

Research Article
Nonampullary Duodenal Neoplasms Can Be Safely and Less Invasively Removed with Clip-Guided Local Duodenectomy
- Hassan A. Saad 1*
- Azza Baz 2
- Mohamed Riad 1
- Mohamed E Eraky 1
- Khaled Sharaf 1
- Lotfy A. Ibrahim 3
- Mohamed I Farid 1
¹ Surgical Department, Faculty of Medicine, Zagazig University, Zagazig City, Egypt.
² Surgical Department, Alahrar Teaching Hospital, Zagazig University, Zagazig City, Egypt.
³ Surgical Department, AlAzhar University, Nasr City, Cairo, Egypt.
*Corresponding Author: Hassan A. Saad, Surgical Department, Faculty of Medicine, Zagazig University, Zagazig City, Egypt.
Citation: Hassan A. Saad, Baz A, Riad M, Mohamed E Eraky, Sharaf K, et al. (2024). Nonampullary Duodenal Neoplasms Can Be Safely and Less Invasively Removed with Clip-Guided Local Duodenectomy. Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers. 3(1):1-12. DOI: 10.59657/2992-9989.brs.24.020
Copyright: © 2024 Hassan A. Saad, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 27, 2024 | Accepted: February 26, 2024 | Published: March 14, 2024
Abstract
Background: For certain nonampullary duodenal neoplasms, a straightforward treatment approach is local duodenectomy and primary closure. A safe primary duodenal closure requires curability and minimization of the resection area. However, finding the proper resection line from the serosal side can be challenging. To improve the safety and ease of local duodenectomy, we created a clip-guided local duodenectomy. To validate the safety of this procedure, we conducted retrospective observational research.
Methods: During the procedure, four endoscopic metal clips were placed on the margin surrounding the tumor three days prior to surgery. The clips are then used to determine the extent of the tumor during X-ray imaging; an incision is made to the duodenum just outside of the clips; a full-thickness resection of the duodenum is performed using the clips as guides to demarcate the tumor; and the incision is closed transversely using a Gambee suture. Between March 2010 and February 2020, one surgical center evaluated the clinicopathological data and surgical outcomes of patients who underwent local duodenectomy under clip guidance.
Results: There were eighteen patients in total. Adenoma (11 patients), adenocarcinoma (6 patients), and GIST (1 patient) were pathologically diagnosed. The primary location of the tumors was in the second part of the duodenum, accounting for 66% of the total tumor size, with a mean size of 18 ± 6 mm. Primary sutures were used for each patient to repair the duodenal defect. The mean operation time was 191 minutes, while the mean blood loss was 79 millilitres. There was a 22% morbidity rate, and all complications were Grade II complications according to the Clavien‒Dindo system. There was no evidence of anastomotic leakage or stenosis. All six of the adenocarcinoma patients had pT1a disease, and there was no evidence of postoperative recurrence. The overall 1-year survival rate was 100%, with no recurrences.
Conclusion: Clip-guided local duodenectomy is a safe and effective way to remove nonampullary duodenal neoplasms such as duodenal adenoma, GIST, and early adenocarcinoma with minimal damage to the surrounding tissue.
Keywords: nonampullary duodenal; neoplasms; less invasively; clip-guided local duodenectomy
Introduction
Approximately 1-5% of patients referred for upper gastrointestinal endoscopy have nonampullary duodenal neoplasms (NADNs) [1,2]. These lesions are both mucosal and submucosal, and the most common treatment for them is surgery. Examples of these lesions include gastrointestinal stromal tumors (GISTs), adenomas, and adenocarcinomas [3,4]. Endoscopic or surgical removal of the adenoma is also performed based on endoscopic findings [5]. This is because duodenal adenomas can progress to adenocarcinomas.
