

Case Report
Perforated Meckel’s Diverticulum Causing Acute Abdomen-A Rare Case
1Jr Resident Department of General Surgery (3RD year), Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences, Sawangi, Wardha, Maharashtra, India.
2Professor and Head of Unit Department of General Surgery, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences, Sawangi, Wardha, Maharashtra, India.
3Jr Resident Department of General Surgery, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences, Sawangi, Wardha, Maharashtra, India.
4final mbbs student, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences, Sawangi, Wardha, Maharashtra, India.
*Corresponding Author: Anil Reddy Cherukula, Jr Resident Department of General Surgery (3RD year), Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences, Sawangi, Wardha, Maharashtra, India.
Citation: Anil R. Cherukula, Suhas N. Jajoo, Garima Saxena G, Harshita J. (2024). Perforated Meckel’s Diverticulum Causing Acute Abdomen- A Rare Case. Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers. 3(1):1-5. DOI: 10.59657/2992-9989.brs.24.022
Copyright: © 2024 Anil Reddy Cherukula, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 07, 2024 | Accepted: March 19, 2024 | Published: March 23, 2024
Abstract
One of the most prevalent congenital gastrointestinal anomalies is Meckel's Diverticulum. A Meckel's Diverticulum presents with hemorrhage, inflammation and obstruction as its most common consequences. Its perforation on its own is quite rare, which is similar to acute appendicitis in presentation. In addition to hemorrhage and intestinal obstruction, perforation, intussusception, volvulus, and malignant transformation are some of its other consequences. Due to the possibility of non-specific presenting symptoms and the difficulty of making a differential diagnosis in children and adults, the preoperative diagnosis of MD can be time- and cost-intensive. We present a case of a 14-year-old boy who developed perforation in Meckel's Diverticulum with pyoperitonitis, a rare condition.
Keywords: meckel’s diverticulum; acute abdomen; hemorrhage; inflammation; obstruction
Introduction
Meckel's Diverticulum (MD) was first described in 1808. It is caused by partial destruction of the proximal-most component of the vitelline duct (also known as the omphalomesenteric duct) during the first 5 to 7 weeks of pregnancy. The ileum's antimesenteric boundary produces this embryonic remnant. It is a frequent small intestine aberration that affects about 2% of the population and is typically fatal. It was discovered by chance at the time of abdominal examination [1,2]. Bleeding and intussusception are common side effects.
In contrast, the second most frequent complication of it is intestinal obstruction. Intussusception, small bowel volvulus attached to the anterior abdominal wall, axial torsion of Meckel's Diverticulum, and Littre's hernia are some potential causes of this [3]. Meckel's Diverticulum is a true diverticulum since the layers of a healthy intestine, and all of the diverticula's contents are contained within the walls of these lesions. It is usually within 100 cm of the ileocecal valve in the ileum. Over 60% of the heterotopic mucosa in MD is stomach mucosa [4]. Other complications include hemorrhage, chronic peptic ulceration, and perforation, which are caused by pancreatic mucosa in most cases. A well-known "rule of twos" also applies, which states that the anomaly affects 2% of the population, is usually located within 2 feet of the ileocecal valve, and is around 2 inches long [5]. It is most commonly seen under two years of age. Meckel's diverticulum is a congenital anomaly found in approximately 2% of the general population. Complications like perforation and peritonitis develop in only 4% of patients with this malformation [6].
Case Presentation
We present a case of a 14-year-old boy who had severe abdominal discomfort for three days, primarily in the right iliac fossa, with two episodes of bilious vomiting for two days and constipation for two days. He also complained of fever for one day. He had no history of other congenital anomalies like Crohn's disease or cardiovascular or neurological abnormalities. He had no history of any previous surgeries. On examination, the patient was afebrile. The pulse was 126 beats per minute. The peripheral pulsations were palpable. Blood pressure was 100/60 mm of Hg and the respiratory rate was 28 breaths per minute. There was no pallor, icterus, cyanosis, clubbing, edema or lymphadenopathy. Cardiovascular, respiratory and central nervous system examinations were within normal limits. Blood investigations revealed Total Leucocyte count (TLC) to be 11,000 cu.mm and C- Reactive Protein (CRP) to be 0.6 mg/dl, which were within normal limits. On inspection, the abdomen was distended, the umbilicus was in the midline, and no previous scars were visible. No engorged veins, no visible masses, and no peristalsis were seen. On palpation, there was tenderness and rigidity were present all over the abdomen. On percussion, a tympanic note was heard all over the abdomen. There was no fluid thrill, and obliteration of liver dullness was present. On auscultation, bowel sounds were absent. Based on the history and the clinical examination, a provisional diagnosis of intestinal perforation, appendicular perforation, perforation of Meckel's Diverticulum, perforation peritonitis, acute appendicitis, and intussusception was made.
