. In Europe and Africa, the prevalence of Angle’s class 1 was in a wide range between 10.3-84.3% [28-37]. In our study, the percentage of class 1 malocclusion among Afghan students was 51.1%, which is a similar finding to studies in Pakistan and Iran with approximately 54.7% [28-37].
Angle's class 2 prevalence in Afghanistan is more comparable to that in Pakistan, Iran, and India. Nonetheless, class 3 malocclusion is not common in Afghanistan, and this finding of our study is also consistent with studies from Iran, Pakistan, and India [28-37]. Because of these parallels and the resulting findings, we can infer that racial, cultural, climatic, dietary, ethnic, and genetic similarity also leads to the same results.
The association between dental malocclusion and a number of variables was investigated. In terms of trauma, this study revealed that males were more likely to experience concussions (32%) than females (16%), which is consistent with Rohini Dua and Sunila Sharma's study's result that males were more likely to get concussions (63%) than females (36.4%). [38] Another element that can contribute to it is inheritance, and this survey revealed that among the kids who had malocclusion, most or all of their relatives also had the disease, which suggests heredity. Blood grouping systems play a part in this analogy; an Indian study found a connection between malocclusion and the blood grouping system. [39] Also, based on the findings of this study, it is determined that the presence of blood group types O and B in both sexes, as well as oral trauma in men and inheritance in women, may be the most important causes for dental malocclusion among the participants.
Research conducted in India found that crowding affected 50.4% of boys and 51.4% of girls, and that cross-bite affected 17.8% and 18.3% of boys and girls, respectively. In this study, crowding was more common in boys (67%), whereas it was more common in girls (57%), although crossbite was only detected in girls (1.53%) and not in boys. In boys and girls, class 1 malocclusion was observed at 78.4% and 80.2%, respectively. 21.5% of boys and 19.8% of girls reported having class II malocclusion, and 0.1% of boys were recognized for having class III malocclusion. While in this survey, girls (53.8%) and boys (48.3%) both had class 1 malocclusions. Class III has 43.3% of boys and 6.6% of girls in it (class II). In another study, crowding predominated, followed in that order by increased overjet, deep bite, and anterior open bite. Following the deep bite, open bite, and edge-to-edge bite, participants' rates of crowding were highest in this study. In Pakistani research, it was noted that women received more class 1 results than men. In this study, it was found that girls also had a higher percentage of class 1 than males.
While the rate of bruxism in females is more prevalent than other oral behaviors, dental caries is more widespread in both sexes than other oral issues. However, a number of other factors, such as dental plaque, which causes gingivitis, might result in malocclusion; hence, it's possible that there is a direct link between dental plaque and gingivitis. Our research suggests that there may be a connection between mouth breathing and dental health issues including caries and gingivitis, as well as between an open bite and class I and class II malocclusion. It is more challenging to clean the teeth when there are irregularities in the teeth. Hence one of the primary causes of dental caries, dental plaque, and calculus, which are seen in both sexes, is food that has been left in the teeth for an extended period of time. Hence, dental carries may be caused directly by tooth abnormalities.
Table 7: It shows the probable relation between causal factors and their effect on oral health.
| Causes | Effects |
|---|---|
| Bad Oral Habits, Bruxism, Nail Chewing, Thumb Sucking, Tongue Thrusting | Open bite |
| Bruxism | Periodontitis |
| Dental Plaque | Gingivitis |
| Mouth Breathing | Caries, Gingivitis |
| Class 2, Class3 | Open bite |
| Edge to Edge Bite | Class 1 |
| Open bite, Class 2, Class 3 | Mouth breathing |
Table 7: Causal factors and their effects
According to this study, women participants are more interested in treatment and experience less psychological impact from dental anomalies than men. The findings of this study show that girls seek treatment 20% less frequently than boys do because girls place a higher value on attractiveness.
