

Research Article
Pattern and Management Outcome of Acute Abdomen and Review of the Role of Task Shifting-Task Sharing in Leku General Hospital, Sidama, Ethiopia
1Leku general hospital, sidama, Ethiopia
2Aleta wondo primary hospital, sidama, Ethiopia.
3Dore bafano primary hospital, sidama, Ethiopia.
*Corresponding Author: Asfaw Kibret, Leku general hospital, sidama, Ethiopia.
Citation: Kibret A, Lema C, Assefa T, Gebeyehu N, Bayelign. (2024). Pattern and Management Outcome of Acute Abdomen and Review of the Role of Task Shifting-Task Sharing in Leku General Hospital, Sidama, Ethiopia. Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers. 3(2):1-9. DOI: 10.59657/2992-9989.brs.24.026
Copyright: © 2024 Asfaw Kibret, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 15, 2024 | Accepted: May 13, 2024 | Published: May 24, 2024
Abstract
Background: acute abdomen is one of the surgical emergencies of abdominal disease presented with sudden onset abdominal pain and often needs urgent surgical interventions. Its pattern varies worldwide. In low-income countries like Ethiopia the surgical workforce is still unmet but strategies like the integrated emergency surgery program was one of the successful tasks shifting and task sharing strategy which saved the life of many which need emergency surgical intervention.
Objective: the aim of this study was to assess the pattern, outcome of management of non-traumatic acute abdomens and the role of task shifting in leku general hospital, Sidama, Ethiopia.
Methods: this was a three years retrospective cross-sectional study conducted at Leku general hospital in sidama region southern part of Ethiopia. The study populations were patients operated in the Leku general hospital for diagnosis of non-traumatic acute abdomen from august 2021 GC to august 2023Gc.Data were collected by checklists and analyzed by SPSS descriptive statistics.
Result: in the study period it was found 225 operated cases for indication of non-traumatic acute abdomen. Majority of the cases were male (161) and 64 were female making male to female ratio 2.5 :1. The age ranges from 4yrs to 80 years. Majority of the cases fall in the 2nd and 3rd decades of age. Most of them were rural dwellers. Most patients arrived after 24hrs of pain. The most frequent acute abdominal case in Leku general hospital found in the study was appendicitis (46.2%) followed by bowel obstruction (34.2%). Small bowel volvulus was the common cause for small bowel obstruction Most of the acute abdomen cases (84.9%) were operated by integrated emergency surgery professionals (IESO). From the 88 bowel related emergency operations 47% of them needed resection and anastomosis. The mortality rate in the study was found 2.2%.
Conclusion: The leading cause of acute abdomen was found appendicitis. Majority of the cases were operated by IESO and their role were remarkable in this general emergency surgery interventions. The fatality rate was 2.2% this was lower than other studies in the country.
Keywords: acute abdomen; appendicitis; small bowel volvulus; task-shifting
Introduction
Acute abdomen is one of the surgical emergencies presented with sudden onset of abdominal pain and often needs immediate operative intervention. The causes of the acute abdomen are several and their relative incidence varies in different populations. Worldwide, appendicitis, bowel obstructions, hernias of different emergency entities and volvulus remain the most common causes of acute abdomen in adults. Intestinal obstruction has been the leading cause of acute abdomen in several African countries whereas acute appendicitis is the most frequently seen cause in the developed world. The leading causes of intestinal obstruction in Africa have mostly been hernia and volvulus whereas adhesions are most frequent in the developed world [1,4].
Analysis based on specific cause of acute abdomen is of great value for early diagnosis and prompt treatment in clinical practice of surgery. Even if the pattern changes overtime, assessing the local epidemiology is helpful. It has epidemiological and clinical benefits. Patients with acute abdomen in Africa countries present late due to factors categorized as patients’ factors and institutional inadequacies. Efforts to reduce delay may reduce complications. Surgery is often the only solution to prevent death from surgical cause of acute abdomen. As the global community increasingly recognizes the large and unmet burden of surgical disease, a new emphasis is being placed on strengthening the health system at the first-level hospital. The shortage of surgical care providers at this district and rural level can be met by surgical task-shifting/sharing to non-physician clinicians [15].