Further, to come to a final diagnosis, investigations were done. On an erect x-ray abdomen, there was evidence of pneumoperitoneum with air outlining the bowel wall. Abdominal ultrasonography showed free fluid in the abdomen. CT (Computed Tomography) abdomen was suggestive of perforated Meckel’s Diverticulum (Figure 1). It also suggested pneumoperitoneum with small air pockets at the gall bladder fossa. In addition, there was fat stranded at the duodenum and free fluid in the pelvis. There was no associated bowel inflammation, peptic ulcer, or duplication cyst with the ectopic gastric mucosa on CT scan. An emergency exploratory laparotomy was performed on the patient.
Intraoperative findings
At the antimesenteric border, a 5 x 5 cm perforated Meckel's Diverticulum was seen 60 cm from the ileocaecal junction. Another 0.5 x 1 cm perforation over the base of Meckel's Diverticulum was present (Figure 2). Pus was seen all over the peritoneal cavity (500 ml of pus was drained), and the rest of the intestine and organs were regular.
It was a class 4 type of wound for which, ideally, an ileostomy should have been done, but the patient's relatives denied consent. Hence, primary closure was planned. The pyoperitoneum was evacuated along with the excision of the perforated Meckel's Diverticulum, an end-to-end ileal anastomosis was done (Figure 3). The perforation was closed with a mersilk suture. After putting a right subhepatic drain and a left pelvic drain, the peritoneum was closed with proline loop sutures. Subsequently, the abdomen was closed in layers with mattress sutures using vicryl and ethilon. On histopathology, the diverticulitis mucosa was heterotopic, supporting the diagnosis. The patient had no complications after surgery and was discharged from the hospital. USG abdomen and pelvis was done on follow-up after a month and were normal.

Figure 1: CT abdomen showing Perforated Meckel’s Diverticulum

Figure 2: Perforation at the Base of Meckel’s Diverticulum
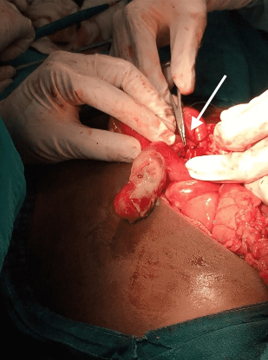
Figure 3: Sutured Perforation of Meckel’s Diverticulum
Discussion
About 2% of the population has Meckel's Diverticulum, a congenital condition. Unfortunately, 4% of children with this abnormality develop complications, with most instances presenting in childhood [6]. In addition to haemorrhage and intestinal blockage, perforation, intussusception, volvulus, and malignant transformation are some significant consequences [8]. The preoperative diagnosis of MD can be time- and money-consuming due to the possibility of non-specific presenting symptoms and the difficulty of making a differential diagnosis in children and adults. usually, the ileostomy is done for patients presenting with perforation of MD, but here due to conscent-related issues, we have done end-to-end ileal anastomosis. Here, we present a challenging and unusual case of perforated Meckel’s diverticulum managed without ileostomy.
A laparotomy is necessary for a conclusive diagnosis and treatment if a patient with MD presents with an acute abdomen. Most MD patients remain asymptomatic for the remainder of their lives; complications are rare [8]. The holes in Meckel's rings, known as Meckel's perforations, might resemble acute appendicitis and present as an acute abdomen [9]. A foreign body irritates the diverticulum wall and generates pressure necrosis or spontaneous perforation due to progressing diverticulosis are the leading causes of MD perforation. After blunt abdominal trauma, MD wall inflammation and perforation are highly uncommon events [10]. It might be challenging to diagnose a complex MD with a preoperative assessment of the overlapping clinical and imaging findings since other acute surgical and inflammatory illnesses of the abdomen also show comparable symptoms.
Conversely, an accurate diagnosis will result in the more effective use of laparoscopic surgery to treat it [11]. Most MD patients remain undiagnosed for the whole of their lives, and only by accident may they be discovered during surgery, an autopsy, or during gastrointestinal examination [12,13]. On a CT scan, MD shows up as a fluid- or air-filled blind-ending pouch. The antimesenteric side of the distal ileum is where the pouch develops. On a CT scan, most individuals with inflammatory MD can be found [14,15]. Diagnosing MD via a CT scan has improved thanks to new technology. The internal organ planes can be seen owing to the capabilities of the most current MDCT (Multidetector Computed Tomography) scanners.
Less than 10% of symptomatic MDs receive a preoperative diagnosis. The most frequent manifestations associated with symptomatic or complex MD are intestinal obstruction, diverticulitis, intussusceptions, and tumour [16]. Diverticulitis rates are not known with certainty [17,18]. A significant problem that frequently results from diverticulitis is gangrene. Lymphatic perforation, Littre's hernia, cancers like leiomyosarcoma, and stromal tumours with weak differentiation are a few more conditions [19]. A review found that foreign body penetration into MD is relatively uncommon and that the resection rate due to foreign body penetration is relatively low. Alternatively, diagnosing an asymptomatic or complicated MD based on the patient's medical history, physical examination, lab results, and imaging could be difficult.
