

Research Article
Predictors of Time-to-Death Among Under-Five Children in Benishangul-Gumuz Regional State, Ethiopia: A Cross-Sectional Study
Department of Statistics, College of Natural and Computational Science, Adigrat University, Adigrat, Ethiopia.
*Corresponding Author: Gebru Gebremeskel Gebrerufael, Department of Statistics, College of Natural and Computational Science, Adigrat University, Adigrat, Ethiopia.
Citation: Gebru G. Gebrerufael. (2023). Predictors of Time-to-Death Among Under-Five Children in Benishangul-Gumuz Regional State, Ethiopia: A Cross-Sectional Study. Journal of BioMed Research and Reports, BRS Publishers. 2(2); DOI: 10.59657/2837-4681.brs.23.017
Copyright: © 2023 Gebru Gebremeskel Gebrerufael, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 30, 2023 | Accepted: April 14, 2023 | Published: April 21, 2023
Abstract
Background: Although Ethiopia attained the fourth-millennium development goal, it promised to decrease the under-five children's death rate in 2015. However, the under-five children death rate has still remained a major public health problem in the Benishangul-Gumuz Regional State at the country level. Therefore, this study aimed to assess the predictor factors associated with the under-five children death rate in the Benishangul-Gumuz Regional State.
Methods: A community-based retrospective cross-sectional study design was used. The information gathered from 906 children born five years preceding the survey was measured. Variables such as maternal and child demographic characteristics, health, and environmental factors were measured as predictor factors of under-five children's death rate. The study used descriptive statistics, and Cox Proportional-hazard (PH) regression model to identify the major significant predictor factors associated with under-five children's death rate.
Results: The overall prevalence of experiencing under-five children death rate was 9.3% [95%CI: 0.0738, 0.112] in the Benishangul-Gumuz Regional State. The Cox PH regression model analysis revealed, being multiple births (AHR = 2.17; 95% CI (1.17–4.20)), using unprotected well water (AHR = 2.13; 95% CI (1.32–3.42)), parity between 6–8 (AHR = 3.16; 95% CI (1.40–7.16)) and 9 and above (AHR = 7.86; 95% CI (2.23–27.72)), the agricultural sector of mother’s occupation (AHR = 0.39; 95% CI (0.20–0.76)) and family size (AHR = 0.74; 95% CI (0.60–0.93)) were significantly associated with a higher risk of under-five children death rate. An increment in family size and parity increases the risk of under-five children's death rate.
Conclusions: The study identified the source of drinking water, family size, parity, mother’s occupation and type of childbirth were the predictor factors significantly associated with under-five children death. The prevalence of under-five children death rate shows that Benishangul-Gumuz Regional State was experiencing a higher death rate than the national level. Therefore, both government policymakers and other concerned organizations should be given special attention to the major predictor factors of the under-five children's death rate and do greater emphasis on decreasing under-five children's death rate, and health intervention policies must be studied.
Keywords: under-five children death; benishangul-gumuz; cox PH model
Introduction
The under-five child death is defined as the probability of dying a child between birth and the fifth birthday [1]. Although there is a global reduction in under-five death, from 5.9 million deaths in 2015 to 5.3 million in 2018, still there is a high death rate in low and middle-income African countries (81/1000 total live births) including Ethiopia, which is approximately 7 times higher than in the European countries [1, 2].
In Ethiopia, under-five child death still remains the major and most difficult public health problem. Underlying the major cause of death rates of children is important to achieve significant improvement in public health and in controlling motherly and children’s deaths. Thus, to improve the health status of mothers and newborn policymakers has set guidelines and solved these risk factors with appropriate intervention. Enclosing appropriate guidelines and policies to decrease child death will protect the sustainability in achieving the decrease in early newborn mortality [3, 4].
The most associated factors of the under-five children death rate are low birth weight, source of drinking water, toilet facilities, family wealth index, and congenital abnormalities [5, 6]. So, to decrease the high death rate of a child and the prevalence of complications in the early newborn period and to ensure the survival of under-five children, and newborn infants, high-quality antenatal care, professional delivery support, and postnatal care service must be taken.
Under-five children death rate in Ethiopia has evidenced a continuous decreasing trend in the previous fifteen years. On the other hand, although under-five children death rates were reduced from 88 deaths per 1,000 pregnancies in 2011 to 67 deaths per 1,000 pregnancies in 2016, it has remained stable high. According to the 2016 Ethiopia Demographic and Health Surveys (EDHS), the Benishangul-Gumuz Regional State is experiencing a higher under-five children death rate of 98 per 1,000 pregnancies, compared to that of the national average death rate of 67 per 1,000 pregnancies [7, 8].
