

Research Article
Powdered Vancomycin as Preventive Treatment in Lumbar Surgical Wound Infection
Department of Neurosurgery, General University Hospital of Valencia, Valencia, Spain.
*Corresponding Author: Inaki Arrotegui Department of Neurosurgery, General University Hospital of Valencia, Valencia, Spain.
Citation: Arrotegui, I. (2022). Powdered Vancomycin as Preventive Treatment in Lumbar Surgical Wound Infection. Journal of Clinical Surgery and Surgical Research, BRS Publishers. 1(1); DOI: 10.59657/2992-9989.brs.22.003
Copyright: © 2022 Inaki Arrotegui, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: October 25, 2022 | Accepted: November 21, 2022 | Published: November 28, 2022
Abstract
Summary: Due to its pharmacodynamic capabilities and its properties at the cell membrane level, vancomycin is considered one of the glycopeptides for clinical use as first-line treatment against most Gram-positive germs.
Objective: To analyze the efficacy of topical vancomycin in the prevention of infections at the surgical wound level in spinal surgery.
Material and methods: A non-randomized, observational and comparative cohort study of 60 patients with instrumented lumbar spine surgery was carried out in the period between June 2021 and june 2022. In 30 cases with placement of 1 g of topical vancomycin group 1, and 30 did not Group 2, in a nonrandomized manner. Patients were followed up during the first 90 postoperative days.
Results: The relationship between vancomycin-infection was not statistically significant, 3 cases of wound infection were identified in the group without vancomycin, it was found that the factor of age over 50 years and Diabetic or immunosuppressed and obesity were predisposing causes respectively, although without p ≤ 0.05, another finding was the RR 2.0208 in an instrumented lumbar level but without significant difference; the main characteristics in the 3 patients with wound infection were only present in the group without vancomycin, identifying.
Conclusions: There is no statistical significance in our study that topical vancomycin plays a fundamental role in the prevention of infections at the surgical wound level in spinal surgery. However, it is important to note that all the infected patients in this study belonged to group 2 (without the use of vancomycin).
Keywords: vancomycin; lumbar surgical; spinal surgery
Introduction
The advent of infectious processes in spinal surgery is currently considered a major health problem. Its incidence varies depending on multiple factors, and it is estimated that it ranges from 2 to 13% of patients undergoing spinal surgery [1-2]. The application of vancomycin within the surgical site is consolidated as a novel alternative for the prevention of surgical site infections. Due to its low cost, wide availability and easy application, it is gaining increasing acceptance among spine surgeons, based on the recommendations established by the North American Spine Society (NASS) [3,4]. Regarding the topical route, there is evidence that the intrawound application of antibiotics can minimize local infection after surgery. In procedures performed at the level of the spine, vancomycin has gained importance in its topical use as prophylaxisThe most frequent microorganisms in surgical wound infections are S. epidermidis and S. aureus, which are sensitive to the spectrum of topical vancomycin, so current studies support the association in reducing the rate of infections using the antibiotic intralesional route [5,6].The objective of this study is to determine the efficacy of topical vancomycin in the prevention of infections at the surgical wound level in spinal surgery.
Material and Methods
A non-randomized, observational, comparative cohort study was conducted. A total of 60 patients with instrumented lumbar spine surgery were prospectively analyzed in the period between June 2021 and June 2022. In 30 cases 1 g of topical vancomycin was placed, and in 30 not, in a non-randomized manner, according to the preference of each surgeon. Patients were followed up during the first 90 postoperative days.
Group 1 patients were identified as those who received a 1-g ampoule of powdered vancomycin on the surgical wound bed below the muscle plane prior to muscle and fascia closure (Figures 1 and 2). In group B, no local vancomycin was applied.
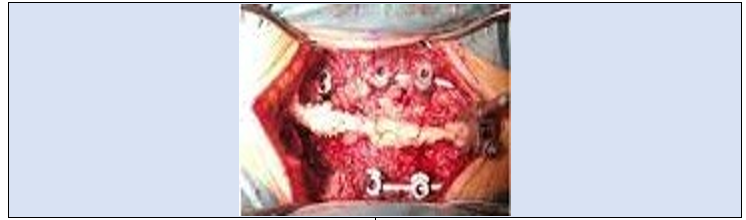
Figure 1: Vancomycin in place. deep plane

Figure 2: Powder vancomycin on the surperficial plane
All patients simultaneously received 1 g of intravenous cephalothin 30 minutes before the skin incision, and continued with this antibiotic every eight hours during the first 24 hours after surgery due to hospital antimicrobial management protocols [7].
Patients operated on with lumbar spine instrumentation for degenerative pathologies were included.
Patient follow-up was in person, clinically monitoring the surgical wound and signs related to infection such as fever, erythema or inflammation of the surgical wound, and atypical pain.
We defined as "early infections" the group that includes acute and subacute infections, for which they included all infections that manifested within three months after the intervention. Similarly, superficial infections were defined as those in which the clinical signs of infection were located above the fascia and subcutaneous cellular tissue, and deep as those in which signs of infection were found below these tissues [8].
