

Review article
Ponseti Method in the Management Equinovaro Clubfoot in Children with Arthrogryposis: Systematic Literature Review
- Bianca Gabriella de Oliveira 1*
- Leonardo Andrade Barreto de Almeida Silva 2
- Rafael Costa Dias 3
- Roberto Palma Costa Filho 4
- David Sadigursky 5
1Acadêmico de Medicina pela Universidade Salvador-UNIFACS, Salvador, BA, Brasil.
2Graduação em Medicina pelo Centro Universitario-UNIFACISA, Campina Grande, PB. Médico residente em Ortopedia e Traumatologia do Hospital Manoel Victorino, Salvador, BA.
3Graduação em Medicina pelo Centro Universitário Maurício de Nassau, Recife, Pernambuco. Médico residente em Ortopedia e Traumatologia do Hospital Manoel Victorino, Salvador, BA.
4Graduação em Medicina pela Universidade Salvador-UNIFACS, Salvador, BA. Médico Residente em Ortopedia e Traumatologia pelo Hospital Manoel Victorino, Salvador, BA.
5Mestre pela Universidade de São Paulo (USP) na especialidade de Cirurgia do Joelho. Membro Titular da Sociedade
*Corresponding Author: Bianca Gabriella de Oliveira, Acadêmico de Medicina pela Universidade Salvador-UNIFACS, Salvador, BA, Brasil.
Citation: Bianca G. Oliveira, L.A.B.A. Silva, Rafael C. Dias, R.P.C. Filho, Sadigursky D. (2024). Ponseti's Method in the Managemento Equinovaro Clubfoot in Children with Arthrogripose: Systematic Literature Review, Clinical Interventions and Clinical Trials, BioRes Scientia Publishers. 2(2):1-09. DOI: 10.59657/2993-1096.brs.24.016
Copyright: © 2024 Bianca Gabriella de Oliveira, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 12, 2024 | Accepted: February 26, 2024 | Published: March 09, 2024
Abstract
Clubfoot equinovarus in children with arthrogryposis multiplex congenita is a condition that is difficult to manage and that can commonly result in partial and/or total gait limitation. The aim of this study was to evaluate the use of the Ponseti method for the treatment of equinovarus clubfoot in children with arthrogryposis multiplex congenita. This is a systematic review of the literature carried out in the databases indexed in the Medical Literature Analysis and Retrieval System Online (MEDLINE) and Latin American and Caribbean Literature in Health Sciences (LILACS) carried out in accordance with the precepts established by the methodology PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). Six studies were selected for analysis that addressed the use of the Ponsenti method in the management of equinovarus clubfoot in children with arthrogryposis. The vast majority of feet treated with the Ponseti method showed a significant reduction in deformities, although the recurrence rate was also significant. It was a consensus among authors that arthrogrypotic foot is more complex for a conservative approach (Ponseti method) than idiopathic equinovarus foot. Faced with such complexity, the association of the technique with tenotomy of the Achilles tendon is observed as the preferred approach reported in the literature.
Keywords: equinovarus clubfoot; arthrogryposis; tenotomy; ponseti method
Introduction
The definition of congenital clubfoot (CTP) encompasses conditions in which there is a permanent and vicious attitude of the foot in relation to the leg, causing it to rest on the ground without adequate support points, with congenital or acquired causes. The equinovarus foot (EFP) is described as one of the most common forms of CTP, although there are also other presentations: talus-vertical foot, talus-valgus foot and metatarsus-varus foot. In order for a VFP to be defined, some specific anatomo-pathological alterations are expected, including adduction-supination of the forefoot, calcaneal varus, equinus, cavus, as well as skeletal alterations, among which the medial and plantar deviation of the anterior part of the talus stands out, with an angle formed between the long axis of the head-collar and the axis of the body of the talus between 115º and 135º (a normal value is considered to be between 150º and 155º). Most cases of PEV have no defined cause and are described as idiopathic. Among the well-defined causes are myelodysplasia and arthrogryposis. Arthrogryposis encompasses various disorders with multiple joint contractures and a heterogeneous presentation, including hip dislocations, deformities in the upper limbs, clubfeet, as well as alterations in the lower limbs, such as knees that can be pathologically flexed or extended [1]. Clubfoot in arthrogryposis tends to be rigid, with severe impairment, difficult correction and a high recurrence rat [2]. In cases of arthrogryposis multiplex congenita (AMC) and equinovarus clubfoot, there is greater tension on the posterior tibial artery, making it difficult to obtain sufficient dorsiflexion angles, even with subtalar release and other soft tissues [3].