Although pancreaticoduodenectomy (PD) is the standard radical surgery for treating NADNs, limited resection has been reported to be preferable for benign duodenal neoplasms and early duodenal carcinoma, as these conditions are not associated with a risk of regional lymph node metastasis [4,6,7,8]. These procedures include local resection, pancreas-sparing duodenectomy, and segmental duodenectomy. The most advantageous course of treatment for NADNs may involve full-thickness, local excision of the duodenum, followed by hand-sewn closure of the defect. This procedure is straightforward and safe [3,8,9]. Determining the ideal resection margin for local excision from the serosal side can be challenging, particularly if the tumor is restricted to the mucosa. For local resection of the duodenum to safely close the defect, there should be a minimally sufficient resection margin surrounding the tumor. The defect needs to be repaired with an ileum patch or other reconstruction if the resection margin is too large to be closed with primary sutures. Determining the best incision to make in the duodenum is essential for safe resection since this approach guarantees that the tumor has a minimally sufficient resection margin. To date, nevertheless, the best way to ascertain this from the serosal side has not been determined.
To identify a minimal and sufficient resection margin, we devised a novel technique for local duodenal resection employing endoscopic metal clips to detect the tumor margin intraoperatively from the serosal side by palpation and X-ray imaging. A retrospective observational study was carried out to investigate the safety of clip-guided local duodenectomy (CGLD) for removing NADNs. Here, we report the operative outcome of CGLD for NADNs and detail our surgical approach.
Methods
Patient features
Between March 2010 and February 2020, CGLD was carried out at two regional high-volume centres: Zagazig University. For perioperative and clinicopathological data, medical records were examined. Age, sex, tumor location, tumor size, and pathological diagnosis were included in the clinicopathological data. The perioperative data included the operation duration, blood loss, physical state categorization of the American Society of Anesthesiologists (ASA-PS), start of oral feeding, hospital stay, and postoperative problems. The Union for International Cancer Control-Tumor Node Metastasis (UICC TNM) system was used to create the T classifications for duodenal adenocarcinoma [10]. This system is used to describe malignant small intestine tumors. The first (D1), second (D2), and third (D3) portions of the duodenum are where the tumor is located. The Clavien‒Dindo classification was used to calculate the incidence of postoperative complications [11]. Tumor marker levels were checked every three months, CT scans every six months, and duodenal endoscopy every year for patients with adenocarcinomas.
Significance of CGLD
The following criteria were established for the classification of duodenal neoplasms as CGLD: (1) NADNs that are more than 2 cm from the vater ampulla; (2) adenoma, superficial adenocarcinoma, or GIST as the histological diagnosis; (3) lesions that cover up to half of the circumference of the duodenal wall on endoscopy; (4) a tumor location that allows the vater ampulla to stay in place; and (5) inability to perform endoscopic resection. Segmental resection or local resection followed by jejunal reconstruction should be performed if the tumor is larger than half the circumference. Since local resection of the tumor located on the pancreatic side of the duodenum is not an effective treatment option, pancreaticoduodenectomy or segmental resection is recommended.
Method of surgery (Figure 1).
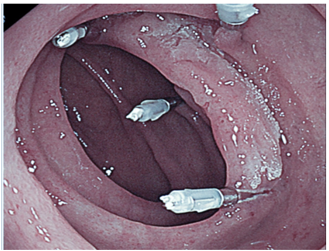
Figure 1: Two or three days prior to surgery, the metal clips were endoscopically positioned close to the tumor edge.
Two or three days before surgery, every patient underwent endoscopy to mark any tumors with metal clips. After carefully examining the margin, the endoscopists placed four clips around the tumor (Figure 1). Because insufflated gas may cause intestinal dilatation and interfere with surgical operation, and because intraoperative endoscopy may not be able to find the tumor margins precisely, it is better to implant the clip prior to surgery. After an upper median laparotomy, the tumor sites were confirmed during surgery by palpation and visualization of the four clips on an X-ray (Figs. 2, 3a). Before addressing the tumor, the Kocher technique was used. If the tumor was situated at D3, the hepatic flexure and transverse colon mesentery were mobilized. Under imaging, a full-thickness incision was made in the duodenum wall immediately outside of the clips, and stay sutures were applied to both ends of the lesion (Fig. 3b). The tumor and clips were directly visible during the full-thickness resection and tumor excision procedure (Figs. 3c, 4). Gambee sutures were used to transversely seal the duodenal wall defect (Figs. 3d, 5). To detect leaks, a drainage tube was inserted behind the anastomosis. If there were no issues once the patient began oral intake, the tube was withdrawn approximately seven days after surgery. Oral intake was started approximately five days after surgery and was typically performed four days after surgery using iodine-containing contrast medium, during which the anastomosis was revealed to be intact.
