

Case Report
Neuroendocrine Tumor of Appendix-A Case Report
1Post Graduate Student, Dept. of General Surgery, Bombay Hospital & Institute of Medical Sciences, India.
2Assistant Professor, Maharashtra University of Health Sciences, Nashik Postgraduate Teacher, Bombay Hospital Institute of Medical Sciences, Chamber no. 108, Bombay Hospital Avenue, New Marine Lines, Mumbai India.
*Corresponding Author: Chatterjee Sanjay, Assistant Professor, Maharashtra University of Health Sciences, Nashik Postgraduate Teacher, Bombay Hospital .
Citation: Shaikh M. Shaad, Keshavi M, Nayan G, Sanjay C. (2024). Neuroendocrine Tumor of Appendix-A Case Report. Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers. 3(1):1-3. DOI: 10.59657/2992-9989.brs.24.021
Copyright: © 2024 Chatterjee Sanjay, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 08, 2024 | Accepted: March 23, 2024 | Published: March 16, 2024
Abstract
Neuroendocrine tumors (NETs) are characterized by their ability to secrete hormones. NETs can develop in any organ of the gastrointestinal system. NETs of appendix are rare in occurrence with an estimated incidence of 0.15 to 06 cases/year per 100,000 people and are often seen in young adults with a higher male preponderance. NETs of the appendix are usually asymptomatic and are discovered incidentally after appendectomy. Treatment is by surgical removal of the tumor with a healthy margin in accordance with the principles of oncology.
Here we report on a case of a 40-year-old male patient. Admitted with sudden onset right iliac fossa pain with no fever. Emergency abdominal ultrasound revealed a 1-cm dilated non-peristaltic blind loop of bowel with moderate fat stranding suggestive of acute appendicitis. The biochemical work-up revealed leukocytosis with a predominance of neutrophils. The patient underwent laparoscopic appendicectomy. Histopathological examination showed an incidental neuroendocrine tumor of appendix Grade 1, less than 2 cm with no lympho-vascular invasion with a free base.
Keywords: appendix; carcinoid tumor; neuroendocrine tumor; right hemi-colectomy
Introduction
Neuroendocrine tumors (NETs) are mainly arise from enterochromaffin cells present in the gastrointestinal tract and the respiratory system. Neuroendocrine tumors of the appendix are the third most common GI neuroendocrine tumor after small intestine and rectum. Appendicular neoplasms are rare in occurrence. Their presentation is mostly asymptomatic. Tumors of the appendix are mostly incidental and are identified in patients operated on for acute appendicitis. They are detected in about 1% of appendectomy specimens on histopathological examination [1]. Current guidelines suggest that a simple appendectomy is an adequate treatment for NETs if they are less than 1 cm in size, and a right hemicolectomy is recommended for those larger than 2 cm involving the base and with higher grades. However, the ideal treatment for tumors between 1 and 2 cm is still unclear.
Case Report
Our case was a 40-year-old gentleman who presented sudden onset right lower abdominal pain since few hours with no history of fever, reduced appetite, nausea or vomiting. Pain was localized to the right lower quadrant and was non-migratory. Patient did not complain of any increased frequency of urination or burning sensation while passing urine. No bowel complaints. On Examination, the patient was fairly built, pulse was 110 bpm and BP was 110/70mmhm. Abdominal examination revealed tenderness at McBurney’s point with no lump and rebound tenderness. Rest of the examination was within normal limits. An emergency abdominal and pelvic ultrasound was performed which revealed a 10 mm dilated non peristaltic blind ending structure in the right iliac fossa with moderate peripheral fat stranding with no faecolith suggestive of Acute appendicitis. Patient was posted for Diagnostic laparoscopy which revealed thickened inflamed appendix with small bowel flimsy adhesions. Careful adhesiolysis was done. Mesoappendix was divided and appendicectomy was performed. A tube drain was placed in the pelvis. Patient tolerated the procedure well and was discharged on POD-2 tolerating full diet. On Follow-up examination, the histopathology report revealed an incidentally detected Neuroendocrine tumor of the appendix less than 2 cm involving the tip with free base and mesoappendix invading only up to sub-mucosa and well differentiated Grade 1 morphology.
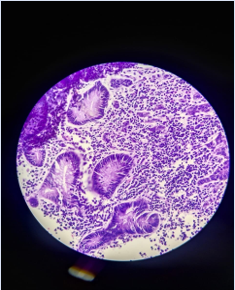
Figure 1: Round or oval nuclei with salt & pepper chromatin & eosinophilic granular cytoplasm in nested pattern.
Discussion
Primary neuroendocrine neoplasia (NEN) has the propensity to develop in any organ of the digestive system. According to the most recent data from the North American Epidemiology Registry (SEER), the most common GI NENs are those arising in the small intestine or rectum, pancreas and stomach or appendix in the order of incidence. Other locations, such as the oesophagus, liver or bile ducts, are exceptional [3]. Neuroendocrine tumor of the appendix is a rare entity [4]. The annual incidence of neuroendocrine tumors of the appendix is estimated to be 0.15 up to 0.6 cases/year per 100,000 people [5]. Their prevalence is estimated to be between 0.3 and 0.9% of appendectomy patients; 95% of appendiceal carcinoid tumors are less than 2 cm in size and 75% of them are located in the distal third of the appendix [6]. Age of the patient at diagnosis is unique in appendiceal carcinoid tumors, and are often seen in young adults [8]. There are no specific clinical signs or symptoms associated with appendiceal carcinoids. Most NETs of the appendix are asymptomatic and usually discovered incidentally during appendectomy or other benign pelvic surgery. More than 50% of carcinoids mimic acute appendicitis with the classic right lower quadrant abdominal pain, which leads to appendectomy [9]. Carcinoid syndrome is very rare (<1>
Table: Recommended surgical strategies for appendiceal NETs based on specific clinical and histological characteristics.