Historically, arthrogryposis clubfoot has been managed surgically with extensive soft tissue releases; talectomy may be necessary, although a high occurrence of complications and high failure rates have been reported, leading to questions about the possibility of other surgical and non-surgical management of such cases [4]. The Ponseti method is characterized as a technique for manipulating clubfoot associated with the application of plaster casts keeping the foot in the initially corrected position. Before the final casting to achieve complete correction, most patients also receive a percutaneous tenotomy of the Achilles tendon. In order to reduce the recurrence of deformities, the use of a foot abduction orthosis is also recommended, with the orthosis persisting for 23 hours a day for three months, with its use being reduced to night time until the child is approximately five years old [5]. The Pirani score is a simplified classification system consisting of three variables in the hindfoot and three in the midfoot. An analysis is made of the clinical signs observed at each visit as changes in foot deformity occur, with a score of 0 for a limb without abnormality, 0.5 for slightly abnormal or 1 for severely abnormal. The foot score helps the doctor determine whether the deformity is being corrected properly and when Achilles tenotomy is indicated [6]. The use of the Ponseti method in idiopathic clubfoot is widely reported in the literature [6,3]. However, arthrogryposis feet tend to be more complex and have a greater chance of recurrence, which can limit the results obtained with this technique [7]. Given this context, this study aimed to analyze the use of the Ponseti method in patients with arthrogryposis and equinovarus clubfoot.
Materials and Methods
The study is characterized as a systematic literature review, structured according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), with a subsequent checklist for analyzing the results [8]. A four-phase flow diagram was used for the systematic analysis and selection of studies. The data search took place in February 2023 in the databases linked to the Medical Literature Analysis and Retrieval System Online (MEDLINE) and Latin American and Caribbean Health Sciences Literature (LILACS), using the SPICE strategy to identify the relevant studies [9].
Setting: patients with arthrogryposis and foot impairment
Perspective: individuals with arthrogryposis and clubfoot
Intervention: Ponseti method for correction of clubfoot
Comparison: Efficacy, complications, recurrence, subsequent surgical management
Evaluation: Rate or occurrence of clubfoot recurrence after the Ponsenti method in children with arthrogryposis.
The health science descriptors (DECS) / MESH TERMS were used in combination, according to the following structures:
Clubfoot AND Arthrogryposis
Clubfoot AND Ponseti method
Arthrogryposis AND Ponseti method
Inclusion and exclusion criteria
Studies meeting the following criteria were included: [1] studies with humans, age group < 18>
Once this stage was completed, the full texts of the articles were retrieved to analyze the other inclusion and exclusion criteria. Duplicate citations and studies not corresponding to the proposed review parameters were also excluded. Possible disagreements were resolved by discussion with a third reviewer, and inclusion was decided after consensus with the two main reviewers. In order to prioritize methodological quality, studies classified as "Good" after the NIH quality assessment were included, with studies with more than nine items ticked being considered suitable for inclusion. Epidemiological and demographic data was extracted using a Microsoft Excel spreadsheet, including parameters such as number of patients, age at onset of the Ponseti method, treatment strategies, relapses, complications and results. The systematic review protocol was registered with the International prospective register of systematic reviews (PROSPERO) under ID 395164 in order to improve the quality and suitability of the results to the proposed objectives.