The Ministry of Health of Ethiopia, in collaboration with universities and development partners, has taken the initiative to train non-doctor health professionals in emergency obstetrics and general surgery in 2006. This innovative program has got the attention of several partners. However, since this program was the first of its kind in the world (training health officers with a Bachelor of Science Degree to Master's Degree level), several professionals (particularly surgeons) were questioning the graduate’s capacity to handle emergency surgical problems in the rural setting, where surgeons and obstetricians are inaccessible. The back-and-forth discussion with stakeholders had delayed the initiation of the program by about three years. Then after the deployment of the first batch of this professionals in 2009 GC, they are serving the unreached community in most rural part of Ethiopia and few in the main cities [16].
Materials and Methods
Study area
The study was conducted at Leku general hospital, which is located in sidama region, southern part of Ethiopia,27km from the region capital, Hawasa and 250 km from Adis Abeba which is the capital city of the country.
Study design and period
The retrospective cross-sectional study design was used. Data of patients with cases of acute abdomen (non-traumatic, non-obstetrics and non-gynecologic) managed surgically in Leku general hospital from August 1,2021 to August 1,2023 Gc.
Participates
The study participants were all emergency general surgery patients operated for diagnosis of non-traumatic acute abdomen in Leku general hospital during the study period.
Data were entered into SPSS version 20 statistical software packages for data analysis. Computer frequencies and summary statistics (such as mean, percentage, etc.) were used to describe the study population in relation to relevant variables.
Results
In the study period there were 225 patients underwent emergency abdominal surgery in the like general hospital for non-traumatic, non-obstetrics and non-gynecologic indication of acute abdomen. Of these 71.6 % (161) were male and 28.4 % (64) female patients making male to female ratio 2.5:1. Among the patients 150 (66.7%) patients were rural and 75(33.3%) urban dwellers. The age ranges from 4yrs up to 80yrs with the mean age of 28.26 ± 16.5yrs (table 1).
Table 1: socio-demographic characterstics of patients with non-traumatic acute abdominal cases at LGH from august 2021-august 2023 GC.
| Socio-demographic variables(n=225) | frequency | percent |
| Age | ||
| <10> | 32 | 14.2 |
| 11-20 | 57 | 25.3 |
| 21-30 | 64 | 28.4 |
| 31-40 | 31 | 13.8 |
| 41-50 | 19 | 8.4 |
| 51-60 | 13 | 5.8 |
| >60 | 9 | 4 |
| Sex | ||
| Male | 161 | 71.6 |
| Female | 64 | 28.4 |
| Residence | ||
| urban | 75 | 33.3 |
| rural | 150 | 66.7 |
Only 27% of pts presented within 24hrs of complain and most patients (41.8) came after 24hrs and before 48hrs of disease duration. Almost 31.1% patients came late after 48hrs of pain. (fig.1).