Ethiopia is one of the nations that succeeded in the fourth-millennium development goal promising to decrease under-five children’s deaths in 2015. Even though there is a high reduction in the child death rate in Ethiopia; in the Benishangul-Gumuz Regional State under-five child death rate still remains high. Therefore, a considerable reduction in the under-five child death rate is critical to attaining this goal in the future. Previous research works stated that the decline in the Benishangul-Gumuz Regional State under-five child death rate over the last three decades has been slower than a decline at the national level.
Interventions to decrease under-five children's death rate are an essential concern and belong to improving motherly health care, where it is important for monitoring the current health care programs and formulating policies on improving the current situation for motherly and children's health status. Moreover, knowledge of the risk factors associated with the under-five children death rate is important to monitor the development of intensive and evidence-based health interventions to reduce newborn deaths [5, 9].
In spite of the fact that the majority of research has been done on the identification of risk factors that are associated with infant and neonatal death at the country level, there are limited studies that look at under-five child death and its predictor factors at the regional level. Such studies miss an important point of policymakers as the country-level result may not show the exact situation at the regional level. To solve this gap, the author conducted an all-inclusive cross-sectional study design of the recent 2016 EDHS, to explore the major predictor factors of under-five child death in the Benishangul-Gumuz Regional State, taking into consideration various demographic, socioeconomic, health, and environmental predictor factors in the Benishangul-Gumuz Regional State, Ethiopia [8].
Therefore, the objective of this study was to assess the major predictor factors of under-five children's deaths in the Benishangul-Gumuz Regional State, Ethiopia.
The significance of this investigation is that the research outcome will be helpful in strengthening the regional and country-level policies and intervention strategies targeted at decreasing under-five child deaths in Ethiopia. The research will also serve as a baseline for further researchers who are going to undertake other investigations in the area.
Methods
Source of data, study design, and study period: This investigation used a secondary analysis of a community-based retrospective cross-sectional study design regarding the data from the 2016 EDHS. The survey was conducted by the Central Statistics Agency (CSA) authority, the ministry of health, and the Ethiopian Public Health Institute (EPHI) from January 18–June 27, 2016. This was sponsored by the United States Agency for International Development (USAID). The data was found from the Demographic Health Survey (DHS) Measure Program with permission [10].
The survey conducted has information on a range of socioeconomic and demographic predictor factors of the population countrywide. Ethiopia has nine Regional States and two administrative cities. The survey used a two-stage sample survey study design. In the first stage sample survey study design 202 in the urban areas and 443 in the rural areas sample were selected with probability proportional to size. Second, the stage sample survey study design involved the selection of 28 households per cluster of equal probability systematic sample selection of the newly formed household list. The 2016 EDHS dataset has three questionnaires: the household questionnaire, the woman’s questionnaire, and the man’s questionnaire. All women of reproductive age 15–49 years and who were either steady residents of the chosen households or who survived in the household at least one night before the survey was conducted, were eligible for the interview. Data was collected through face-to-face interviews with women that met the eligibility criteria.
Sample size determination
A total of 15,683 women of the reproductive age group, and 12,688 men aged (15–59 years) in 16,650 households were interviewed in the 2016 EDHS report in Ethiopia. In the Benishangul-Gumuz Regional State, 986 total live births were reported in the previous five years preceding the survey. Then, children with full recorded information on the survey during the last five years were identified [8]. Finally, a total of 906 children that have completed information about all the predictor factors considered were involved in the study.
Data collection procedure and description of study area: The study used the Benishangul Gumuz Regional State DHS data. The region has a predicted area of 51,000 KM2. It is found in the Western part of Ethiopia. It shares common borders with the Amhara Regional State in the East, the Republic of Sudan in the Northwest, and the Oromia Regional State in the South. The region is divided into three administrative zones and 19 districts. About three-fourths (75%) of the region is categorized as low land, which is below 1,500 meters above sea level. The altitude ranges from 550–2,500 meters above sea level. Based on the 2011 CSA estimates, the region has a total of 982, 004 population. About 90% of the total population lives in rural areas, indicating that there is a very low level of urbanization. The agricultural sector is the main economic activity followed by traditional gold mining. The region has two general hospitals, 28 health centers, and 339 health posts [11].