Conclusion
Our report exhibits a rare case of perforation of Meckel's Diverticulum, which led to peritonitis. It may carry a higher risk of unfavourable outcomes. So, treating it is very crucial. In this case, the gastric mucosa inside Meckel's Diverticulum led to perforation and eventually caused peritonitis, presenting us with an acute abdomen. A pathologic MD is challenging to diagnose; and it is not always easy to make a preoperative diagnosis. A complex Meckel's Diverticulum diagnosed late can result in substantial morbidity and mortality, and to avoid bowel strangulation and gangrene, exploration should be performed as early as possible. MD should be included in the differential diagnosis of individuals who report small intestinal obstruction. So, we can also recommend Meckel's diverticulectomy and end-to-end ileal anastomosis in cases with acute abdomen having perforation of Meckel's Diverticulum.
References
- Ding Y, Zhou Y, Ji Zh, et al. (2012). Laparoscopic Management of Perforated Meckel's Diverticulum in Adults. Int J Med Sci, 3:243-247.
Publisher | Google Scholor - Dimitriou I, Evaggelou N, Tavaki E, et al. (2013). Perforation of Meckel's diverticulum by a fish bone presenting as acute appendicitis: A case report. J Med Case Rep, 7:231.
Publisher | Google Scholor - Sharma RK, Jain VK. (2008). Emergency surgery for Meckel's diverticulum. World J Emerg Surg, 3:27.
Publisher | Google Scholor - Dumper J, Mackenzie S, Mitchell P, et al. (2006). Complications of Meckel's diverticula in adults. Can J Surg, 49:353-357.
Publisher | Google Scholor - Camelo R, Santos P, Mateus Marques R. (2019). Perforated Meckel's Diverticulum in an Adult. GE Port J Gastroenterol, 26:285-289.
Publisher | Google Scholor - Bemelman WA, Hugenholtz E, Heij HA, et al. (1995). Meckel's diverticulum in Amsterdam: experience in 136 patients. World J Surg, 5:734-736.
Publisher | Google Scholor - Platon A, Gervaz P, Becker CD, Morel P, Poletti P-A. (2010). Computed tomography of complicated Meckel’s diverticulum in adults: a pictorial review. Insights Imaging, 1:53-61.
Publisher | Google Scholor - Park JJ, Wolff BG, Tollefson MK, et al. (2005). Meckel diverticulum: the Mayo Clinic experience with 1476 patients (1950-2002). Ann Surg, 241:529-533.
Publisher | Google Scholor - Bani-Hani KE, Shatnawi NJ. (2004). Meckel's diverticulum: comparison of incidental and symptomatic cases. World J Surg, 28:917-20.
Publisher | Google Scholor - Ekwunife CN, Mbadugha TN, Ogbue UN. (2014). Isolated Meckel's diverticulum perforation as a sequel to blunt abdominal trauma: a case report. J Med Case Rep, 8:111.
Publisher | Google Scholor - Kloss BT, Broton CE, Sullivan AM. (2010). Perforated Meckel diverticulum. Int J Emerg Med, 3:455-457.
Publisher | Google Scholor - Levy AD, Hobbs CM. (2004). From the archives of the AFIP. Meckel diverticulum: radiologic features with pathologic Correlation. Radiographics, 24:565-587.
Publisher | Google Scholor - Rossi P, Gourtsoyiannis N, Bezzi M, et al. (1996). Meckel's diverticulum: imaging diagnosis. AJR Am J Roentgenol, 166:567-573.
Publisher | Google Scholor - Sancar S, Demirci H, Sayan A, et al. (2015). Meckel's diverticulum: Ten years' experience. Ulus Cerrahi Derg, 31:65-67.
Publisher | Google Scholor - Yahchouchy EK, Marano AF, Etienne JC, et al. (2001). Meckel's diverticulum. J Am Coll Surg, 192:658-662.
Publisher | Google Scholor - Ferguson H, Soumian S, Dmitrewski J. (2010). Perforation of Meckel’s diverticulum secondary to a large faecolith. BMJ Case Rep, 2010:2308.
Publisher | Google Scholor - Kusumoto H, Yoshida M, Takahashi I, et al. (1992). Complications and diagnosis of Meckel’s diverticulum in 776 patients. Am J Surg, 164:382-383.
Publisher | Google Scholor - Hager M, Maier H, Eberwein M, et al. (2005). Perforated Meckel’s diverticulum presenting as a gastrointestinal stromal tumor: a case report. J Gastrointest Surg, 9:809-811.
Publisher | Google Scholor - Yagcı G, Cetiner S, Tufan T. (2004). Perforation of Meckel’s diverticulum by a chicken bone, a rare complication: report of a case. Surg Today, 34:606-608.
Publisher | Google Scholor