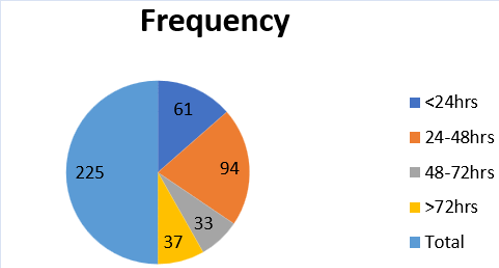
Figure 1: duration of presentation of acute abdomen patients at LGH, August 2021-2023
The major causes of acute abdomen in this study was found to be acute appendicitis 104(46.2%) followed by intestinal obstruction (small and large bowel obstruction) 77(34.2%).There were 26(11.6%) cases of peritonitis not due to gangrenous bowel obstructions of which there were 17(7.6%) patients were due to perforated appendicitis who developed generalized peritonitis and 8(3.6%) pts were cases of perforated peptic ulcer disease (PPUD).There was one patient who developed peritonitis due to typhoid perforation(fig 2). From the 77 intestinal obstruction cases,60(77.9%) cases were due to small bowel obstruction,17(22.1%) were due to large bowel obstructions. In this study the most common causes of small bowel obstruction were small bowel volvulus 37(61.7%), post operative adhesion and band 12(20%) and the common causes for large bowel obstruction was sigmoid volvulus 9(52.9%) and cecal volvulus 4(23.5%). Among 88 bowel related surgeries including obstruction, hernia, intussusceptions 47.7% were non-viable bowels which needed resection (table 2). In the study period among the 225 operated acute abdomen cases 191(84.9%) cases were operated by IESO surgeon on duty.15 (6.7%) cases were operated by general surgeon with the IESO surgeon on duty.19 (8.4%) cases were operated by the general surgeon solely. (table 3). Nine patients developed post operative complications. Among the complications 5 of it was wound infections,there were 2 patients with anastomotic leak.Five patients died after operation in the ward making the mortality rate 2.2% during the study period.(fig 3).
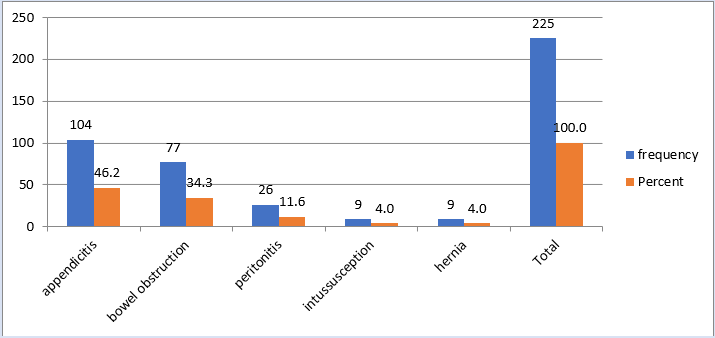
Figure 2: frequency of causes of acute abdomen at LGH,August 2021-2023
Table 2: specific causes of intestinal obstructions at LGH, August 2021-2023
| Causes of SBO | No of cases | % From SBO | %from total obstruction |
| Small bowel volvulus | 37 | 61.7 | 48.05 |
| Adhesion and band | 12 | 20 | 15.6 |
| Intussusception | 3 | 5 | 3.9 |
| Ascaris bolus | 3 | 5 | 3.9 |
| hernia | 3 | 5 | 3.9 |
| Bowel mass | 1 | 1.6 | 1.3 |
| Ileoileal knotting | 1 | 1.6 | 1.3 |
| Causes of LBO | No of cases | % From LBO | % from total obstruction |
| Sigmoid volvulus | 9 | 52.9 | 11.7 |
| Ileosigmoid knotting | 4 | 23.5 | 5.2 |
| Cecal volvulus | 3 | 17.6 | 3.9 |
| Bowel mass | 1 | 5.8 | 1.3 |
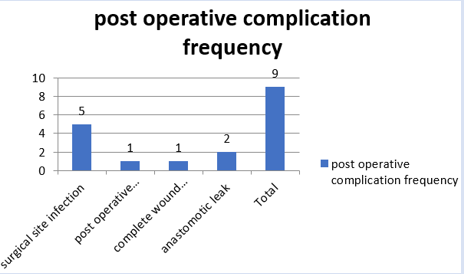
Figure 3: post operative complication
Table 3: summary cross tabulation of procedure done with the clinician type.
