

Research article
Prevalence and Associated Factors of Forgone Care Among Hypertensive Patients in Selected Public Hospitals in Addis Ababa, Ethiopia: Cross-Sectional Study
1Department of Internal Medicine, Ras Desta Damtew Memorial Hospital, Addis Ababa, Ethiopia.
2Gandi Memorial Hospital, Addis Ababa, Ethiopia.
3Redat Healthcare, Addis Ababa, Ethiopia.
*Corresponding Author: Kirubel Workiye Gebretsadik, Department of Internal Medicine, Ras Desta Damtew Memorial Hospital, Addis Ababa, Ethiopia.
Citation: Kirubel W. Gebretsadik, Feruza M. Suleyiman, Biruktawit D. Enkoye. (2024). Prevalence and Associated Factors of Forgone Care Among Hypertensive Patients in Selected Public Hospitals in Addis Ababa, Ethiopia: Cross-Sectional Study, Pollution and Community Health Effects, BioRes Scientia Publishers. 2(1):1-8. DOI: 10.59657/2993-5776.brs.24.017
Copyright: © 2024 Kirubel Workiye Gebretsadik, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 15, 2024 | Accepted: March 02, 2024 | Published: March 09, 2024
Abstract
Background: Hypertension is a complex chronic disease requiring appropriate continuous medical care, and forgone care may exacerbate the severity of the disease and associated complications. The assessment of forgone care indicates the gap between perceived need and actual utilization of healthcare services. This study aimed to investigate the prevalence and associated factors affecting forgone care in patients with hypertension.
Method:A cross-sectional study was also conducted. Study subjects were selected by using a systematic sampling technique. The data were collected using an interview-administered written questionnaire. A descriptive analysis was conducted to obtain a summary value for each variable. All variables with a p value < 0.25 in the bivariate analysis were entered into a multivariable logistic regression model to identify factors that were significantly associated with the outcome variable. A p value < 0.05 indicated statistical significance. The data are presented in statements, tables, and graphs.
Results:A total of 405 patients were included in the study. Of these, 35.2% reported forgone care. The most frequently stated reason for forgoing care was the financial burden resulting from the costs of disease treatment (46.3%). According to the final multivariable regression model, the odds of receiving care among hypertensive patients who did not have community-based health insurance were 2.754 times greater than those among those who did. The odds of receiving care among hypertensive patients who did not have family support were 2.31 times greater than those among patients who had family support.
Conclusion and recommendation: A considerable number of patients with hypertension had a history of forgoing care, and the most important reasons for forgoing care were related to financial pressure and lack of family support for receiving treatment. A qualitative study is needed to further investigate the underlying reasons why hypertensive patients forgo healthcare.
Keywords: hypertension; forgone care; treatment withdrawal; relinquished care
Introduction
Forgone treatment was defined as the frequency with which a person self-reported skipping out of medical care while they were ill and in need of it in the year before the survey day [1]. A person who forgone medical care does not use medical services even when they believe they are necessary [2]. Forgoing care is a significant factor in evaluating the effectiveness of the healthcare system because it highlights a discrepancy between the public's perception of their need for care and their actual utilization. A lack of care can have a variety of negative effects, such as the advancement of an illness, increased usage of emergency rooms, "worrying," and/or difficulties going about daily tasks [2,3]. People who reported forgoing care can be categorized into two groups: group (I), people who believe they need healthcare and that a professional would confirm that need (both subjective and objective need); and group (II), people who believe they need healthcare but that a professional would not confirm that need (subjective but not objective need). Both types of forgone care are highly relevant for the individuals, health care providers, and, eventually, the health care system. Reported forgone care points to impediments to healthcare utilization [2]. According to a recent World Health Organization (WHO) report, the cost of healthcare has thrown approximately 100 million people worldwide into "severe poverty." Many people around the world must make difficult decisions to forgo necessary medical care due to cost, which is especially difficult for those who live in low- to middle-income nations where the proportion of out-of-pocket spending can be significant [4].