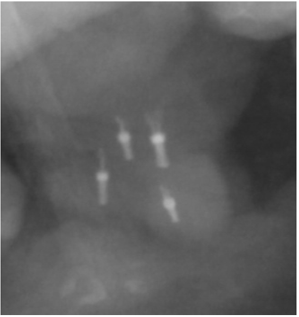
Figure 2: Intraoperative X-ray imaging revealed clips on the tumor's margin.
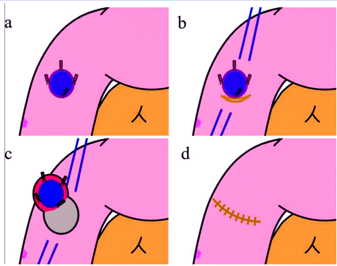
Figure 3: Diagram illustrating the method of clip-guided local duodenectomy. The four clips were found during the upper median laparotomy using X-ray imaging. A full-thickness incision was made in the duodenum wall just outside of the clips under imaging, and stay sutures were applied to both ends of the lesion. The tumor and clips were visible during full-thickness duodenal resection. Gambee sutures were used to transversely close the duodenal wall defect [32].
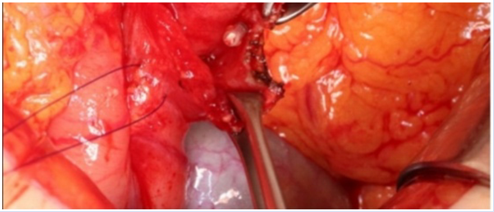
Figure 4: Immediately outside of the clips, a full-layer incision was made in the duodenum wall. Making an incision with the clips serving as a guide allowed the tumor to be removed with the fewest possible margins.

Figure 5: Gambee sutures were used to create a single-layer closure for the duodenal lesion.
Results
Clinical qualities
Two regional facilities performed CGLD on a total of twenty-three individuals. Using clip guidance under X-ray imaging, the tumors were easily identified in all patients, and hand-sewn sutures were used to heal all the duodenal abnormalities. The analysis did not include five patients who had cooperative operations for CGLD, such as hepatectomy and cholecystectomy. Table 1 displays the clinicopathological features and surgical results for the 18 patients. There were 13 men and 5 women, with a mean age of 63.1 ± 11.3 years. The mean± SD BMI was 23.8 ± 2.9 kg/m2. The serum ALB concentration was 4.1 ± 0.3 g/dL before surgery. Two patients had cerebrovascular illness and chronic renal failure, which were severe systemic disorders (ASA-PS III). Twelve individuals met the criteria for mild systemic illness (ASA-PS II), which included diabetes mellitus and hypertension. Eleven patients had an adenoma, six had an adenocarcinoma, and one had a GIST pathological diagnosis. Every adenocarcinoma patient had a pT1a tumor depth. A tumor was found at D1 in 1 patient, D2 in 12 individuals, and D3 in 5 patients. The mean ± SD tumor size was 17.7 ± 5.8 mm.
Table 1: Patient characteristics, surgical results, and complications after surgery.
| Variables | Data |
| Background characteristics | |
| Sex, male: female | 13:5 |
| Age, y, mean ± SD | 63.1 ± 11.3 |
| BMI, kg/m2, mean ± SD | 23.8 ± 2.9 |
| ASA-PS, I/II/III | 4/12/2 |
| Preoperative albumin, g/dL, mean ± SD | 4.1 ± 0.3 |
| Disease, n (%) | |
| Adenoma | 11 (61) |
| Adenocarcinoma | 6 (33) |
| GIST | 1 (6) |
| Tumor size, mm, mean ± SD | 17.7 ± 5.8 |
| Location, n (%) | |
| D1 | 1 (6) |
| D2 | 12 (66) |
| D3 | 5 (28) |
| Outcomes of surgery | |
| Operation time, min, mean ± SD | 191 ± 72 |
| Blood loss, mL, mean ± SD | 79 ± 121 |
| Time to first oral feeding, d, median (range) | 7 (2–26) |
| Hospital stays, d, median (range) | 17.5 (9–37) |
| Negative pathological tumor margin, n (%) | 18 (100) |
| Tumor recurrence, n | 0 |
| Mortality, n | 0 |
| Postoperative complications | |
| Morbidity, n (%) | 4 (22) |
| Clavien–Dindo classification, n (%) | |
| I | 0 |
| II | 4 (22) |
| IIIa–V | 0 |
| Reoperation, n | 0 |
The American Society of Anesthesiologists (ASA-PS) evaluates the physical status of the duodenum in the first, second, and third segments, referred to as D1, D2, and D3, respectively.