Variables of the study
Independent variables: Predictor factors of under-five child deaths in this study were selected from the available prior studies on the subject. An essential mother and child demographic description explored from a theoretical perspective and various works of literature on under-five children survival are presented in Table 1[1–2].
Table 1: Operational description and categorization of independent variables used in the study.
| Independent variables | Description and categorization of variables |
| Residence | Place of residence (urban, rural) |
| Source of drinking water | Source of drinking water (protected well,piped water, unprotected well) |
| Toilet facility | Mother’s toilet facility (with facility, no facility) |
| Religion | Mother’s religion status (Muslim, other religion group, orthodox) |
| Family size | Family size of households (discrete) |
| Sex of household head | Sex of household head in the family members (male, female) |
| Wealth index | Family wealth index of households (rich, middle, poor) |
| Parity | Total children ever born (3 and below, 4–5, 6–8, 9 and above) |
| Contraceptive use | Mother’s contraceptive use (yes, no) |
| Marital status | Mother’s marital status (married,divorced, single, widowed) |
| Mother’s occupation | Mother’s occupational status (non-agricultural sector, agricultural sector, not working) |
| Type of child birth | Type of child birth (single, multiple) |
Dependent variable
During the collection of the DHS dataset, mothers were requested to report every pregnancy loss and death of a live-born child. Then, the under-five child death rate will be obtained as the sum of the death of children within the probability of dying between birth and the fifth birthday.
The dependent variable for this study was considered to be the length (survival) of time measured in months from date of birth until time-to-death (censor) on under–five children. Thus, the outcome variable for the child is categorized as dichotomous, represented by a random variable that takes the value “1” with a probability of death (died) and the value “0” with a probability of alive (censored), such that

Operational definitions: Under-five children mortality: The under-five child mortality is the death of a child before reaching the age of 5 years old.
Time to death: The time is calculated from the start of observation until the occurrence of the outcome of observation (i.e., death or censoring).
Death: In this paper, death referred to the study subject who had experienced the interest of event (had died) during the observation period and labeled as (1).
Censored: In this paper, censored is referred to the study subject who had not experienced death during the follow-up time. Study participants who were at the end of the study time before experiencing death were considered censored.
Statistical methods of data analysis
The investigation used descriptive statistics such as frequency and percentage of distribution to define the sample selected information. The Kaplan-Meier (K-M) survival curve was used to compare the survival probability of categorical variables among under-five years of age of children. Cox Proportional-Hazard (PH) regression model is used as the most appropriate method of survival analysis for time-to-event data.
Cox PH regression model was used to estimate the effect of socioeconomic and demographic predictor factors associated with under-five children's death rate (hazard rates with their 95% confidence intervals). The general structure of the Cox PH model is expressed as follows;
〖h(t)=h_o (t)*exp〗^((^(b_1 x_1 〖+ b〗_2 x_2 + b_3 x_3 + ………….. b_p x_p ))), were used to determine and check the impact of each covariate variable on the time-to-event.
Hazard function is identified by set of p covariates (x1 x2,x3……,xp), whose effect is measured by magnitude of the corresponding coefficients (b1,b2,b3……,bp ). The term (t) is called the baseline hazard for a time-to-death. The proportionality assumptions of Cox PH regression model analysis were checked on each predictor variable and on the overall test of proportionality. None of the predictor variables failed Cox PH regression model assumptions.
Results
Descriptive statistics: To identify the predictor factors associated with under-five children's death, 906 births within the five years before the survey were considered. The result from Table 2 showed that out of 906 births included in the study, 84 (9.3% [95%CI: 7.38, 11.2]) were reported under-five children's death rates. This showed that the ratio of under-five children death rates in Ethiopia to under-five death rates in the Benishangul-Gumuz Regional State is 6.7/100 to 9.3/100. The possible explanation for this variation might be that under-five child deaths are likely being missed as women are afraid of reporting pregnancy terminations due to some traditional cultures and religions in the community. Therefore, the analysis found that the prevalence of under-five death rates was 93 per 1,000 births for the five years preceding the survey.