Research on forgone care among patients with CVD has been carried out mainly in Europe, the USA, and Canada. Research from Africa is largely unavailable. Previous research has associated delayed and forgone medical care with lower health outcomes and more expensive medical care, particularly in the older population[5]. Despite being one of the most modifiable risk factors for cardiovascular illnesses, the prevention and treatment of hypertension have not received the attention of many poor nations [6]. Because HIV/AIDS, tuberculosis, and malaria are given top priority in these nations, there is a severe lack of awareness, treatment, and control of hypertension[7]. According to the 2019 WHO Africa report, in Ethiopia, where CVD was by far the most common NCD-related cause of death, hypertension was one of the main risk factors. In this report, 15.9% of people in the population had hypertension; however, just 1.5% of them had hypertension under control, and 2.8% received necessary care [8]. Therefore, it is very important to understand the prevalence of forgone care and associated factors for public health programs and intervention designs among hypertensive patients in the Ethiopian context. The government of Ethiopia is concentrating its efforts on establishing universal health care. To achieve universal health coverage, it is essential to try to recognize and remove obstacles that prevent people from receiving the medical care they require. Less attention has been given to comprehending issues related to forgoing health needs. Forgone care is an important component of unmet health needs; it delays and lowers quality care and involves an individual not using health care despite the need for it. Therefore, this study aimed to assess the prevalence and associated factors of forgone care in hypertensive patients in Addis Ababa, Ethiopia. This research will identify the most common reasons for forgone care.
Methods
Study area and period
The study was conducted from May 22 to June 22, 2023, at selected public hospitals (namely, Yekatit 12 Hospital Medical College, Ras Desta Damtew Memorial Hospital, and MenelikII Comprehensive Specialized Hospital) in Addis Ababa, Ethiopia.
Study Design
A cross-sectional study was conducted on hypertensive patients in selected public hospitals in 2023.
Source and Study Population: The source population was all hypertensive patients in selected public hospitals in Addis Ababa during the study period.
The study population included hypertensive patients who met the eligibility criteria at selected public hospitals in Addis Ababa during the study period.
Study unit: patients
Inclusion criteria
All hypertensive patients aged >18 years were admitted to the hospital outpatient department and emergency department.
Exclusion criteria
Seriously ill hypertensive patients and hypertensive patients with a major psychiatric problem, which was recorded on the patient chart, were excluded from the study.
Sampling Procedure
First, a list of public hospitals in Addis Ababa was identified, and three public hospitals were included randomly in the study (1 teaching hospital, 1 specialized hospital, and 1 general hospital). Second, study participants who were diagnosed with hypertension were identified by using inclusion and exclusion criteria. Based on the total number of hypertensive patients available in each hospital during the study period, the sample size of the study was allocated to those hospitals proportional to the number of hypertensive patients. Using the sampling frame, systematic random sampling was used to select and enroll study participants. From the sampling frame, the first sample was selected randomly, and then, every 3rd patient from a selected sample that fulfilled the inclusion criteria was recruited until the sample size was fulfilled for each hospital.
Data Collection Methods
Data collection instruments and procedure
A structured questionnaire was used to examine the factors affecting foregone care. The data were collected using structured and pretested questionnaires developed based on the relevant literature and modified to match the aims of this study. The appropriateness and applicability of the measures and tools were evaluated by pretest and face validity. The English version of the questionnaire was prepared and translated to Amharic and then back-translated to English to confirm the appropriateness of the translation. All the questionnaires were subsequently subjected to a face-to-face interview to validate the accuracy of the responses. The questionnaire consists of three parts: sociodemographic and social network variables (gender, age, marital status, income status, education status, employment status, household side, village proximity to the hospital), disease-related variables (chronicity in years of hypertension, presence of comorbidity or complications, history of hospitalization due to complications of hypertension during the last year and awareness about hypertension) and items related to reasons for forgoing care (cost, waiting time, community health insurance).
Data quality control
Pretesting was performed on 20 randomly selected patients who fulfilled the inclusion criteria during the specified study period before full-scale data collection. Based on the pretest results, the questionnaire was additionally adjusted and administered to the whole sample. All the data collectors and supervisors were trained by the principal researcher. To improve the data quality, double data entry and data cleaning were performed by checking for inconsistent numerical errors and missing parameters. Once the data were completely clean, the data were exported to SPSS version 25.0 software for analysis.
Operational definition
Forgone care: Forgone health care is defined as not using health care despite perceiving a need for it[9]. Hypertension: Hypertension (high blood pressure) occurs when the pressure in a patient’s blood vessels is too high (140/90 mmHg or higher). It is common but can be severe if not treated [10]. Monthly income: A person working in Ethiopia typically earns approximately 8,930 ETB. Salaries range from 2,250 ETB (lowest average) to 39,700 ETB (highest average, actual maximum salary is higher) [11].