Operational outcomes and endurance
The mean operation time was 191 minutes, while the mean blood loss was 79 millilitres. The mean operation times for the tumors on D1, D2, and D3 were 144, 180, and 226 minutes, respectively. When the tumors were on D2 or D3, the operation took longer on average. This could be the case because, to access D2 and D3 lesions, the Kocher manoeuvre and transverse mesocolon must be mobilized. The hospital stay was 18 days, and the average postoperative fasting period was 7 days. There was no discernible difference in the duration of hospitalization or postoperative fasting days among patients with varying tumor sites, sizes, or clinical diagnoses. For every patient, the pathological tumor margin was negative. During the median follow-up length of 883 days (range 197–2090) among the adenocarcinoma patients, there were no deaths from any cause or recurrences of the cancer. The overall 1-year survival rate was 100%, with no recurrences.
Difficulties
Postoperative morbidity as a whole was 22%. Complications included delayed stomach emptying in 2 (11%) individuals, pneumonia in 1 (6%) patient, and surgical site infection in 1 (6%) patient (Table 2). All complications were Clavien‒Dindo grade II. All patients received conservative treatment to alleviate these issues, and none of them experienced Grade III or higher complications. Anastomotic leakage or other potentially fatal issues did not affect any of the patients. The sizes and locations of the tumors did not correlate with surgical outcomes. There were no recorded hospital deaths or reoperations.
Table 2: Postoperative Complication Details
| Age | Sex | Location | Complication (C–D grade) | Hospital stays, d |
| 78 | Male | D2 | DGE (II) | 37 |
| 61 | Male | D2 | SSI (II) | 29 |
| 53 | Male | D3 | DGE (II) | 28 |
| 74 | Male | D3 | Pneumonia (II) | 16 |
The duodenum was divided into two sections, D2 and D3: delayed gastric emptying (DGE), surgical site infection (SSI), and Grade C–D according to the Clavien–Dindo classification.
Discussion
The current study assessed the utility and safety of CGLD for the treatment of NAFLD. To obtain minimally sufficient local excision for NADNs, the clip-guided approach was helpful. The defects were successfully closed in all CGLD patients without the need for an ileal patch or anastomotic reconstruction. Following CGLD, there was no stenosis or leakage. There were no reports of severe complications or postoperative mortality. Furthermore, there was no evidence of lymph node metastasis or local recurrence in duodenal pT1a adenocarcinoma patients.