The data was transferred to an Excel spreadsheet (Microsoft 2019) and analyzed with the Epi Info CDC statistical analysis program. Values of p ≤ 0.05 were accepted as statistically significant data [9].
A total of 60 patients were included and studied, 30 patients belonging to group 1 (use of vancomycin Fig III) and group 2, 30 without use of vancomycin. Among the patients in group A1, an average age of 65 with SD of 14.9056 was found, and in group 2 68 with SD of 14.0619. In the aspect of sex, a predominance was found for the male sex in the group with vancomycin, in the group without vancomycin the female sex was the most predominant.
The most reported comorbidity was diabetes mellitus with a total of 14 people, the opposite was the case in the group without vancomycin, a total of 17.
In our study, 3 cases of surgical wound infection were reported, these five belonged to group 2 without vancomycin. Of these cases, 2 were men and one woman. There was only one case of deep-late infection in a 75-year-old patient. In all cases of infection, patients presented with associated comorbidities, predominantly diabetes mellitus.
Discussion
Surgical site infection (SSI) is one of the most common nosocomial infections. Approximately 500,000 CSRs are registered in the United States annually, with a higher cost to ten billion dollars in health spending [10].
The rate of infection after spinal fusion is estimated between 2% and 3% of the cases operated on. Treatment for these infections requires multiple hospitalizations, additional surgeries, as well as prolonged antibiotic treatment, which raises up to 4 times the total value of the attention of the affected person [11].
The risk factors most closely related to the development of SSI include: patient obesity, advanced age, states of malnutrition, prolonged surgical times, smoker, blood transfusions, cancer, myelopathy as a condition as well as a history of infections in previous surgical site [12].
The microorganism most frequently involved in SSI after spinal surgery is Staphylococcus aureus, closely followed by Staphylococcus epidermidis [13].
In epidemiological studies of cultures of infected surgical sites in adults, it was found that around 80% of these grew Gram-positive bacteria, such as those already mentioned, as well as Streptococcus mutans and Enterococcus fecalis [14].
Only 20% of the microorganisms were Gram negative, predominantly: Corynebacteria sp, Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis and Pseudomonas aeruginosa.
The goal of preoperative antibiotic prophylaxis is to specifically combat the bacteria most closely related to SSI. The routine protocol contemplates the prophylactic use of cephalosporins intravenous and skin preparation for incision as sterilization methods (chlorhexidine) [14].
vancomycin is glycopeptide produced by Streptococcus orientalis. This antibiotic is an inhibitor bacteriostatic of protein synthesis on the ribosomes. It is considered active Mainly against Gram bacteria positive; within the sensitive strains may mention: S. aureus, S. epidermidis, S. pyogenes, S. pneumoniae, and Streptococcus viridans [15].
On the other hand, there is resistance to vancomycin on all gram bacillinegative and mycobacteria. The mechanism of action is to inhibit the
bacterial cell wall synthesis sensitive, by joining with the ending’s High affinity D-alanyl-D-alanine in the cell parietal precursor units [16].
The drug has a bactericidal effect on dividing microorganisms. The therapeutic use should be only to combat Seriou’s infections, particularly those caused by staphylococci resistant to penicillins, among which can be include: pneumonia, empyema, endocarditis, osteomyelitis and abscesses [17].
Adverse effects of vancomycin are varied, mainly reactions of hypersensitivity, such as skin macules and anaphylaxis. Red man syndrome presents as hyperemia and dermal flushing widespread, caused by a direct effect of vancomycin on mast cells, which causes the release of histamine. The incidence of anaphylactic reactions ranges from 1.6% to 35% in adults [18].
Since 2009, the use of vancomycin powder in doses between 1 and 2
grams at the surgical site. Its use has come expanding on the global stage, though Certainly empirically [19].
Initially was used in instrumentation surgeries of spine, due to high rates of SSI. Application of vancomycin powder performed on the exposed vertebra, in the muscle, fascia or subcutaneous tissue, prior to closure of the surgical wound.Local vancomycin reaches adequate inhibitory concentration minimal at the site of the surgical wound, without have systemic side effects, such as hypotension and nephrotoxicity, which are more frequent with intravenous applicationof this antibiotic [20].
The widespread use of vancomycin powder intraoperative could increase the incidence of spinal infections by microorganisms Gram negative or polymicrobial flora.
However, there are no large studies comparisons that show the increase in these microorganisms by the selection of the bacterial flora with the use of vancomycin local.
The potential development of resistance bacteria to vancomycin and the appearance of new strains is a question to be defined.
Figure 3: vancomycin powder
Conclusion
Sufficient evidence is still lacking regarding to the widespread use of vancomycin powder for local application in neurosurgery. Without however, it has been shown in several studies that at least in patients with prostheses and spinal instrumentation, antibiotic is effective in reducing the risk of ISQ.
The use of vancomycin by route direct is an economical option, accessible and easy to use in instrumentation spinal cord, which can greatly benefit significant the evolution of the patient and the health system costs. Furthermore, the profile risk versus benefit in the use of this method is quite favorable.