Data processing and analysis
Descriptive statistics were used to calculate the frequency distribution and proportions for categorical variables. Numerical variables were summarized using the mean (± standard deviation) or median (interquartile range) after testing the normality of the variables using the Kolmogorov‒Smirnov test, where a p value >0.05 indicated a normal distribution. A bivariate logistic regression model was used to assess the factors associated with forgone care among hypertensive patients. Variables with a p value <0 xss=removed xss=removed>
Results
Sociodemographic characteristics
From the 423 samples, information was collected from 405 hypertensive patients, for a response rate of 95.7 percentage. The average age of the patients was 57 (SD ±12) years. Most of the hypertensive patients were married (250 [61.2 percentage]) or female (227 [55.8 percentage]). More than a quarter of the patients did not attend formal school (112 [27.2 percentage]) and were in less than 5 km proximity to the hospitals (165 [39.5 percentage]) and workers (229 [56.3 percentage]). Most of the hypertensive patients had a 4-6 family size (207 [49.6 percentage]), as shown in Table 1.
Table 1: Sociodemographic and health system characteristics of the study population seen at selected public hospitals in Addis Ababa, 2023. (n=405)
| Variable category | frequency | Percent | |
| Sociodemography factors | |||
| sex | male | 178 | 44.2 |
| female | 227 | 55.8 | |
| Age category | <50> | 120 | 29.6 |
| 50-59 | 125 | 28.6 | |
| 60-69 | 106 | 26.5 | |
| >=70 | 54 | 15.4 | |
| Marital status | single | 34 | 9.5 |
| married | 253 | 61.2 | |
| widowed | 79 | 20.1 | |
| divorced | 39 | 9.2 | |
| education | No formal education | 111 | 27.2 |
| primary | 98 | 24.1 | |
| secondary | 77 | 19.1 | |
| vocational | 60 | 14.9 | |
| College/university | 59 | 14.7 | |
| Habitant distance in KM | <5> | 161 | 39.5 |
| 5-9 | 148 | 36.4 | |
| >=10 | 96 | 24.1 | |
| Family size | 1-3 | 153 | 37.6 |
| 4-6 | 204 | 49.6 | |
| >=7 | 48 | 12.8 | |
| employment | Not worker | 176 | 43.7 |
| worker | 229 | 56.3 | |
| CBHI | Yes | 235 | 57.7 |
| No | 170 | 42.3 | |
| Support from family | Yes | 276 | 67.4 |
| No | 129 | 32.6 | |
Disease-related profile
The majority of the patients were diagnosed with hypertension within 5 years (210 [50.6 percentage]), followed by 5-9 years (119 [29.1 percentage]). The majority of these patients used hypertensive medications (389 [93.6 percentage]) or more than 1 medication (193 [47.3%]). Approximately half of the patients had a comorbidity (186 [45.4 percentage]), 81 [19.1 percentage] had reported hypertensive complications, and 51 [12.8%] were hospitalized during the last year due to hypertension complications. As shown in Table 2.
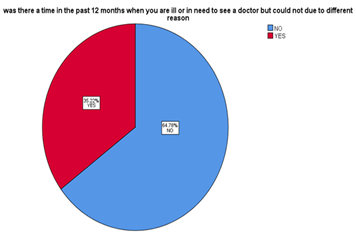
Table 2: Common reasons for, symptoms of, and treatment options for hypertensive patients who forgone care at selected public hospitals in Addis Ababa, 2023. (n=405)
| Variable category | Frequency | Percentage | |
| Common reasons to forgone care | Long Waiting time and long process of treatment | 45 | 32.2% |
| The financial burden due to the cost of treatment | 65 | 46.3% | |
| Long distances from the health care centers | 26 | 18.8% | |
| Inappropriate behavior of health care providers (discriminatory behavior, and disrespectful behavior) | 2 | 1.3% | |
| Major symptom or reason encountered while forgone care | Follow-up | 62 | 43% |
| Headache | 47 | 32.9% | |
| Chest pain | 5 | 4.7% | |
| Other (myalgia, leg swelling, numbness…) | 26 | 19.5% | |
| The alternative solution used for forgone care | Missed follow-up | 63 | 43.6% |
| Herbal medication | 15 | 11.4% | |
| Buy anti-pain from pharmacy | 46 | 32.2% | |
| Other (does nothing, sleep…) | 17 | 12.8% |
Factors associated with forgone care
The results of the binary logistic regression model are shown in Table 3. Univariate binary logistic regression was run at a 25% level of significance to select variables to be included in the final multivariable binary logistic regression model, and the following variables were found to be significant: age category, sex, family size, living area category, employment status, income, number of medications, method used for hypertension control, community-based health insurance and family support. The final multivariable binary logistic regression model showed that community-based health insurance, habitant distance, income, and family support were significantly associated with forgone care among hypertensive patients at the 5 percentage level of significance. Accordingly, after adjusting for other covariates included in the final regression model, the odds of forgone care among hypertensive patients who did not have community-based health insurance were 2.754 times greater than those among patients who had community-based health insurance (AOR= 2.754, 95 percentage CI= 1.610, 4.710; p value=0.000). The odds of receiving care for hypertensive patients who did not have family support were 2.31 times greater than those who had family support (AOR= 2.310, 95 percentage CI= 1.237, 4.315; p value=0.009). In addition, the odds of reporting forgone care were 61.8 percentage lower for patients who lived within a five-kilometer distance from the hospital and 47.2 percentage lower for patients who lived within five-to-nine-kilometer distances. AOR=0.382, 95 percentage CI= 0.209, 0.699, p value=0.002; and AOR=0.528, 95 percentage CI= 0.294, 1.266, p value=0.033. The odds of reporting forgone care were 74.4 percentage lower for patients whose monthly income was less than 2250 birr (AOR= 0.256, 95 percentage CI= 0.067, 0.097, p value=0.046).