Table 2 presented the frequency and percentage distribution of the selected predictor factors of under-five death rates in the study. About three-fifths (61.1%) of the births in the study had belonged to a woman with a poor wealth index, one-fifth (21.5%) belonged to the rich wealth index and one-sixth (17.4%) were in the middle wealth index group. Concerning the mother’s occupational status, nearly half of the mothers were working in the agricultural sector, 38.4% did not work in any sector and one-sixth (15.8%) were working in the non-agricultural sector.
On the other hand, when the sex of the household head of the family was concerned, four-fifth (81.7%) was reported as male household head. Of the majority of the mothers two-fifths (40.1%) had less than four children in their lifetime, 9.4% of respondents had at least nine children and 24.3% had 6 – 8 children in their life. The family wealth index was inversely proportional to under-five child death, as the family wealth index increases from poor to middle and then to rich, under-five child death decreases from 6.6 to 1.1%. Thus, those children born to poor wealth index groups have the highest percentage of under-five child death rate than any of the higher wealth index groups.
Children belonging to his/her mothers who work in the non-agricultural sector had a comparatively higher percentage (2.5%) of the under-five child death rate. Concerning sanitation indicator variables, the proportions of under-five child death rate was higher among mothers using unprotected drinking water than that of piped drinking water users. Similarly, under-five child death rates were higher among mothers with no toilet facility than that with facilities (see Table 2).
Moreover, to the descriptive statistics given in Table 2, Kaplan-Meier (K-M) survival curve estimators are plotted for the most important predictor variables (see Figure 1–4). These sample K-M curves showed that under-five years old children who use unprotected water drink sources, have parity (6–8, 9 and above), being a non-agricultural sector of mother’s occupational status, and have multiple types of childbirth have a short survival time compared to those reference categories.
| Status of child | ||||
| Covariate variables | Censored | Death | Total frequency (N = 906) | Total percent (%) |
| Residence | ||||
| Urban | 99 | 7 | 106 | 11.7 |
| Rural | 723 | 77 | 800 | 88.3 |
| Source of drinking water | ||||
| Protected well | 558 | 47 | 605 | 66.8 |
| Piped water | 75 | 3 | 78 | 8.6 |
| Unprotected well | 189 | 34 | 223 | 24.6 |
| Toilet facility | ||||
| With facility | 640 | 53 | 693 | 76.5 |
| No facility | 182 | 31 | 213 | 23.5 |
| Religion | ||||
| Muslim | 368 | 43 | 411 | 45.4 |
| Orthodox | 293 | 23 | 316 | 34.9 |
| Other religion group | 161 | 18 | 179 | 19.8 |
| Sex of household head | ||||
| Male | 675 | 65 | 740 | 81.7 |
| Female | 147 | 19 | 166 | 18.3 |
| Wealth index | ||||
| Rich | 185 | 10 | 195 | 21.5 |
| Middle | 144 | 14 | 158 | 17.4 |
| Poor | 493 | 60 | 553 | 61.1 |
| Parity | ||||
| 3 and below | 339 | 24 | 363 | 40.1 |
| 4 – 5 | 221 | 17 | 238 | 26.3 |
| 6 – 8 | 195 | 25 | 220 | 24.3 |
| 9 and above | 67 | 18 | 85 | 9.4 |
| Contraceptive use | ||||
| No | 590 | 69 | 659 | 72.7 |
| Yes | 232 | 15 | 247 | 27.3 |
| Marital status | ||||
| Married | 749 | 69 | 818 | 90.3 |
| Divorced | 38 | 7 | 45 | 5.0 |
| Single | 21 | 4 | 25 | 2.8 |
| Widowed | 14 | 4 | 18 | 2.0 |
| Mother’s occupation | ||||
| Nonagricultural Sector | 120 | 23 | 143 | 15.8 |
| Agricultural Sector | 395 | 20 | 415 | 45.8 |
| Not Working | 307 | 41 | 348 | 38.4 |
| Type of child birth | ||||
| Single | 801 | 73 | 874 | 96.5 |
| Multiple | 21 | 11 | 32 | 3.5 |
Table 2: Distribution of under-five children death by selected maternal and child demographic characteristics, health, and environmental predictor factors in the Benishangul-Gumuz Regional State, 2016 (N = 906).