The usual surgical approach for early-stage duodenal cancer and benign duodenal neoplasms is unknown [4]. Duodenal cancer lymph node metastases are associated with a poor prognosis [12, 13], and PD is advised for aggressive treatment of duodenal carcinoma [14, 15]. The majority of the patients included in these studies had T2 or more advanced duodenal cancer. Limited resection for T1 duodenal cancer was reported in two patients. According to Kohga et al. [8], only one of the five patients (20%) with T1b disease experienced lymph node metastases, but none of the 34 patients with T1a duodenal cancer did. According to Kato et al. [6], not every patient with T1a/T1b duodenal carcinoma has lymph node metastases (0/15). According to a different study, there is no difference in survival between patients with stage I duodenal cancer who underwent segmental resection and those who underwent PD [7]. These findings suggest that a less invasive surgical approach is adequate for treating T1a duodenal cancer in a curative manner. Some institutions conduct endoscopic submucosal dissection (ESD) for duodenal adenoma, which is the usual treatment for early gastric cancer [2]. Duodenal ESD has been linked to immediate and delayed perforation in 39% of patients and delayed bleeding in 18% of patients. This is because the duodenal wall is thin, and the surgical site is exposed to pancreatic and bile juice [16]. Endoscopists with extensive training in endoscopic closure of the mucosa to prevent perforation should perform duodenal ESD, even though several techniques have been used [17, 18]. For duodenal cancer, laparoscopic-endoscopic cooperative surgery (LECS) may be a good and promising treatment option [19, 20]. However, a highly skilled endoscopist must perform endoscopic resection of the tumor with the proper margins for LECSs to be successful. Consequently, there is a lack of proven practice and safety for duodenal LECSs in general hospitals. Intraoperative endoscopy is not necessary for CGLD, and it is more practical when clips can be positioned on the tumor margin without requiring such a complex endoscopic procedure. A less invasive method called laparoscopic CGLD might be helpful, particularly for D1 and D2 lesions. Because CGLD is an open technique, its usefulness lies in its ability to be conducted outside of high-volume facilities, regardless of the facility's technical capabilities. Duodenal restricted resection has been observed to benefit from segmental duodenectomy and pancreas-sparing duodenectomy [21, 22]. These techniques necessitate restoration utilizing small intestine patch closure or intestinal anastomosis, perhaps with consequences such as leakage and obstruction of passage. Furthermore, when the tumors are adenomas or GISTs, they can result in a broad resection margin of the duodenum. When the resection margin stays within the minimal range and the defects can be fixed safely with surgical suturing, the duodenum may not change much after local resection and defect closure. When the tumor does not need to be removed via lymphadenectomy, it should be sufficient to obtain a minimally appropriate margin surrounding the tumor. Nonetheless, it is necessary to identify the best incision line for a minimally adequate resection margin. To address this, we devised a metallic clip-guided method.
We can more safely close the defect and readily calculate the minimum resection area with this clip-guided approach. Although practically all of the tumors in this study were adenomas or superficial adenocarcinomas, which are invisible and unpalpable from the serosal side, all of the tumors could be easily identified by imaging. It has been reported that marking with dyes such as indocyanine green for location identification during laparoscopic gastrectomy for stomach cancer is feasible [23]. In local duodenal resection, on the other hand, the minimal resection range is very important for avoiding stenosis after surgery. However, feathering during dye labelling can increase the width of the resection range. An ileal patch or anastomotic reconstruction was not necessary for any of the study's subjects since hand stitches were a sufficient method for closing CGLD flaws. Furthermore, there were no instances of CGLD-related anastomotic leakage or stenosis. After limited resection, such as segmental duodenectomy or pancreas-sparing duodenectomy, the intestines need to be rebuilt. This procedure is performed with anastomosis. This procedure can result in anastomotic problems and nonphysiological reconstruction. Among the available techniques for limited duodenal resection, local resection is the most straightforward and well-rounded. There were no cases of lymph node metastasis, peritoneal metastasis, local recurrence, or any distant metastasis in any of the pT1a adenocarcinoma patients. Compared to endoscopic resection, full-thickness resection is more helpful for accurately diagnosing the pT factor when cancers are more advanced. Furthermore, when PD is determined to be necessary, CGLD does not interfere with PD because it does not necessitate sophisticated rebuilding. Endoscopy is frequently necessary for local duodenectomy, particularly when the tumor is confined to the mucosal side, but CGLD can be carried out successfully without this procedure [24]. Moreover, intraoperative endoscopy may not always reveal the entire tumor. The surgeon can quickly identify the clips and the whole tumor region in CGLD. Since CGLD involves accessing the duodenum lumen, it is impossible to rule out the possibility of peritoneal spread. Peritoneal dispersion has not recurred in our experience. The danger of dissemination is the same as that for other limited resection procedures, such as segmental resection and LECS, even though cautious handling is necessary to prevent intestinal contents from leaking out. A tumor smaller than 30 mm should be amenable to partial excision.