Table 3: Factors associated with forgone care among hypertensive patients in Addis Ababa, 2023. (n=405)
| variable | Forgone care | COR at 95% CI | AOR at 95%CI | P value | ||
| Yes | No | |||||
| Community-based health insurance | Yes | 54(40.3%) | 180(67.2%) | 1 | 1 | |
| No | 85(59.7%) | 86(32.8%) | 3.033(2.006,4.584) | 2.754 (1.610, 4.710) | 0.000* | |
| Age category | <50> | 53(36.9%) | 68(25.5%) | 1.646(0.878,3.086) | 1.742 (0.613, 4.954) | 0.298 |
| 50-59 | 37(26.2%) | 83(29.9%) | 0.997(0.523,1.899) | 1.601 (0.581, 4.409) | 0.363 | |
| 60-69 | 31(22.8) | 75(28.5%) | 0.913(0.473,1.763) | 0.951 (0.442, 2.045) | 0.897 | |
| >70 | 18(14.1%) | 40(16.1%) | 1 | 1 | ||
| Family size | 1-3 | 64(45%) | 89(33.6%) | 0.93 (0.215, 4.113) | 0.881 (0.178, 4.368) | 0.877 |
| 4-6 | 65(45.6%) | 139(51.8%) | 2.052(0.963,4.373) | 1.039 (0.424, 2.544) | 0.933 | |
| >6 | 11(9.4%) | 37(14.6%) | 1.350(0.640,2.846) | 0.940 (0.400, 2.209) | 0.888 | |
| Income category in birr | <2250> | 24(18.1%) | 87(32.8%) | 0.263(0.087,0.790) | 0.256 (0.067, 0.977) | 0.046* |
| 2251- 8900 | 110(76.5%) | 173(64.6%) | 0.564(0.199,1.597) | 0.491 (0.145, 1.664) | 0.253 | |
| >8900 | 5(5.4%) | 6(2.6%) | 1 | 1 | ||
| Sex | Male | 74(52.3%) | 104(39.8%) | 0.601(0.402,0.899) | 0.726 (0.440, 1.199) | 0.211 |
| Female | 67(47.7%) | 160(60.2%) | 1 | 1 | ||
Support from family | Yes | 34(25.5%) | 242(90.1%) | 1 | 1 | |
| No | 106(74.5%) | 23(9.9%) | 3.132(1.822,5.384) | 2.310 (1.237, 4.315) | 0.009* | |
| Number of HTN medication | 0 | 4(2.7%) | 21(7.7%) | 1 | 1 | |
| 1 | 60(43.6%) | 130(48.5%) | 0.286(0.095,0.864) | 0.237 (0.010, 5.731) | 0.375 | |
| >=2 | 75(53.7%) | 115(43.8%) | 0.733(0.487,1.105) | 0.699 (0.422, 1.157) | 0.164 | |
| Method, do you use for hypertension control | Lifestyle only | 5(3.4%) | 22(8%) | 0.398(0.147,1.073) | 1.103(0.058,21.010) | 0.948 |
| medication | 135(96.6%) | 243(92%) | 1 | 1 | ||
| Employment status reorganized | Not worker | 54(38.9%) | 122(46.4%) | 0.738(0.492,1.107) | 1.896(0.865,4.158) | 0.110 |
| Worker | 87(61.1%) | 139(53.6%) | 1 | 1 | ||
Note: COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval; *statistically significant
Discussion
This study aimed to assess the prevalence of forgone care and identify the factors affecting forgone care among patients with hypertension. According to our results, 35.2% of the patients reported forgone care. This result is comparable with those of other studies performed in Kenya, Ghana, and Indonesia [12-14]. However, this number is greater than that reported in other studies performed in China, Europe, and the USA[2,5,15,16]. Given that hypertension and other chronic diseases require long-term care and that the consequences of their treatment are not immediate or short-term, in many cases, the patient cannot make a reasonable association between forgoing treatment and its outcomes. Given the implementation of the Ethiopian Noncommunicable Disease Prevention and Control Program, it can be concluded that the percentage of patients with hypertension receiving forgone care is high, which is indicative of the poor performance of the healthcare system in treating CVD.