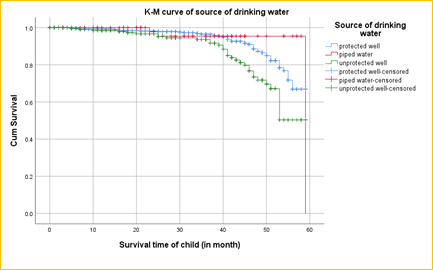
Figure 1: Plot of K-M estimates for source of drinking water
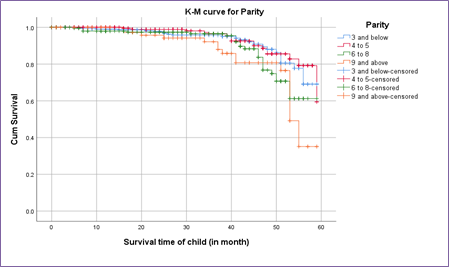
Figure 2: Plot of K-M estimates for parity
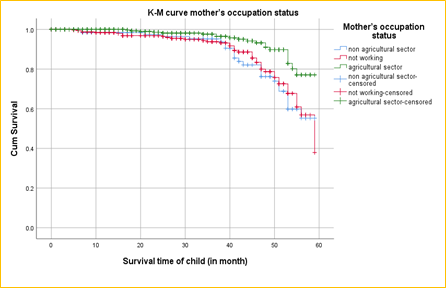
Figure 3: Plot of K-M estimates for mother’s occupation status
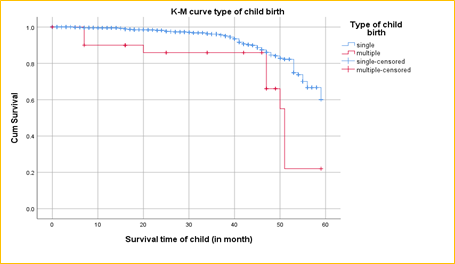
Figure 4: Plot of K-M estimates for type of child birth
Predictors of time to death
Cox PH regression and assessment of goodness of fit of the model results: Cox PH regression model analysis was used to examine the effect of each covariate variable on the under-five year's children death rate.
The result of the Likelihood, Wald, and Score (log-rank) test had a p-value = 0.000, which is statistically significant at the 5% level of significance and the concordance = 0.72 (se = 0.038) illustrating that the data and the model were in good fit. Further, since the overall Global test (p-value = 0.78) for all predictor factors is > 0.05 and none of the predictor variables failed the Cox PH regression model of the necessary assumption. Therefore, the model violated the Cox PH regression model proportionality assumptions and the Cox PH regression model is mathematically adequate.
Interpretation of Cox PH regression model results: The multivariable Cox PH regression model analysis of predictor factors associated with the under-five death rate was presented in Table 3. The relationship between the probability of under-five death rates and the socioeconomic and demographic predictor factors was explored using hazard rates.
The result showed the source of drinking water, family size, parity, mother’s occupation and type of childbirth were statistically significant predictor factors of under-five child death. However, variables residence, toilet facility, religion, sex of household head, wealth index, contraceptive use, and marital status were found insignificant.
The hazard of death in under-five children who had multiple births was 2.17 times higher as compared to children with singleton births (AHR = 2.17; 95% CI (1.17–4.20)). Besides, compared to an agricultural sector of mother’s occupation, children whose mother’s occupation of the non-agricultural sector were more likely to die before celebrating their fifth year of birth, keeping all other variables constant. The hazard rate of under-five child death rate was 39% times less among agricultural sector children than in the non-agricultural sector (AHR = 0.39; 95% CI (0.20–0.76)).
The availability of sources of drinking water had a positive impact on the under-five death rate. The hazards of the under-five death rate were 2.13 times higher among children belonging to a mother without a protected water well source of drinking water than those with a source of drinking water (AHR = 2.13; 95% CI (1.32–3.42)).
For the variable family size, the hazard rates of under-five deaths were about 0.74% times lower as the family size decreased by one family size (AHR = 0.74; 95% CI (0.60–0.93)).
Moreover, Table 3 also showed that the hazard rates of under-five deaths were higher among children born to mothers, those total children ever born between 6 - 8, and 9 and above (AHR = 3.16; 95% CI (1.40–7.16)) and (AHR = 7.86; 95% CI (2.23–27.72)), respectively, compared to that of 3 and below the total number of children.