This study has certain limitations. First, as this was a retrospective, single-arm observational study, it was not possible to compare CGLD with currently used surgical methods. Second, there is uncertainty about long-term results due to the short observation durations. Third, the study's duration was excessively extended, leading to initial lengthy hospital stays and fasting periods as a result of past modifications, including those in postoperative care. There is a high chance that the anastomosis will leak because it is exposed to bile and pancreatic fluid. This is especially true if there are D2 or D3 lesions. Thus, during the first part of the process, there was a tendency to start the diet cautiously because of worries about anastomotic leakage. The anastomosis was discovered to be extremely stable in the past few years, and hospital stays and postoperative fasting days have generally decreased. Last, it is possible that the clips will loosen before the procedure. The tumor area may be greater than what the remaining clips suggest if three or fewer clips remain near the tumor. Endoscopy should be carried out intraoperatively if four clips are not visible via intraoperative X-ray imaging, even if we have not seen any instances of the clips falling out. Furthermore, to use this procedure, clips must be carefully positioned, leaving no room between them and the tumor's edge. The size of the resected region increases if the clips are positioned away from the tumor. Before performing an endoscopy, surgeons should talk with endoscopists about clip placement. The clips were positioned at four sites to guarantee proper identification of the tumor area.
Conclusion
In summary, CGLD is a helpful and safe technique for accomplishing minimally adequate local duodenectomy for treating NADNs. Treatment should be available for GIST and duodenal adenoma early.
Declarations
Acknowledgements are not applicable
Declaration and ethical clearance
Ethical clearance was obtained from the Institutional Board of Zagagic University, and written informed consent was obtained from all patients, their parents or their first relative. All human experiments were performed in accordance with the relevant guidelines and regulations of the Helsinki declaration.
Consent for publication is not applicable
Availability of database and materials: The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request. All the authors have shared and approved the database. (This manuscript does not report the data generation or analysis).
Competing interests
The authors declare that they have no competing interests or financial disclosures.
Funding
No specific funds were received for this study.
Author contributions
HAS, and ME contributed to the conception and design of MR. HAS: organized the database and performed the statistical analysis. HAS, KS: wrote sections of the manuscript and prepared the tables. MIF, AB, and LAI contributed to the manuscript. revision and investigation. All the authors read, approved, and equally shared the submitted version.
References
- Bartel MJ, Puri R, Brahmbhatt B, Chen WC, Kim D, Simons-Linares CR, et al. (2018). Endoscopic and surgical management of nonampullary duodenal neoplasms. Surg Endosc, 32:2859-2869.
Publisher | Google Scholor - Lim CH, Cho YS. (2016). Nonampullary duodenal adenoma: current understanding of its diagnosis, pathogenesis, and clinical management. World J Gastroenterol, 22:853-861.
Publisher | Google Scholor - Crown A, Biehl TR, Rocha FG. (2016). Local resection for duodenal gastrointestinal stromal tumors. Am J Surg, 211:867-870.
Publisher | Google Scholor - Kakushima N, Kanemoto H, Tanaka M, Takizawa K, Ono H. (2014). Treatment for superficial nonampullary duodenal epithelial tumors. World J Gastroenterol, 20:12501-12508.
Publisher | Google Scholor - Okada K, Fujisaki J, Kasuga A, Omae M, Kubota M, Hirasawa T, et al. (2011). Sporadic nonampullary duodenal adenoma in the natural history of duodenal cancer: a study of follow-up surveillance. Am J Gastroenterol, 106:357-364.
Publisher | Google Scholor - Kato Y, Takahashi S, Kinoshita T, Shibasaki H, Gotohda N, Konishi M. (2014). Surgical procedure depending on the depth of tumor invasion in duodenal cancer. Jpn J Clin Oncol, 44:224-231.
Publisher | Google Scholor - Jiang QL, Huang XH, Chen YT, Zhang JW, Wang CF. (2016). Prognostic factors and clinical characteristics of patients with primary duodenal adenocarcinoma: a single-center experience from China. Biomed Res Int, 2016:6491049.
Publisher | Google Scholor - Kohga A, Yamamoto Y, Sano S, Sugiura T, Okamura Y, Ito T, et al. (2017). Surgical strategy for T1 duodenal or ampullary carcinoma according to the depth of tumor invasion. Anticancer Res, 37:5277-5283.
Publisher | Google Scholor - Shen Z, Chen P, Du N, Khadaroo PA, Mao D, Gu L. (2019). Pancreaticoduodenectomy versus limited resection for duodenal gastrointestinal stromal tumors: a systematic review and meta-analysis. BMC Surg, 19:121.