In this study, the odds of receiving care among hypertensive patients who did not have community-based health insurance were 2.754 times greater than those among patients who had community-based health insurance. These results are in line with those of other studies performed in Kenya, Ghana, Germany, China, and the USA [2,17-20]. Since most patients were elderly individuals with low socioeconomic status and only a small percentage of patients were covered by supplementary insurance, the disease treatment cost was reported as the leading cause of forgone care. For people who were not covered by health insurance, financial barriers to access had a greater impact on their treatment withdrawal. Hypertension imposes a considerable cost on patients, especially lower-income patients. Therefore, to reduce the rate of withdrawal from treatment, it is necessary to provide financial support, such as strengthening community-based health insurance coverage for low-income people to improve their financial access to healthcare services. In the study of L.A. Adebusoye et al. among hypertensive patients, the proportion of hypertensive patients with strong perceived family support was 93.3%, which is in line with our study [21]. In our study, forgone care was more likely to be provided to patients with no family support or no community-based health insurance during the last year.
Limitations
Some limitations of the study must be acknowledged. The study evaluated foregone care only among hypertensive patients who perceived a need for healthcare but did not seek treatment; however, it did not take into account those with other cardiovascular diseases. The study was performed in selected public hospitals in Addis Ababa; it did not include private hospitals or health centers. Therefore, the prevalence of foregone care may have been underestimated to some extent. In addition, cross-sectional data cannot be used to draw causal conclusions about why these individuals may have foregone care.
Conclusion
The results showed that despite the implementation of the prevention and control program for noncommunicable diseases, a considerable number of patients with hypertension had a history of forgoing care in selected public hospitals in Addis Ababa, and the most important reasons for forgoing care were related to financial barriers and long waiting times. The findings indicate that individuals without adequate health insurance coverage are more likely to experience barriers to accessing healthcare, leading to a greater likelihood of forgone care. Additionally, longer waiting times to receive treatment contribute to the decision to forgo care, as patients may opt to delay or avoid treatment due to time constraints or worsening symptoms. Finally, the presence of family support serves as a protective factor, as individuals with strong support are more likely to seek timely care.
Abbreviations
AARHB…………Addis Ababa Regional Health Bureau
BP ………………. Blood pressure
CVD ……………Cardio vascular disease
EMOH ………… Ethiopian Ministry of Health
MCH………………Maternal and Child Health
NCD………………Non-Communicable Disease
SDG………………Sustainable Development Goal
WHO……………World Health Organization
Declarations
Ethical considerations
Ethical clearance was obtained from the Addis Ababa Public Health Research and Emergency Management Directorate. Permission letters were obtained from the Addis Ababa City Administration Health Bureau Institutional Review Board. All the study participants were reassured/informed that they would be anonymous. Access to the collected information was limited to the investigators, and confidentiality was maintained throughout the project.
Availability of data and materials
All relevant data are available upon reasonable request.
Competing interests
The authors declare that they have no known competing interests.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Contribution
K.W. contributed to the study conception, designed the study, performed the statistical analysis, and drafted the manuscript. B.D. and F.M. assisted in the statistical analysis and drafting of the manuscript. All the authors revised and approved the final manuscript. K.W. contributed to the conception and proposal and writing of the research.
Acknowledgments
The authors would like to thank all individuals involved in the facilitation of this research.
References
- Jalilian H, Heydari S, Mir N, Fehresti S, Khodayari-Zarnaq R. (2021). Forgone care in patients with type 2 diabetes: a cross-sectional study. BMC Public Health, 21(1):1588.