Results
The screening process using the proposed DECS and respective Boolean Operators initially retrieved 119 studies. Subsequently, by excluding studies published more than ten years ago, 69 articles remained for analysis of the title. Twenty-nine studies were excluded because they were literature reviews and 27 studies were excluded because they did not use the Ponseti method in children with AMC, resulting in 13 studies for abstract analysis. After reading the abstracts, seven studies were excluded, giving a total of six studies for reading the full text and discussion. Three studies were excluded because they did not deal with children with clubfoot who had been diagnosed with arthrogryposis. Two studies were opinion articles and one study had duplicate records. Finally, six studies were selected for data extraction and discussion. Figure 1 shows the flowchart of the study selection process, as proposed by the PRISMA methodology adopted in this study.
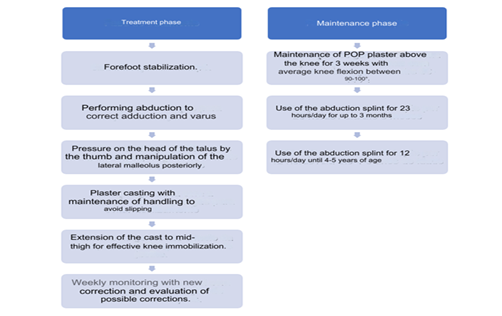
Figure 1: Flowchart described by the authors addressing the Ponseti method.
Source: Own elaboration (2023) based on data described in the literature.
The six studies included for analysis totaled 106 feet analyzed in terms of correction of clubfoot with the AMC condition, representing an average of 17.66±17.53 feet per study. The average age at the start of treatment was 2 years ± 2.3. Most of the studies reported improvement in deformities with the Ponseti method, although there was great variability in the rate of recurrence of such deformities. Recurrence rates of clubfoot ranging from 16.66 percentage to 87.5 percentage were reported in five studies.10,11 The average recurrence rate of the studies was 45.76 percentage ± 26.79 (p less then 0.005).
In all six studies selected for analysis, the Pirani score was used to monitor the correction of foot deformities, as described in the articles evaluated. Several authors have already stated that there is a high correlation between this score and the Ponsenti method, with a Pirani score of greeter then 4 commonly requiring at least four plaster casts, while a foot with a hindfoot score of 2.5-3 is more than 70 percentage likely to require a tenotomy, which would be performed when the midfoot score is less then 0.5.12,13. For the purposes of practical analysis, we considered total regression of deformities when Pirani's index was ≤ 0.5, thus observing a total correction rate of the feet analyzed of 27.44% ± 19.64 after the end of treatment. For this analysis, the feet that reached this rate were considered, regardless of whether or not there was a recurrence of the condition. Patients who did not show a regression of at least 1 point in the Pirani score were described as a failure of the method, and this situation was observed in an average of 30.55 percentage ±17.26 equinovarus feet of children with AMC. Table 1 shows the studies selected for analysis with a description of the variables considered. Three studies described isolated cases of children with clubfoot treated with the Ponseti method, including a total of 20 children/30 feet. Given the wealth of data described, we decided to carry out a comparative analysis (Table 2).
Table 1: Characterization of selected studies according to variables considered.
| Sharma et al.17 (2021) | Abraham et al.11 (2021) | Ayadi et al. (2015) | Matar et al.16 (2016) | Church et al.14 (2020) | Meseguer et al.10 (2021) | Média dos estudos | Valor – p | |
| Número de pés analisados | 7 | 8 | 12 | 17 | 56 | 6 | 17,66±17,53 | 0,03 |
| Idade média de início do tratamento (semanas) | 17,25±20,76 | 23 | 288 | 5 | 258±45,6 | 32,8 | 104±120,08 | 0,002 |
| Índice de reabilitação total no tratamento (Pirani ≤0,5) | 57,14% (4/7) | 37,5% (3/8) | 41,66% (5/12) | 17,64% (3/17) | 10,71% 3/28) | 0% (0/6) | 27,44%±19,64 | 0,03 |
| Índice de falha do tratamento | - | 62,5% (5/8) | 25% (3/12) | 17,64% (3/17) | 14,28% (4/28) | 33,33% (2/6) | 30,55%±17,26 | 0,002 |
| Recorrência | - | 87,5% (7/8) | 66,66% (8/12) | 29,41% (5/17) | 28,57% (16/28) | 16,66% (1/6) | 45,76%±26,79 | P<0> |
Source: Own elaboration according to data collected from the literature (2023).