Based on the causes and the existence of an unequal number of participants in terms of gender, the current survey and Table (8) show that there were significant differences between the prevalence of dental irregularities in girls and boys. Obviously, we are unable to determine which gender was more or less affected by these irregularities.
Table 8: Prevalence of Dental Malocclusion in Both Sexes According to Its Mean
| Male | Female | |
|---|---|---|
| Angles Classes | 32.77% | 36.19% |
| Oral Problems | 17.38% | 20.27% |
| Dental Bites | 20% | 8.46% |
| Bad Oral Habits | 5.31% | 6.46% |
| Dental Crowding | 33% | 43% |
| Overall Average of Observation | 21.7% | 22.88% |
Note: In this study, students were chosen at random from a small pool of samples. As a result, although not all Afghan students or members of society suffer from dental malocclusion, the survey's findings do show that it is common among dentistry students at Kabul University of Medical Science.
Conclusion
The following conclusions were drawn from the present survey:
- Angle’s class I malocclusion was 48.3% in males and 53.8% in females. Class II was 6.6% in males and 21.5% in females and class III was 43.3% in males and 23% in females.
- Class I of malocclusion was more standard in females than males, while class III of malocclusion was more common in males than females.
- Crowding had the highest speed among participants followed by a deep bite, open bite, and edge-to-edge bite.
- The occurrence of dental trauma in boys and heredity in girls may be the most important factors for dental malocclusion.
- Girls were more interested in orthodontic treatments, because they pay more attention to beauty than boys.
Recommendations
- According to our survey of Kabul University of Medical Science's dentistry faculty students, all of the respondents were dental students who had adequate knowledge and information about the issues posed by dental abnormalities and irregularities. As a result, all of the respondents paid close attention to their oral health, particularly dental irregularities. Thus, it seems sense that knowledge and information about a problem are required in order to address or lessen it. As a result, we urge the Afghan government to eliminate dental anomalies in society by providing adequate information about them and increasing community awareness. To raise awareness of oral health, particularly dental malocclusion, the public should be educated through the media, academic conferences held in schools and universities, and the press.
- Girls were more interested than boys in addressing dental malocclusion, according to our research, and it is also evident that dental therapies and specialized orthodontics treatments are frequently pricey, making the majority of people unable to afford the treatment. As a result, we implore and urge the government to provide greater facilities for women, both financially and in terms of simple access to treatment, especially orthodontists who should give more discounts for women's orthodontic care. By doing so, we may both raise public awareness of the need to treat dental problems and slow their spread across society.
- Due to the paucity of study on dental malocclusion in Afghanistan, it is unable to fully and in-depth assess the underlying issues of the population. So, in order to develop and propose efficient treatments and programs to resolve or lessen malocclusion issues, we need more research on more individuals throughout all provinces. Thus, we urge our government to give researchers additional opportunities to conduct such inquiries.
Author contributions
Ehsan H. contributed to the conception of the study, its administration and collection of the questionnaires, interpretation of the findings, creation of the master table of findings, and writing and data analysis of the paper; Azami, M. contributed to the research's concept, the creation of the master results table, the results' interpretation, and the drafting and revision of the report; Azimi, S. contributed to the conception of the study, the analysis of the findings, and the revision of the publication. All authors agreed to be responsible for every part of the work and granted their final permission.
References
- Marques LS, Porteus IA, Ramos-Jorge ML, Filogônio CA, Filogônio CB. et al. (2009). Factors associated with the desire for orthodontic treatment among Brazilian adolescents and their parents. BMC Oral Health, 9:34.
Publisher | Google Scholor - Tak M, Nagarajappa R, Sharda AJ, Asawa K, Tak A. et al. (2013). Prevalence of malocclusion and orthodontic treatment needs among 12–15 years old school children of Udaipur, India. Eur J Dent. 7(1): S45-S53.
Publisher | Google Scholor - Gupta DK, Singh SP, Utreja A, Verma S. (2016). Prevalence of malocclusion and assessment of treatment needs in β-thalassemia major children. Prog Orthod, 17(1):7.