Table 3 Bi-variable and multivariable Cox PH regression model analysis of predictor factors associated with under-five children died in the Benishangul-Gumuz Regional State, Ethiopia, 2016 (N = 906).
| Covariate variables | Bi-variable Cox PH regression | Multivariable Cox PH regression | ||||||
| 95% CI for CHR | 95% CI for AHR | |||||||
| CHR | LB | UB | P-value | AHR | LB | UB | P-value | |
| Residence (ref.= urban) | 1.0 | 1.0 | ||||||
| Rural | 1.46 | 0.67 | 3.17 | 0.335 | 0.61 | 0.27 | 1.37 | 0.228 |
| Source of drinking water (ref.= protected well) | 1.0 | 1.0 | ||||||
| Piped water | 0.65 | 0.21 | 2.00 | 0.452 | 1.01 | 0.31 | 3.32 | 0.989 |
| Unprotected well | 2.12 | 1.37 | 3.29 | 0.001* | 2.13 | 1.32 | 3.42 | 0.002* |
| Toilet facility (ref.= with facility) | 1.0 | 1.0 | ||||||
| No facility | 2.03 | 1.30 | 3.16 | 0.002 * | 1.60 | 0.91 | 2.78 | 0.100 |
| Religion (ref.= Muslim) | 1.0 | 1.0 | ||||||
| Orthodox | 0.66 | 1.52 | 0.40 | 0.106 | 0.67 | 0.36 | 1.24 | 0.204 |
| Other religion group | 0.82 | 0.48 | 1.40 | 0.469 | 0.612 | 0.32 | 1.17 | 0.136 |
| Family size | 0.92 | 0.81 | 1.05 | 0.239 | 0.74 | 0.60 | 0.93 | 0.008* |
| Sex of household head (ref.= male) | 1.0 | 1.0 | ||||||
| Female | 1.4 | 0.85 | 2.30 | 0.183 | 0.96 | 0.55 | 1.69 | 0.899 |
| Wealth index (ref.= rich) | 1.0 | 1.0 | ||||||
| Middle | 1.55 | 0.69 | 3.45 | 0.2891 | 1.29 | 0.519 | 3.19 | 0.586 |
| Poor | 2.43 | 1.28 | 4.63 | 0.007* | 1.36 | 0.60 | 3.10 | 0.468 |
| Parity (ref.= 3 and below) | 1.0 | 1.0 | ||||||
| 4 – 5 | 0.84 | 0.45 | 1.55 | 0.575 | 1.35 | 0.62 | 2.96 | 0.450 |
| 6 – 8 | 1.6 | 0.91 | 2.78 | 0.100 | 3.16 | 1.40 | 7.16 | 0.006* |
| 9 and above | 2.25 | 1.25 | 4.06 | 0.007 * | 7.86 | 2.23 | 27.72 | 0.001* |
| Contraceptive use (ref.= no) | 1.0 | 1.0 | ||||||
| Yes | 0.52 | 0.30 | 0.90 | 0.76 | 0.41 | 1.43 | 0.400 | |
| Marital status (ref.= married) | 1.0 | 1.0 | ||||||
| Divorced | 1.88 | 0.97 | 3.66 | 0.062 | 1.65 | 0.85 | 3.19 | 0.138 |
| Single | 2.20 | 0.94 | 5.16 | 0.069 | 1.43 | 0.58 | 3.51 | 0.433 |
| Widowed | 1.72 | 0.63 | 4.66 | 0.290 | 0.52 | 0.14 | 1.87 | 0.315 |
| Mother’s occupation (ref.=non-agricultural Sector) | 1.0 | 1.0 | ||||||
| Agricultural sector | 0.39 | 0.22 | 0.71 | 0.002* | 0.40 | 0.20 | 0.76 | 0.005* |
| Not Working | 0.95 | 0.57 | 1.59 | 0.845 | 0.98 | 0.55 | 1.73 | 0.932 |
| Type of child birth (ref.= single) | 1.0 | 1.0 | ||||||
| Multiple | 3.2 | 1.69 | 6.08 | 0.000* | 2.17 | 1.17 | 4.20 | 0.022* |
CHR: Crude Hazard Rate, AHR: Adjusted Hazard Rate, ref.: Reference, * Significant at 5% level of significance, LB: Lower Boundary, UB; Upper Boundary.
Discussion
The study empirically investigated and identified the predictor factors that were associated with under-five children's death in the Benishangul-Gumuz Regional State, using the 2016 EDHS datasets. The hazards of under-five children's death rate were more likely among multiple compared to singletons births. This is similar to previous studies done in Ethiopia that showed a significant association between under-five children's death rate [12–14]. Moreover, multiple birth types might result in under-nutrition because of inadequate breast milk as well as infections due to inappropriate procedures of feeding.