Table 2: Analysis of individual cases described by the studies
| Autor | Criança | Idade de início do método Ponseti (semanas) | Método | Escore Pirani antes | Escore Pirani após | Recorrência |
| Sharma et al.17 2021 | 1 | 9 | Ponseti isolado | 5,5 e 1,5 | 1,5 e 0 | Não descrito |
| 2 | 4 | Ponseti + alongamento TA | 5,5 e 5 | 0,5 e 1 | Não descrito | |
| 3 | 3 | Ponseti + Tenotomia TA | 1,5 e 5,5 | 0,5 e 1,5 | Não descrito | |
| 4 | 53 | Ponseti + Tenotomia TA | 4 | 0,5 | Não descrito | |
| Meseguer et al.10 2021 | 5 | 92 | Ponseti isolado | 3,5 | 1 | Não |
| 6 | 8 | Ponseti + Tenotomia TA | 5,5 | 1,5 | Sim | |
| 7 | 1 | Ponseti isolado | 4 | 1,5 | Não | |
| 8 | 624 (13 anos) | Ponseti + Tenotomia TA | 6 | 1,5 | Não | |
| 9 | 12 | Ponseti + Tenotomia TA | 6 | 1 | Não | |
| 10 | 51 (1 ano) | Ponseti + Tenotomia TA | 6 | 1 | Não | |
| Matar et al.16 2016 | 11 | 20 | Ponseti isolado | 3 | 0,5 | Não |
| 12 | 6 | Ponseti + Tenotomia TA | 5 | 1,5 | Sim | |
| 13 | 3 | Ponseti + Tenotomia TA | 5 e 5,5 | 1 e 0,5 | Não | |
| 14 | 6 | Ponseti + Tenotomia TA | 5 e 5 | 1,5 e 0,5 | Não | |
| 15 | 2 | Ponseti + Tenotomia TA | 6 | 1 | Não | |
| 16 | 3 | Ponseti + Tenotomia TA | 6 e 6 | 1 e 1 | Não | |
| 17 | 6 | Ponseti + Tenotomia TA | 5,5 e 5,5 | 1 e 1,5 | Sim | |
| 18 | 5 | Ponseti + Tenotomia TA | 6 e 6 | 6 e 6 | Sim | |
| 19 | 3 | Ponseti + Tenotomia TA | 6 e 6 | 6 e 6 | Sim | |
| 20 | 4 | Ponseti + Tenotomia TA | 6 e 6 | 6 e 6 | Sim |
Source: Own elaboration according to data collected from the literature (2023).
Considering the 20 cases presented, the Ponseti method was started at an average age of 45.75 weeks ± 134.58, with a predominance of treatment starts in the first two years of life. Of all the children individually assessed (n=20/30 feet), the Ponseti method alone was used in 4 cases/5 feet (20%), the Ponseti method associated with stretching the Achilles tendon was used in 1 child/2 feet (5 percentage ) and in 75 percentag of the cases the Ponseti method associated with TA tenotomy was used (n=15/23 feet). Four studies (n=4/8 feet) did not address the recurrence of clubfoot, in 10 feet (33.33 percentag) recurrence was reported and non-recurrence was described in 14 feet (46.66 percentage ) (Table 2). The mean initial Pirani score in the 30 feet included was 5.1 ±1.24. The final Pirani score was 2.03 ± 2.07, showing that there was a reduction in the degree of deformity in the feet treated with the Ponseti method. A total of 7 feet (23.33 percentag) obtained a final Pirani score ≤ 0.5, which was considered by the studies to be a complete reduction in deformities. In six feet, the Pirani score remained equal to six, representing a failure of the method in the approach to clubfoot. In all cases, the approach was a combination of the Ponseti method associated with Achilles tendon tenotomy and the patients were less than six months old (Table 2).
