

Case Report
Post-surgical Bleeding Disorders in Neuroblastomas Causes and Treatments
Department of Pediatric Surgery, Dona Estefania, Portugal.
*Corresponding Author: Antonio Gentil Martins, Department of Pediatric Surgery, Dona Estefânia, Portugal.
Citation: Antonio G Martins. (2023). Post-surgical Bleeding Disorders in Neuroblastomas Causes and Treatments, Journal of Clinical Research and Clinical Trials, BRS publishers. 2(2); DOI: 10.59657/2837-7184.brs.23.012
Copyright: © 2023 António Gentil Martins, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 30, 2023 | Accepted: July 17, 2023 | Published: July 24, 2023
Abstract
A patient is shown that has presented with a large abdominal neuroblastoma having had a laparotomy for tumor removal, followed by signs of low blood pressure, paleness, tachycardia, sweating and with wound oozing, after a few hours silent period, raising immediately the possibility of the need for an emergency re-laparotomy. This patient calls attention for the need to study pre-operatively the preoperative level of phospholipid antibodies as a possible cause for an autoimmune reaction to be delt with only medically and avoiding dangerous and unjustified surgery.
Keywords: neuroblastomas; retroperitoneal tumors; laparotomy; coagulation cascade
Introduction and Objectives
To call attention to bleeding of a non-surgical nature, appearing in the immediate post- operative period of major abdominal Neuroblastoma excision, thus helping to avoid dangerous and inappropriate laparotomies.
Material and Methods
Caucasian male, 15 months old, presented with a stage IV large abdominal Neuroblastoma, associated with multiple bone metastases. VMA was 19.4ug/mg creatinine, Ferritin was 36.8 ug/ml, NSE was 87,2 ug/ml and LDH was 6988, total proteins 6,9 gr/dl, Hg was 8.9gr/dl and Platelets 203.000 WBC 4.400. Preoperative coagulation studies were normal, with PT 100 percent, APTT25,8 sec and Fibrinogen 408 mg/dl. (Fig 1).
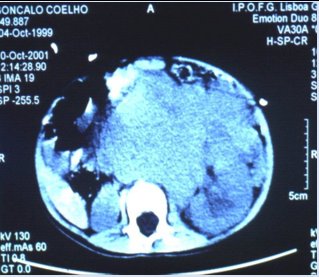
Figure 1: CT scan on diagnoses.
Therapy was started with Cyclo/Adria followed by VP16/CDDP, with disappearance of the metastatic lesions in the bones (fig 2) and marked reduction in the size of the tumor (fig 3).
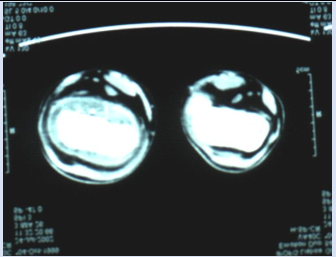
Figure 2: Metastases to the femur.
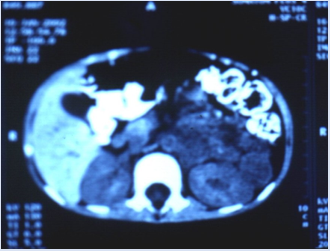
Figure 3: CT after chemotherapy.
On the 25thFebruary 2002, under endotracheal General Anesthesia, he was submitted to a left side transverse laparotomy, with extensive and laborious dissection for removal of the primary tumor, which reached the left adrenal and adhered markedly to the aorta, renal vein, left ureter (with partial obstruction and associated hydronephrosis) and other retroperitoneal structures, like muscles and the spine bones. Around 90% of the tumor was removed together with a large portion of the left mesocolon (but with preservation of the intestine) (fig 4).

Figure 4: tumor bed after resection, exposing the aorta. vena cava and renal pedicle.
The operated area looked so well and dry that, contrary to our routine, we did not even leave a rubber drain. At the end of surgery that lasted 3 hours his B.P. was 99/41 mmHg. Nevertheless, after a silent period of 4 to 5 hours that followed the end of surgery, he became pale and tachycardic, sweating, with blood oozing through the abdominal suture line, the blood pressure dropping to 61/29 mmHg.
New blood tests showed APTT to be above 2405 seconds and PT was43%, INR 3.30. IgM anti Beta 2 glycoprotein antibodies 9.2 MOL U/ml IgM anti cardiolipin antibodies 11.7 MPL U/nl, IgM anti-phospholipid antibodies 16.8 MPL U/ml, Hg 7.4g%, Platelets 235.000, Fibrinogen 2323 mg/dl.