References
- Hiroshi T, Yasuaki I, Yuichirou Y. (2018). Use of intrawound vancomycin powder against postoperative infection after spine surgery. Spine Surg Relat Res. 2 (1): 18-22.
Publisher | Google Scholor - Abhiram G, Alex R, Torin C. (2019). Selection pressures of vancomycin powder use in spine surgery: a metaanalysis. Spine J 19 (6): 1076-1084.
Publisher | Google Scholor - Sipeng L, Hongtao R, Xueqin Z. (2019). Meta analysis of topical vancomycin powder for microbial profile in spinal surgical site infections. Eur Spine J 28 (12): 2972-2980.
Publisher | Google Scholor - Sombat K, Sirichai S, Chaiwat P. (2019). Comparison between 1 g and 2 g of intrawound vancomycin powder application for prophylaxis in posterior instrumented thoracic or lumbosacral spine surgery: a preliminary report. Asian J Neurosurg. 14: 710-714.
Publisher | Google Scholor - Justin V, Cumhur O, Sebastiaan P. (2019). The efficacy of intrawound vancomycin powder and povidone-iodine irrigation to prevent surgical site infections in complex instrumented spine surgery. Spine J. 19 (10): 1648-1656.
Publisher | Google Scholor - Alcalá G, Paternina A, Moscote L. (2014). Aplicación de vancomicina en polvo dentro de la herida quirúrgica durante cirugías de columna: revisión sistemática y metaanálisis. Rev Esp Cir Ortop Traumatol. 58 (3): 182-191.
Publisher | Google Scholor - Fabian L, Félix S, Martín G. (2018) Vancomicina tópica en la prevención de infecciones tempranas en cirugías instrumentadas espinales: serie de casos y revisión de la literatura. Rev Argent Neuroc. 32 (2): 158-164.
Publisher | Google Scholor - Savage JW, Anderson PA. (2013) An update on modifiable factors to reduce the risk of surgical site infections. Spine J. 13:1017---29.
Publisher | Google Scholor - Godil SS, Parker SL, O’Neill KR, Devin CJ, McGirt MJ. (2013) Comparative effectiveness and cost-benefit analysis of local application of vancomycin powder in posterior spinal fusion for spine trauma. J Neuro surg Spine. 19:331-335.
Publisher | Google Scholor - Chua K, Howden BP. (2009) Treating Gram-positive infections: Vancomycin update and the whys, wherefores and evidence base for continuous infusion of anti-Gram-positive antibiotics. Curr Opin Infect Dis. 22:525-534.
Publisher | Google Scholor - Epstein NE. (2011) Preoperative, intraoperative, and postoperative measures to further reduce spinal infections. Surg Neurol Int. 2:17.
Publisher | Google Scholor - Watter’s 3rd WC, Baisden J, Bono CM, Heggeness MH, Resnick DK, et al. (2009). Antibiotic prophylaxis in spine surgery: An evidence-based clinical guideline for the use of prophylactic antibiotics in spine surgery. Spine J. 9:142-146.
Publisher | Google Scholor - Kanj WW, Flynn JM, Spiegel DA, Dormans JP, Baldwin KD. (2013). Vancomycin prophylaxis of surgical site infection in clean orthopedic surgery. Orthopedics. 36:138-146
Publisher | Google Scholor - Glotzbecker MP, Vitale MG, Shea KG, Flynn JM. (2013) Surgeon practices regarding infection prevention for pediatric spinal surgery. J Pediatr Orthop. 33:694-699.
Publisher | Google Scholor - Vitale MG, Riedel MD, Glotzbecker MP, Matsumoto H, Roye DP, et al. (2013) Building consensus: Development of a best practice guideline (BPG) for surgical site infection (SSI) prevention in high-risk pediatric spine surgery. J Pediatr Orthop.33:471-478.
Publisher | Google Scholor - Chi J. (2012) Powder time? Reducing spinal postoperative infections with intrawound application of antibiotic powder. Neurosurgery. 70: N12-13.
Publisher | Google Scholor - Sweet FA, Roh M, Sliva C. (2011) Intrawound application of vancomycin for prophylaxis in instrumented thoracolumbar fusions: Efficacy, drug levels, and patient outcomes. Spine (Phila Pa 1976).36:2084-2088.
Publisher | Google Scholor - Molinari RW, Khera OA, Molinari 3rd WJ. (2012) Prophylactic intraoperative powdered vancomycin and postoperative deep spinal wound infection: 1,512 consecutive surgical cases over a 6-year period. Eur Spine J. 21 Suppl 4: S476-482.
Publisher | Google Scholor - Mariappan R, Manninen P, Massicotte EM, Bhatia A. (2013) Circulatory collapse after topical application of vancomycin powder during spine surgery. J Neurosurg Spine. 19:381-383.
Publisher | Google Scholor - Gans I, Dormans JP, Spiegel DA, Flynn JM, Sankar WN, Campbell RM, et al. (2013). Adjunctive vancomycin powder in pediatric spine surgery is safe. Spine (Phila Pa 1976). 38:1703-1707.
Publisher | Google Scholor