Discussion
The Ponseti method used in the selected studies includes two phases, the first being treatment and the second maintenance. The treatment phase involves manipulating the foot and correcting deformities simultaneously and sequentially (Figure 1) [11,12,14,15,16,17,18]. The study by Sharma et al. (2021) included 85 children with clubfoot. Four patients (3.70%) were diagnosed with arthrogryposis multiplex congenita (AMC), including a total of 7 affected feet. The authors carried out a minimum follow-up of 52 weeks, using the Pirani score for evaluation before and after treatment. Only one of the patients with MCA underwent the Ponseti method exclusively, with an initial score of 5.5 and 1.5 in the feet and a reduction to 1.5 in the first foot and total correction in the second foot (Pirani score 0.5). In the other three children, the Ponseti method associated with Achilles tendon lengthening (n=1; 2 feet) or Achilles tendon tenotomy (AT) was performed, including five feet and with complete correction in 3 feet, and partial correction in two feet (post-treatment Pirani score of 1 and 1.5 respectively [17]. The study by Abraham et al. (2021) included six patients with AMC (8 feet) who underwent treatment with the Ponseti method before the age of two. Recurrence of clubfoot in AMC was 87.5% (7/8 feet). The average follow-up was 39.2 months (range 12 to 147 months), with an average initial treatment age of 23 weeks (range 2 to 62 weeks). The average number of releases was 4.7 per foot for initial correction (range 1 to 9). All patients underwent tenotomy [11].
High recurrence of clubfoot in children with AMC after treatment with the Ponseti method was also reported by Ayadi et al. (2015) in which out of a total of 12 feet treated there was recurrence in 8 cases (66.66 percentage), however, the authors report that all patients had a reduction in deformities after the method and there was no total recurrence, but partial recurrence of deformities [18]. Although the recurrence of clubfoot is widely reported in the literature in cases of AMC, in the study by Meseguer et al. (2021) the authors described six cases of children and adolescents with this condition who underwent the Ponseti method with or without an Achilles tendon tenotomy, representing a recurrence rate of 16.66 percentage, much lower than that previously reported [10]. In the study presented by Church et al. (2020), the authors reported the need for tenotomy in 85 percentage of children with AMC (23/28) associated with the Ponseti method, 19 percentage of whom required more than one tenotomy (5/28) All the children with AMC included in the study (n=28) had residual deformity in range of motion, especially in dorsiflexion and plantar flexion. Eight children (35 percentage) required repeated lengthening of the Achilles tendon, three children required transfer of the anterior tibial tendon (12percentage), two children required release of the plantar fascia (8 percentage) and one child required triple arthrodesis [14]. The combination of the Ponseti method and Achilles tendon tenotomy was used in 94.1 percentage (16/17) of the patients with MCA included in the study by Matar et al. (2016), and initial correction was achieved in all children with an average of 8 (range 4-10) Ponseti casts. Three patients with severe, bilateral deformities (6/17, 35.3 percentage) failed treatment with Ponseti, despite the initial correction [16].
Final Considerations
Six studies were selected for analysis that addressed the use of the Ponsenti method in the management of clubfoot in children with arthrogryposis. There was a consensus among the authors that arthrogryposis feet are more complex to treat conservatively (Ponsenti method) than idiopathic equinovarus feet. The vast majority of feet treated with the Ponseti method showed a significant reduction in deformities, although the recurrence rate was also significant.
Faced with such complexity, the association of the technique with Achilles tendon tenotomy as the preferred approach reported in the literature, with a reduction in recurrence rates. Isolated interventions with the Ponseti method have also been described, as well as this method associated with stretching the Achilles tendon.
Declarations
Conflict of Interest
The authors declare no conflict of interest.