Publisher | Google Scholor - Ahangar-Atashi MH, Dabaghi-Tabriz F, S, Rahbar M. (2017). Prevalence of Dental Malocclusions in Patients admitted to the Department of Orthodontics, School of Dentistry, Tabriz, in. J Contemp Dent Pract, 18(11):1034-1039.
Publisher | Google Scholor - Staley, N. (2001). Etiology and prevalence of malocclusion. In: Bishara SE, editor. Textbook of orthodontics. Philadelphia (PA): W.B Saunders Company, 84-104.
Publisher | Google Scholor - Guo L, Feng Y, Guo HG, Liu BW, Zhang Y. (2016). Consequences of orthodontic treatment in malocclusion patients clinical and microbial effects in adults and children. BMC Oral Health, 16(1):112-112.
Publisher | Google Scholor - Dimberg L, Lennartsson B, Arnrup K, Bondemark L. (2015). Prevalence and change of malocclusions from primary to early permanent dentition: A longitudinal study. Angle Orthod, 85:728-734.
Publisher | Google Scholor - Peres KG, Barros AJ, Peres MA, Victora CG. (2007). Effects of breastfeeding and sucking habits on malocclusion in a birth cohort study. Rev Saude Publica, 41:343-350.
Publisher | Google Scholor - Heimer MV, Tornisiello Katz CR, Rosenblatt A. (2008). Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: A longitudinal study. Eur J Orthod, 30:580-585.
Publisher | Google Scholor - Grewe JM, Cervenka J, Shapiro BL, Witkop CJ., Jr. (1968). Prevalence of malocclusion in Chippewa Indian children. J Dent Res,47:302-305.
Publisher | Google Scholor - Mills LF. (1966). Epidemiologic studies of occlusion. IV. The prevalence of malocclusion in a population of 1,455 school children. J Dent Res, 45:332-336.
Publisher | Google Scholor - Proffit WR, Fields HW, Jr, Moray LJ. (1998). Prevalence of malocclusion and orthodontic treatment need in the United States: Estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg, 13:97-106.
Publisher | Google Scholor - Helm S. (1968). Malocclusion in Danish children with adolescent dentition: An epidemiologic study. Am J Orthod, 54:352-366.
Publisher | Google Scholor - Lew KK, Foong WC, Loh E. (1993). Malocclusion prevalence in an ethnic Chinese population. Aust Dent J, 38:442-449.
Publisher | Google Scholor - Alexander S, Hegde S, Sudha P. (1997). Prevalence of malocclusion and periodontal status in Tibetan school children of Kushalnagar, Mysore district. J Indian Soc Pedod Prev Dent, 15:114-117.
Publisher | Google Scholor - Siddegowda R, Satish RM. (2014). The prevalence of malocclusion and its gender distribution among Indian school children: An epidemiological survey. SRM J Res Dent Sci, 5:224-229
Publisher | Google Scholor - Abhishek, Goyal M. (2019). Prevalence of Malocclusion in Rural and Backward Area (Seemanchal) in Bihar-India. Ann. Int. Med. Den. Res, 5(4): DE34-DE39.
Publisher | Google Scholor - Gul-e-Erum, Fida, M. (2008). Pattern of malocclusion in orthodontic patients: a hospital-based study. Journal of Ayub Medical College, 20(1), 43-47.
Publisher | Google Scholor - (2014). PREVALENCE OF ANGLES MALOCCLUSION ACCORDING to TOAGE GROUPS AND GENDER. Pakistan Oral & Dental Journal.
Publisher | Google Scholor - (2016). Orthodontic Treatment of Malocclusion and its Impact on Oral Health-Related Quality of Life. The Open Dentistry Journal, 10:236 -241.
Publisher | Google Scholor - Clark J, Evans R. (2001). Functional occlusion: I. A review. Journal of Orthodontics, 28: 76-81.