Publisher | Google Scholor - Röttger J, Blümel M, Köppen J, Busse R. (2016). Forgone care among chronically ill patients in Germany—Results from a cross-sectional survey with 15,565 individuals. Health Policy, 120(2):170-178.
Publisher | Google Scholor - Anderson KE, McGinty EE, Presskreischer R, Barry CL. (2023). Reports of Forgone Medical Care Among US Adults During the Initial Phase of the COVID-19 Pandemic. JAMA Netw Open, 4(1):2034882.
Publisher | Google Scholor - (2023). Global Health Expenditure Database.
Publisher | Google Scholor - Li X, Chen M, Wang Z, Si L. (2018). Forgone care among middle aged and elderly with chronic diseases in China: evidence from the China Health and Retirement Longitudinal Study Baseline Survey. BMJ Open, 8(3):019901.
Publisher | Google Scholor - (2018). WHO. Noncommunicable diseases (NCD) country profiles. Risk of premature death due to NCDS in Ethiopia.
Publisher | Google Scholor - Geldsetzer P, Manne-Goehler J, Marcus ME, Ebert C, Zhumadilov Z et al. (2022). The state of hypertension care in 44 low-income and middle-income countries: a cross-sectional study of nationally representative individual-level data from 1·1 million adults. The Lancet, 394(10199):652-662.
Publisher | Google Scholor - Guwatudde D, Nankya-Mutyoba J, Kalyesubula R, Laurence C, Adebamowo C. et al. (2015). The burden of hypertension in sub-Saharan Africa: a four-country cross sectional study. BMC Public Health, 5(15):1211.
Publisher | Google Scholor - Tsuzaki K, Taira D. (2023). Forgone Health Care for Non–COVID-19–Related Needs Among Medicare Beneficiaries During the COVID-19 Pandemic, Summer 2020–Winter 2021. Prev Chronic Dis, 6(19):220110
Publisher | Google Scholor - (2021). WHO.
Publisher | Google Scholor - (2023). Average Salary in Ethiopia 2023 - The Complete Guide.
Publisher | Google Scholor - Ainy A, Idris H, Maharani A. (2020). Unmet Need for Healthcare Among People with Hypertension in Indonesia.
Publisher | Google Scholor - Kuria N, Reid A, Owiti P, Tweya H, Kibet CK. (2018). et al. Compliance with follow-up and adherence to medication in hypertensive patients in an urban informal settlement in Kenya: comparison of three models of care. Trop Med Int Health, 23(7):785-794.
Publisher | Google Scholor - Adler AJ, Laar A, Prieto-Merino D, Der RMM, Mangortey D.et al. (2019). Can a nurse-led community-based model of hypertension care improve hypertension control in Ghana? Results from the ComHIP cohort study. BMJ Open, 9(4):026799.
Publisher | Google Scholor - Lucevic A, Péntek M, Kringos D, Klazinga N, Gulácsi L. et al. (2019). Unmet medical needs in ambulatory care in Hungary: forgone visits and medications from a representative population survey. Eur J Health Econ, 20(1):71-78.
Publisher | Google Scholor - Thomas A, Valero-Elizondo J, Khera R, Warraich HJ, Reinhardt SW. et al. (2021). Forgone Medical Care Associated with Increased Health Care Costs Among the U.S. Heart Failure Population. JACC Heart Fail, 9(10):710-719.
Publisher | Google Scholor - Bonfrer I, Gustafsson-Wright E. (2017). Health shocks, coping strategies and foregone healthcare among agricultural households in Kenya. Glob Public Health, 12(11):1369-1390.
Publisher | Google Scholor - Bodenmann P, Favrat B, Wolff H, Guessous I, Panese F. et al. (2014). Screening Primary-Care Patients Forgoing Health Care for Economic Reasons. PLoS ONE, 9(4):94006.
Publisher | Google Scholor - Werner P, Tur-Sinai A. (2021). Prevalence and correlates of forgone care among adult Israeli Jews: A survey conducted during the COVID-19 outbreak. PloS One, 16(11):0260399.
Publisher | Google Scholor - (2023). Forgone Health and Economic Benefits Associated with Socioeconomic Differences in Organized Cervical Cancer Screening – PMC.
Publisher | Google Scholor - Ilori HT, Adebusoye LA, Daramola OO, Ajetunmobi OA. (2020). Perceived family support and its effect on cardiovascular disease risk among hypertensive patients presenting at a family medicine practice in south west Nigeria. Niger J Fam Pract, 11(2):19-26.
Publisher | Google Scholor