| procedure done * procedure done by Cross tabulation | |||||
| procedure done by | Total | ||||
| IESO only | IESO+general surgeon | general surgeon only | |||
| procedure done | appendectomy | 99 | 1 | 4 | 104 |
| derotation and decompression | 25 | 1 | 2 | 28 | |
| adhesiolysis or band release | 8 | 1 | 0 | 9 | |
| resection anastomosis | 29 | 6 | 6 | 41 | |
| stoma | 1 | 0 | 0 | 1 | |
| hernia repair | 3 | 3 | 3 | 9 | |
| peritonal lavage for peritonitis secondary to perforated appendicitis | 16 | 1 | 0 | 17 | |
| omental patch for perforated PUD | 3 | 1 | 4 | 8 | |
| bowel repair for typhoid perforation | 1 | 0 | 0 | 1 | |
| reduction for intussusception | 6 | 1 | 0 | 7 | |
| Total | 191 | 15 | 19 | 225 | |
Discussion
There are very few studies done on the general pattern of non tramatic acute abdomen in Ethiopia. Twenty years passed after study done in the vicinity (yirgalem general hospital 2000GC) of the sidama region on the general pattern of acute abdomen. In our study there were 225 cases operated in LGH for indication of non-traumatic acute abdomen with male preponderance. Majority of the patients were in the second decades of life similar to the studies done in NRH, TAH and other African countries. As other studies, in this study also showed rural resident preponderance [1,6]. Almost similarly with study in dill chora, Nekemt referral hospital, goba referral hospital, abdominal pain, vomiting, constipation and abdominal distension were the commonest presenting symptoms of the patients. As others study showed there is also similarity in delay to presentation to hospital. majority of the patients presented after 24hrs of pain started which is against the slogan “the sun should not set and rise on acute abdomen’’ [2,4,16]. Acute appendicitis was found to be the leading cause of non-traumatic surgical acute abdomen leading to emergency operations in this study. This is contrary to the study done 20yrs back in yirgalem general hospital in the vicinity which found intestinal obstruction as the main cause of acute abdomen. This study shows the changing pattern. Other than yirgalem hospital, Gonder university hospital found intestinal obstruction as main cause of non-traumatic acute abdomen. But studies in NRH, west Ethiopia, dillchora referral hospital, east Ethiopia and Goba referral hospital depicted appendicitis as the leading cause of non-traumatic surgical abdomen in their findings [2-7].
Bowel obstruction was found the second most common cause of non-traumatic acute abdomen in this study which accounted 34.2% of all cases. This finding is in agreement with study done in NRH, TAH and Goba referral hospital. The most common cause of obstruction was found to be SBO and volvulus of small bowel (48.05% from total obstruction and 61.6% from SBO) was the leading cause of SBO. This is in contrast with study in addis abeba, Teklehaimanot general hospital, Adama general hospital and certain African country study done from Nigeria by Adesunkami which all reported adhesion as frequent cause of SBO. Sigmoid volvulus was the most frequent cause of LBO in agreement with most studies in Ethiopia and other African countries [1,7,8-13,18]. Most of the cases were operated by IESO (84.9%). Studies depicted the performance of IESO on emergency surgeries and the role of task-shifting specially in reduction of maternal and perinatal mortalities. This study also showed the positive role of the IESO even in a hospital where specialist consultant surgeons availed [15,16]. The overall mortality rate in this study was 2.2% which was lower than most of reports in Ethiopia. Delay in presentation was the major factor for unfavorable outcome of the cases; among the 5 died patients were 4(80%) were SBO cases which presented late and with non-viable bowel ischemia.
Conclusion
In this study we noticed that emergency operation for non-traumatic acute abdomen was found to be the commonest emergency surgical interventions. Appendicitis was found to be the commonest among others in the LGH. Most emergency operations were done by integrated emergency surgeons and their role in managing emergency acute abdomens was undeniable and effective in emergency general surgeries beyond their involvement in obstetrics and gynecologic emergency operations. The overall mortality rate was 2.2%.
References
- Adem A, Abebe A & Abdurahman M. (2001). Pattern of surgical admissions to Tikur Anbessa Hospital, Addis Ababa, Ethiopia. East and Central African Journal of Surgery, 6(1).
Publisher | Google Scholor - Ayenew Z, Gizaw A.T, Workneh D & Fentahun N. (2017). Outcome of Non-Traumatic Surgical Acute Abdomen in Nekemte Referral Hospital Southwest Ethiopia: A Retrospective Cross-Sectional Study.