Financial Support
This research did not receive any specific funding from public, commercial or non-profit sector funding agencies
References
- Bevan WP, Hall JG, (2007). Bamshad M, Staheli LT, Jaffe KM, Song K. Arthrogryposis multiplex congenita (amyoplasia): an orthopaedic perspective. J Pediatr Orthop, 27(5):594-600
Publisher | Google Scholor - Guidera KJ, Drennan JC. (1985). Foot and ankle deformities in arthrogryposis multiplex congenita. Clin Orthop Relat Res, (194):93-98
Publisher | Google Scholor - Kowalczyk B, Lejman T. (2008). Short-term experience with Ponseti casting and the Achilles tenotomy method for clubfeet treatment in arthrogryposis multiplex congenita. J Child Orthop, 2(5):365-371
Publisher | Google Scholor - Machida J, Inaba Y, Nakamura N. (2017). Management of foot deformity in children. J Orthop Sci, 22(2):175-183
Publisher | Google Scholor - Dietz FR, Noonan K. (2016). Treatment of Clubfoot Using the Ponseti Method. JBJS Essent Surg Tech, 6(3):28
Publisher | Google Scholor - Boehm S, Limpaphayom N, Alaee F, Sinclair MF, Dobbs MB. (2008). Early results of the Ponseti method for the treatment of clubfoot in distal arthrogryposis. J Bone Joint Surg Am, 90(7):1501-1507
Publisher | Google Scholor - Simis SD, Fucs PMB. (2008). O tratamento do pé artrogripótico. Rev Bras Ortop, 43(5):151-156
Publisher | Google Scholor - Liberati A, Altman DG, Tetzlaff J, et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med, 6(7):1000100
Publisher | Google Scholor - Booth A. (2016). Searching for qualitative research for inclusion in systematic reviews: a structured methodological review. Syst Rev, 5:74
Publisher | Google Scholor - Ferrando Meseguer E, Roig Sánchez S, Pino Almero L, Romano Bataller A, Mínguez Rey MF. (2021). Syndromic clubfoot beyond arthrogryposis and myelomeningocele: orthopedic treatment with Ponseti method. Pie zambo sindrómico más allá de la artrogriposis y el mielomeningocele: tratamiento ortopédico con el método de Ponseti. Rev Esp Cir Ortop Traumatol (Engl Ed), 65(3):180-185
Publisher | Google Scholor - Abraham J, Wall JC Jr, Diab M, Beaver C. (2021). Ponseti Casting vs. Soft Tissue Release for the Initial Treatment of Non-idiopathic Clubfoot. Front Surg, 8:668334
Publisher | Google Scholor - Agarwal A, Gupta N. (2014). Does initial Pirani score and age influence number of Ponseti casts in children? Int Orthop, 38(3):569-572
Publisher | Google Scholor - Hussain FN. (2007). The role of the Pirani scoring system in the management of club foot by the Ponseti method. J Bone Joint Surg Br, 89(4):561-562
Publisher | Google Scholor - Church C, McGowan A, Henley J, et al. (2020). The 5-Year Outcome of the Ponseti Method in Children with Idiopathic Clubfoot and Arthrogryposis. J Pediatr Orthop, 40(7):641-646
Publisher | Google Scholor - Maranho DA, Volpon JB. (2011). Congenital Clubfoot. Acta Ortop Bras, 19(3):163-169
Publisher | Google Scholor - Matar HE, Beirne P, Garg N. (2016). The effectiveness of the Ponseti method for treating clubfoot associated with arthrogryposis: up to 8 years follow-up. J Child Orthop, 10(1):15-18.
Publisher | Google Scholor - Sharma PK, Verma V, Meena S, Singh R, Km P. (2021). Comparative evaluation and analysis of outcomes in non-idiopathic and idiopathic clubfeet with Ponseti method at a tertiary care centre of a developing country. Foot (Edinb), 49:101841
Publisher | Google Scholor - Ayadi K, Trigui M, Abid A, Cheniour A, Zribi M. et.al. (2015). [Arthrogryposis: clinical manifestations and management]. Arch Pediatr, 22(8):830-839.
Publisher | Google Scholor