Meanwhile he was transfused with packed cells, fresh frozen plasma, cryoprecipitate and vitamin K. recovering completely within the next 5 hours. At that time APTT had returned to normal, with a value of 38 seconds, and PT was already 78%. 24 hours later APTT was 22.4 sec, Pt 12.9 sec (95%) Fibrinogen 349 mg/dl, Hg 11.5 gr/dl Platelets 163.000 WBC 14.200.
N-myc was negative and there were no alterations in chromosome 1p32. There were no further postoperative problems. (Fig 5) Unfortunately, 8 months later, the Patient that had been kept on chemotherapy saw recurrence of the bone lesions and died.
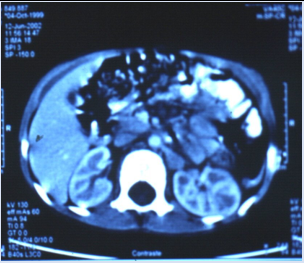
Figure 5: Post operative CT scan.
Discussion and Results
Coagulation studies are frequently abnormal in extensive and disseminated Neuroblastomas, but that did not happen in our Patient. Impending shock, soon after extensive abdominal surgery, always suggests the possibility of a bleeding vessel and often leads to re-laparotomy, particularly dangerous in the circumstances.
Neuroblastoma cells are rich in phospholipids and their disruption, by prolonged and extensive surgery, may lead to the production of antibodies. Through that autoimmune response (interaction between the antibody and the protein phospholipid complex) there may be interference with the coagulation cascade, resulting in non-surgical postoperative bleeding, as it seems to have happened in this Patient who had normal platelets and fibrinogen but moderately raised levels of antiphospholipid anticardiolipin and anti-Beta 2 glycoprotein antibodies.
In another Patient, previously treated and that showed a totally identical clinical picture and evolution (but with full early and late recovery), unfortunately, no antibodies studies were performed. It was his problem that prompted us to try to understand why the hemorrhagic situation had appeared, although certainly no final conclusions can be drawn from a single, although apparently proven, case
Conclusions
In this kind of patients, postoperative bleeding. after a silent period, may be due to non-surgical causes, what must be always kept in mind. Leaving abdominal drainage after surgery for 24 to 48 hours should always be done after extensive abdominal surgery, what might help in the differential diagnosis of the cause of the blood loss.
The study of phospholipid antibodies should now become a routine in the pre and postoperative evaluation of these Patients, and becomes even more important if postoperative bleeding occurs. Not delaying the mandatory active transfusion treatment, the possibility of a autoimmune reaction should certainly caution the Surgeon on the decision to re-open the abdomen. Only the study of future cases may tell if our hypothesis is correct and if prophylactic corticoids (in anticipation of an autoimmune response) or the administration of heparin, would be justified or even recommended.'
Funding: none
Consent: not required
Disclaimer: This Paper is a single authors piece and presents no conflict of interests.
References
- Macgregor A. R. (1962). Malignant disease in Infancy and Childhood Surgery of Childhood j.j: Mason Brown Edward Arnold (Publishers) Ltd, 20:543.
Publisher | Google Scholor - Maximiliano Salas M. Neoplasias Primarias do Sistema Nervoso Las Neoplasias de os ninos Maximiliano Salas M, 4:212
Publisher | Google Scholor - Graham A.G. (1973). Genitourinary System Surgery in Infancy and Childhood W.M.Dennison Churchill Livingstone, 16:327.
Publisher | Google Scholor - Grosfeld J.L. (1980). Rhabdomyosarcoma Pediatric Pediatric Surgery Holder and Ashcraft W.B. Saunders Company, 75:997.
Publisher | Google Scholor - Johnston J. H. (1969). Tumors of the genito-urinary tract and of the retroperitoneal tissues Neonatal Surgery P.P. Rickham and J.H.Johnston Butterworths, 48:591.
Publisher | Google Scholor - Pack G. T and Ariel I. (1959). Tumors of the Soft Somatic Tissues George T. Pack and Irving Ariel Little, Brown and Company, 17:411.
Publisher | Google Scholor - Wischuck L.E. (1980). Abominable masses and fluid Pediatric Surgery Holder and Hshcraft W.B.Saunders Company, 68.
Publisher | Google Scholor - Zacharias Zachariou. (2008). Pediatric Surgical Oncology Zacharias Zachariou Springer, 28:559.
Publisher | Google Scholor