Publisher | Google Scholor - Tsegaye, Sisay Tamene et al. (2007). “Surgically Treated Acute Abdomen at Gondar University Hospital, Ethiopia.” East and Central African Journal of Surgery, 12(2007):53-57.
Publisher | Google Scholor - Melkie A, Alemayehu T & Tarekegn E. (2016). Pattern of Acute Abdomen in Dil Chora Referral Hospital, Eastern Ethiopia. International journal of collaborative research on internal medicine and public health, 8.
Publisher | Google Scholor - Gebrie T, Handiso T & Hagisso S. (2019). Management outcome and associated factors of surgically treated non traumatic acute abdomen at Attat Hospital, Zone, Ethiopia. Int J Surg Res Pract, 6:99.
Publisher | Google Scholor - Asefa Z. (2000). Pattern of acute abdomen in Yirgalem Hospital, southern Ethiopia. Ethiop Med J, 38(4):227-235.
Publisher | Google Scholor - Tassew B, Haile MT, Tefera TB, Balda SS, Gonfa KB and Mubashir K. (2017). Presentation and Outcome of Acute Abdomen in Goba Referral Hospital, Goba, Southeast Ethiopia: Retrospective Study. SM J Fam Med, 1(1):1003.
Publisher | Google Scholor - Ademe Y, Seyoum N, Lemma R. (2022). Surgical Management of Acute Abdomen in Adult Patients: Experience from a Private Hospital in Addis Ababa, Ethiopia. Ethiop J Health Sci, 32(4):729-738.
Publisher | Google Scholor - Atalay M, Gebremickael A, Demissie S, Derso Y. (2021). Magnitude, pattern and management outcome of intestinal obstruction among non-traumatic acute abdomen surgical admissions in Arba Minch General Hospital, Southern Ethiopia. BMC Surg, 21(1):293.
Publisher | Google Scholor - Awedew, Atalel & Ayele, Tesfaneh. (2022). Epidemiological pattern and outcomes of surgical acute abdomen in Ethiopia: A meta-analysis.
Publisher | Google Scholor - Gebresellassie HW, Tamerat G. (2019). Audit of surgical services in a teaching hospital in Addis Ababa, Ethiopia. BMC Res Notes, 12(1):678.
Publisher | Google Scholor - Soressa U, Mamo A, Hiko D, Fentahun N. (2016). Prevalence, causes and management outcome of intestinal obstruction in Adama Hospital, Ethiopia. BMC Surg, 16(1):38.
Publisher | Google Scholor - Ghebrat, K. (2001). Seasonal variation of primary small intestinal volvulus in North Western Ethiopia. East and Central African Journal of Surgery, 6(2).
Publisher | Google Scholor - Hagos M. (2015). Acute Abdomen in Adults: A Two-Year Experience in Mekelle, Ethiopia. Ethiop Med J, 53(1):19-24.
Publisher | Google Scholor - McConkey, S. (2002). Case Series of Acute Abdominal Surgery in Rural Sierra Leone. World Journal of Surgery, 26:509-513.
Publisher | Google Scholor - Triadafilopoulos G, Legha P & Lombard C. (2018). Sun Should Not Rise and Set on a Case of Acute Intestinal Obstruction. Dig Dis Sci, 63:27-31.
Publisher | Google Scholor - Gobeze A. A, Kebede Z, Berhan Y & Ghosh B. (2016). Clinical performance of emergency surgical officers in southern Ethiopia. Ethiopian Journal of Health Sciences, 26(5):463-470.
Publisher | Google Scholor - Kotiso B, Abdurahman Z. (2006). Pattern of acute abdomen in adult patients in Tikur Anbessa Teaching Hospital, Addis Ababa, 12(1):47-52.
Publisher | Google Scholor - Adesunkanmi AR, Agbakwuru EA. (1996). Changing pattern East Cent Afr J Surg of acute intestinal obstruction in a tropical African population. East Afr Med J, 73(11):727-731.
Publisher | Google Scholor