Publisher | Google Scholor - Davies S, Gray R. (2001). Occlusion: What is occlusion? British dental journal, 191: 235-45.
Publisher | Google Scholor - Mohlin B, al-Saadi E, Andrup L, Ekblom K. (2002). Orthodontics in 12-year old children. Demand, treatment motivating factors, and treatment decisions. Swed Dent J, 26(2): 89-98.
Publisher | Google Scholor - Perillo L, Esposito M, Contiello M, Lucchese A, Santini AC, et al. (2013). Occlusal traits in developmental dyslexia: a preliminary study. Neuropsychiatr Dis Treat, 9: 1231-1237.
Publisher | Google Scholor - Liu Z, McGrath C, Hägg U. (2009). The impact of malocclusion/orthodontic treatment need on the quality of life. A systematic review. Angle Orthod, 79(3): 585-591.
Publisher | Google Scholor - Siddegowda R, Satish R. (2014). The prevalence of malocclusion and its gender distribution among Indian school children: an epidemiological survey. SRM Journal of Research in Dental Sciences, 5(04):224-229.
Publisher | Google Scholor - (2004). National Oral Health Survey and Fluoride Mapping. Dental Council of India New Delhi.
Publisher | Google Scholor - Aikins EA, Onyeaso CO. (2014). Prevalence of malocclusion and occlusal traits among adolescents and young adults in Rivers state, Nigeria. Odontostomatol Trop, 37:5-12.
Publisher | Google Scholor - Ahmed G. (2015). [Thesis] Medical and Health Studies Board, Graduate College, University Khartoum. Prevalence of Malocclusion in University of Khartoum Students.
Publisher | Google Scholor - Bugaighis I, Karanth D. (2013). The prevalence of malocclusion in urban Libyan schoolchildren. J Orthod Sci, 2:1-6.
Publisher | Google Scholor - Laganà G, Masucci C, Fabi F, Bollero P, Cozza P. (2013). Prevalence of malocclusions, oral habits and orthodontic treatment need in a 7- to 15-year-old schoolchildren population in Tirana. Prog Orthod, 14:12.
Publisher | Google Scholor - Kasparaviciene K, Sidlauskas A, Zasciurinskiene E, Vasiliauskas A, Juodzbalys G, et al. (2014). The prevalence of malocclusion and oral habits among 5-7-year-old children. Med Sci Monit, 20:2036-2042.
Publisher | Google Scholor - Singh VP, Sharma A. (2014). Epidemiology of malocclusion and assessment of orthodontic treatment need for Nepalese children. Int Sch Res Notices, 1-4.
Publisher | Google Scholor - Siddegowda R, Satish R. (2014). The prevalence of malocclusion and its gender distribution among Indian school children: An epidemiological survey. SRM J Res Dent Sci. 5:224-229.
Publisher | Google Scholor - Alatrach AB, Saleh FK, Osman E. (2001). The prevalence of malocclusion and orthodontic treatment need in a sample of Syrian children. Eur J Orthod, 10:153-167.
Publisher | Google Scholor - Nazir R, Hussain A, Kaleem M. (2012). Oral health status and malocclusion in flood-affected and internally displaced children in Pakistan. Pak Oral Dent J, 32:110-114.
Publisher | Google Scholor - Celikoglu M, Akpinar S, Yavuz I. (2010). The pattern of malocclusion in a sample of orthodontic patients from Turkey. Med Oral Patol Oral Cir Bucal, 15:e791-796.
Publisher | Google Scholor - Dua R, Sharma S. (2012). Prevalence, causes, and correlates of traumatic dental injuries among seven-to-twelve-year-old school children in Dera Bassi. Contemp Clin Dent, 3:38-41.
Publisher | Google Scholor - Sharma, Ruchi, et al. (2015).
Publisher | Google Scholor