In this current study, parity is also significantly associated with under-five children's death rate. The hazards of under-five children death rate were higher for a child with a greater total number of children ever born. This suggests that the under-five death rate increases as parity increases [2, 12] but in contrast to other studies [15, 16]. This might be because mothers with greater parity might be busy caring for several children in the family size and may not give special attention to the health care service of their last child. Moreover, mothers with greater parity had enough children so they might be careless in seeking appropriate care from the health facility service for this child [17].
On the other hand, there were no significant differences in the risk factors of under-five children's death rate between residence places. This finding is consistent with previous studies [18].
Another essential demographic risk factor significantly associated with the under-five children death rate was family size. Having greater members of family size were at a higher risk of death under-five children mortality. Previous research had also stated a significant association between the under-five children death rate and family size [18]. This might be due to the lack of adequate use of infrastructure and mothers busy caring for many children in the household.
The source of drinking water was also an essential predictor factor significantly correlated with the under-five children's death rate in the Benishangul-Gumuz Regional State. Children, whose mothers were using unprotected drinking water, were more likely to die in the early newborn period than those who used protected well water. This is because using unsafe water drinks is regarded as the major risk factor of infectious diseases such as diarrhea infection and intestinal parasites [5, 19, 20]. Furthermore, the occupation of the mother was also found to be a significant predictor factor of under-five children's death. Compared to children whose mothers were working in the non-agricultural sector those children whose mothers were working in the agricultural sector had a significantly higher risk of death rate [5, 21].
Generally, the trend revealed that although the national level (Ethiopia) has attained the fourth-millennium development goal, in under-five children death rate, however, the progress is very slow in the Benishangul-Gumuz Regional State.
Limitations of the study
This present investigation used a national-level sample survey dataset, which enhances conclusions for the entire regional level. Moreover, since it is based on the regional-level survey dataset the investigation has the potential to give special awareness to policy-makers and program planners to design suitable intervention strategies at regional levels. However, this investigation is regarding secondary data the main limitation is; the study was a mother's recall of events that conduct for the previous five years earlier the survey, which indicates there is a subject-to-recall bias. Probably this may be because women are afraid of reporting pregnancy terminations because of some traditional cultures and religious perceptions in the community.
Conclusions
This investigation was carried out to assess associated predictor factors of the under-five children's death rate in the Benishangul-Gumuz Regional State. Both descriptive statistics and the Cox PH regression model were used to analyze the data. The Benishangul-Gumuz Regional State has experienced a higher under-five children death rate than that of the national level. The Cox PH regression model analysis showed that being multiple births, an unprotected good source of drinking water, parity (6–8), and parity (9 and above) were found as factors that positively associated with the risk of under-five children death.
On the other hand, mothers working in agricultural sectors and decreasing family size were found factors that were inversely associated with under-five children's death. However, variables residence, toilet facility, religion, sex of household head, wealth index, contraceptive use, and marital status were found insignificant.
Moreover, healthcare service providers must give special attention and direct care to those mothers who have multiple children born during delivery service and they should give awareness about family planning is essential to remove deaths due to several family sizes and ever-born children in a household. Finally, both government policymakers and other concerned organizations should be given special attention to the major predictor factors among under-five children's death rate and do greater emphasis on decreasing under-five children's death, and health intervention policies must be studied.
Abbreviations
AHR: Adjusted Hazards Rate;
CI: Confidence Interval; CSA:
Central Statistical Agency;
DHS: Demographic and Health Survey;
EDHS: Ethiopian Demographic and Health Survey;
EPHI: Ethiopian Public Health Institute;
K-M: Kaplan-Meier; PH: Proportional-Hazard;
USAID: United States Agency for International Development
Declarations
Acknowledgments
The author is most thankful to the DHS Measure Program for providing the datasets for the investigation. Besides, the authors wish to thank the anonymous reviewers and editor for their numerous constructive comments.
Authors’ contributions
GGG is involved from the inception to design, acquisition of data, analysis, and interpretation, drafting the manuscript, revising critically the manuscript, and editing the manuscript for the final submission. The author read and approved the final manuscript.
Funding
The author has no support or funding to report.
Availability of data and materials
The data used during the current investigation are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
Ethics approval for this study was not required since the data is secondary and is available in the public domain.
Consent for publication
Not applicable.
Competing interests
The author declares that there was no competing interest.