Publisher | Google Scholor - James DB, Mary KG, Christian W. (2017). TNM classification of malignant tumours. 8th ed. UK: John Wiley & Sons.
Publisher | Google Scholor - Dindo D, Demartines N, Clavien PA. (2004). Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg, 240:205-213.
Publisher | Google Scholor - Poultsides GA, Huang LC, Cameron JL, Tuli R, Lan L, Hruban RH, et al. (2012). Duodenal adenocarcinoma: clinicopathologic analysis and implications for treatment. Ann Surg Oncol, 19:1928-1935.
Publisher | Google Scholor - Li D, Si X, Wan T, Zhou Y. (2019). Outcomes of surgical resection for primary duodenal adenocarcinoma: a systematic review. Asian J Surg, 42:46-52.
Publisher | Google Scholor - Solaini L, Jamieson NB, Metcalfe M, Hilal MA, Soonawalla Z, Davidson BR, et al. (2015). Outcome after surgical resection for duodenal adenocarcinoma in the UK. Br J Surg, 102:676-681.
Publisher | Google Scholor - Sakamoto T, Saiura A, Ono Y, Mise Y, Inoue Y, Ishizawa T, et al. (2017). Optimal Lymphadenectomy for Duodenal Adenocarcinoma: Does the Number Alone Matter? Ann Surg Oncol, 24:3368-3375.
Publisher | Google Scholor - Hoteya S, Yahagi N, Iizuka T, Kikuchi D, Mitani T, Matsui A, et al. (2013). Endoscopic submucosal dissection for nonampullary large superficial adenocarcinoma/adenoma of the duodenum: feasibility and long-term outcomes. Endosc Int Open, 1:2-7.
Publisher | Google Scholor - Akimoto T, Goto O, Sasaki M, Ochiai Y, Maehata T, Fujimoto A, et al. (2016). “Hold-and-drag” closure technique using repositionable clips for large mucosal defects after colonic endoscopic submucosal dissection. Endosc Int Open, 4:1068-1072.
Publisher | Google Scholor - Draganov PV, Wang AY, Othman MO, Fukami N. (2019). AGA institute clinical practice update: endoscopic submucosal dissection in the United States. Clin Gastroenterol Hepatol, 17:16-25.
Publisher | Google Scholor - Irino T, Nunobe S, Hiki N, Yamamoto Y, Hirasawa T, Ohashi M, et al. (2015). Laparoscopic-endoscopic cooperative surgery for duodenal tumors: a unique procedure that helps ensure the safety of endoscopic submucosal dissection. Endoscopy, 47:349-351.
Publisher | Google Scholor - Ojima T, Nakamori M, Nakamura M, Hayata K, Katsuda M, Takifuji K, et al. (2018). Laparoscopic and endoscopic cooperative surgery versus endoscopic submucosal dissection for the treatment of low-risk tumors of the duodenum. J Gastrointest Surg, 22:935-940.
Publisher | Google Scholor - Stauffer JA, Raimondo M, Woodward TA, Goldberg RF, Bowers SP, Asbun HJ, et al. (2013). Laparoscopic partial sleeve duodenectomy (PSD) for nonampullary duodenal neoplasms: avoiding a whipple by separating the duodenum from the pancreatic head. Pancreas, 42:461-466.
Publisher | Google Scholor - Konishi M, Kinoshita T, Nakagohri T, Takahashi S, Gotohda N, Ryu M. (2007). Pancreas-sparing duodenectomy for duodenal neoplasms including malignancies. Hepatogastroenterology, 54:753-757.
Publisher | Google Scholor - Ushimaru Y, Omori T, Fujiwara Y, Yanagimoto Y, Sugimura K, Yamamoto K, et al. (2019). The feasibility and safety of preoperative fluorescence marking with indocyanine green (ICG) in laparoscopic gastrectomy for gastric cancer. J Gastrointest Surg, 23:468-476.
Publisher | Google Scholor - Poves I, Burdio F, Alonso S, Seoane A, Grande L. (2011). Laparoscopic pancreas-sparing subtotal duodenectomy. JOP, 12:62-65.
Publisher | Google Scholor