| Indications | Type of operation |
| Tumor size< 1 cm | Appendicectomy |
| Tumorsize 1-2 cm | Appendicectomy + Regular F/Up for 5 years |
| Tumor size> 2 cm | Right hemicolectomy |
| Location of the tumorat the base of the appendix | Right hemicolectomy |
| Infiltration of the cecum | Right hemicolectomy |
| Positive surgical resection margins | Right hemicolectomy |
| Appendiceal mesentery invasion | Right hemicolectomy |
| Metastatically infiltrated mesoappendiceal lymph node | Right hemicolectomy |
| Presence of undifferentiated or low differentiated cells | Right hemicolectomy |
| Presence of goblet cells | |
| Goblet cell carcinoma in males | Right hemicolectomy |
| Goblet cell carcinoma in females (regardless of age) | Righthemicolectomy + Bilateral salpingo-oophorectomy |
| Peritoneal dissemination from goblet cell carcinoma | Cytoreductive surgery + Adjuvant intraperitoneal chemotherapy |
In particular for tumors larger than 2 cm, a CT scan and somatostatin receptor scan (SRS) is recommended at 6 months and 12 months postoperatively and then annually. Colonoscopy is recommended for the early detection of large bowel tumors that are synchronous or metachronously developed [10]. The use of plasma chromogranin-A levels as a tumor marker contributes to the differential diagnosis of caliciform cell carcinoma, early detection of recurrence and long-term follow-up of metastatic disease. All patients should be examined 6 and 12 months after surgery and then annually, while follow- up should be lifelong [10]. Hematological investigations, biochemical or urinary investigations are only indicated in rare carcinoid syndrome to monitor disease progression [9].
Conclusion
Post-operative oncological follow-up is not necessary for tumors smaller than 1 cm. On the other hand, it is essential for high-risk tumors and involves an abdominal scan at 3 months post-operatively and then every 6 to 12 months for 10 years. A colonoscopy should also be performed at a distance from the operation to look for a synchronous tumor [4]. Neuroendocrine tumors of the appendix are rare and can be discovered by chance. Its clinical picture is unrecognized, often misleading and non- specific. It is mistaken for acute appendicitis. Although neuroendocrine tumors of the appendix are frequently rare, knowledge of the therapeutic management of these tumors is very important as they have a poor prognosis.
References
- Bayhan Z, Yildiz YA, Akdeniz Y, Gonullu E, Altintoprak F, Mantoglu B, et al. (2020). Appendix Neuroendocrine Tumor: Retrospective Analysis of 4026 Appendectomy Patients in a Single Center. Emergency Medicine International, 2020:1-6.
Publisher | Google Scholor - Morais C, Silva E, Brandão PN, Correia R, Foreid S, Valente V. (2019). Neuroendocrine tumor of the appendix—a case report and review of the literature. Journal of Surgical Case Reports, 3.
Publisher | Google Scholor - Néoplasies Neuroendocrines (NNE) digestives. Société Nationale Française de Gastro-Entérologie. [Internet].
Publisher | Google Scholor - Meyer DJ, Balaphas A, Koessler T, Morel PP, Bühler L, Buchs DN. (2018). Tumors of the appendix and their management. Swiss Medical Review, 5.
Publisher | Google Scholor - Bahi L, Oqbani K, Karich N, Mounhoub M. Tumor of the Appendix: A Case Report. International Journal of Advanced Research. 2018; 6(11): 697-701.
Publisher | Google Scholor - Dousset B. (2006). Surgical treatment of endocrine tumors of the digestive tract. The Letter of the Hepato-Gastroenterologist, 1(9):32-35.
Publisher | Google Scholor - Hof KH, van der Wal HC, Kazemier G, Lange JF. (2008). Carcinoid Tumour of the Appendix: An Analysis of 1,485 Consecutive Emergency Appendectomies. J Gastrointest Surg, 12(8):1436-1438.
Publisher | Google Scholor - Pickhardt PJ, Levy AD, Rohrmann CA, Kende AI. (2003). Primary Neoplasms of the Appendix: Radiologic Spectrum of Disease with Pathologic Correlation. Radio Graphics, 23(3):645-662.
Publisher | Google Scholor - Ploenes T, Börner N, Kirkpatrick CJ, Heintz A. (2013). Neuroendocrine Tumour, Mucinous Adenocarcinoma and Signet-Ring Cell Carcinoma of the Appendix: Three Cases and Review of Literature. Indian J Surg, 75(1):299-302.
Publisher | Google Scholor - Griniatsos J. (2010). Appendiceal neuroendocrine tumors: Recent insights and clinical implications. WJGO, 2(4):192.
Publisher | Google Scholor - Tchana-Sato V. (2006). Carcinoid tumor of the appendix: A consecutive series from 1237 appendectomies. WJG, 12(41):6699.
Publisher | Google Scholor - Modlin IM, Lye KD, Kidd M. (2003). A 5-decade analysis of 13,715 carcinoid tumors. Cancer, 97(4):934-959.
Publisher | Google Scholor