References
- Zewudie AT, Gelagay AA, Enyew EF. (2016). Determinants of under-five child mortality in Ethiopia: analysis using Ethiopian demographic health survey. Int J Pediatr.
Publisher | Google Scholor - Gebretsadik S, Gabreyohannes E. (2016). Determinants of under-five mortality in high mortality regions of Ethiopia: an analysis of the 2011 Ethiopia demographic and health survey data. Int J Popul Res.
Publisher | Google Scholor - World Health Organization. (2006). Neonatal and perinatal mortality: country, regional and global estimates. Geneva: World Health Organization.
Publisher | Google Scholor - Y G, S B. (2016). Survival analysis of under-five mortality of children and its associated risk factors in Ethiopia. J Biosens Bioelectron, 7:3.
Publisher | Google Scholor - Woldeamanuel BT, Gelebo KK (2019). Statistical analysis of socioeconomic and demographic correlates of perinatal mortality in Tigray region, Ethiopia: a cross sectional study. BMC Public Health, 19:1301.
Publisher | Google Scholor - Allanson, E. R., Muller, M., & Pattinson, R. C. (2015). Causes of perinatal mortality and associated maternal complications in a south Africanprovince: challenges in predicting poor outcomes. BMC pregnancy and childbirth, 15:37.
Publisher | Google Scholor - Central Statistical Agency [Ethiopia] and ICF. (2011). Ethiopia demographic and health survey. Addis Ababa, Ethiopia and Calverton, Maryland, USA: CSA and ICF International.
Publisher | Google Scholor - Central Statistical Agency (CSA) [Ethiopia] and ICF. (2016). Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF.
Publisher | Google Scholor - Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I. et al. (2010): child health epidemiology reference group of WHO and UNICEF. Lancet. 2010; 375 (9730):1969–1987.
Publisher | Google Scholor - Measure DHS, The DHS. Program: demographic and health surveys. Rockville: ICF Macro.
Publisher | Google Scholor - CSA: Annual Statistical Abstract (2011). Addis Ababa: Central Statistical Agency.
Publisher | Google Scholor - Worku MG, Teshale AB, Tesema GA (2021). Determinants of under-five mortality in the high mortality regions of Ethiopia: mixedeffect logistic regression analysis. Archives of Public Health, (2021)79:55.
Publisher | Google Scholor - Fenta SM, Fenta HM (2020). Risk factors of child mortality in Ethiopia: Application of multilevel two-part model. PLoS ONE ,15(8):e0237640.
Publisher | Google Scholor - Berelie Y, Yismaw L, Tesfa E, Alene M. (2019). Risk factors for under-five mortality in Ethiopia: evidence from the 2016 Ethiopian demographic and health survey. S Afr J Child Health. 13(3):137-140-140.
Publisher | Google Scholor - Ettarh R, Kimani J. (2012). Determinants of under-five mortality in rural and urban Kenya. Rural Remote Health, 12:1812.
Publisher | Google Scholor - Mehretie Adinew Y, Feleke SA, Mengesha ZB, Workie SB. (2017). Childhood mortality: trends and determinants in Ethiopia from 1990 to 2015—a systematic review. Adv Public Health.
Publisher | Google Scholor - Deribew A, Tessema F, Girma B. (2007). Determinants of under-five mortality in Gilgel gibe field research center, Southwest Ethiopia. Ethiop J Health Dev. 21(2):117–124.
Publisher | Google Scholor - Statistical Modeling of the Number of Deaths of Children in Bangladesh
Publisher | Google Scholor - Saffron, Lale Say, João-Paulo Souza, Carol J Hogue, Dinorah L Calles, et al. (2011) The relationship between maternal education and mortality among women giving birth in health care institutions: Analysis of the cross sectional WHO Global Survey on Maternal and Perinatal Health. BMC Public Health, 11:606.
Publisher | Google Scholor - Berelie Y,Yismaw L, Tesfa E, Alene M(2019). Risk factors for under-five mortality in Ethiopia: Evidence from the 2016 Ethiopian Demographic and Health Survey. S Afr J Child Health, 13(3):137-140.
Publisher | Google Scholor - Mostafa A. Arafa, Taher Amine and Moataz Abdel (2007): Fattah Association of Maternal Work with Adverse Perinatal Outcome Canadian. Journal of Public Health / Revue Canadienne de Santé Publique, 98(3):217-221.
Publisher | Google Scholor














