

case report
Multiple Polycystic Organs in A Middle Age Female: A Rare Case of More Than Ten Years Without Surgical Intervention
1.Associate Professor of Surgery, University of Khartoum- Faculty of Medicine- Department of Surgery, Sudan.
2.Professor of Surgery, University of Khartoum- Faculty of Medicine- Department of Surgery, Sudan.
*Corresponding Author: Randa Zaki A M Khair,Associate Professor of Surgery, University of Khartoum- Faculty of Medicine- Department of Surgery, Sudan
Citation: R.Z.A.M. Khair, M.M.M Ibrahim. (2023). Multiple Polycystic Organs in A Middle Age Female: A Rare Case of More Than Ten Years Without Surgical Intervention, International Journal of Medical Case Reports and Reviews, BRS Publishers. 2(3); DOI: 10.59657/2837-8172.brs.23.027
Copyright: © 2023 Randa Zaki A M Khair, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 03, 2023 | Accepted: July 18, 2023 | Published: July 26, 2023
Abstract
Some organs are recognized to develop cysts more common than others do; these include the kidney the liver, the pancreas and the spleen. The structure and function of these organs may play a role. The frequency of polycystic kidney is variable. It is reported as 50 or less in100000 (5 in 10000), 1 in 400 and 1 in 1000 life birth. Prevalence of autosomal dominant polycystic kidney disease (ADPKD) is thought to be overestimated by 2 to 5 folds. Multiplepolycystic organs are not common, and reviewing the literature revealed some case reports, which indicatesthat such cases do not have regularpattern. Inherited polycystic kidney disease has two varieties; autosomal dominant polycystic kidney disease (ADPKD) and autosomal recessive polycystic kidney disease (ARPKD).
Keywords: polycystic; liver; kidney; pancreas
Introduction
Some organs are recognized to develop cysts more common than others do; these include the kidney the liver, the pancreas and the spleen. The structure and function of these organs may play a role. The frequency of polycystic kidney is variable. It is reported as 50 or less in 100000 (5 in 10000), 1 in 400 and 1 in 1000 life birth [1, 2]. Prevalence of autosomal dominant polycystic kidney disease (ADPKD) is thought to be overestimated by 2 to 5 folds [2]. Multiple polycystic organs are not common, and reviewing the literature revealed some case reports, which indicates that such cases do not have regular pattern.
Inherited polycystic kidney disease has two varieties; autosomal dominant polycystic kidney disease (ADPKD) and autosomal recessive polycystic kidney disease (ARPKD) [3-7]. Polycystic liver disease is one of the known associations with ADPKD [4]. Polycystic kidney is also associated with polycystic lung, brain, ovary and other organs [4,7,8]. ADPKD is characterized by slowly progressive kidney enlargement that may progress to end stage renal failure in about 2.5% of patients [7]. Hypertension is common in 60% of patients with ADPKD [7]. Patients with ARPKD have variable natural history. More than half of them presented in the neonatal period. They frequently experience liver fibrosis which is complicated in 20-60% by portal hypertension and consequently the patients present with esophageal varices. Nonetheless portal hypertension rarely causes disturbance in liver function and hence rarely fatal [7]. Some patients with ADPKD develop severe respiratory complications that require prolonged ventilation and most of the patients die with respiratory failure or sepsis mainly in the neonatal period [7].
Polycystic disease of the pancreas (PDP) is a rare condition. It can rarely occur independently but usually associated with polycystic kidney disease [9,10]. The prevalence of asymptomatic pancreatic cysts is estimated as 2.2% on CT-Scan and it is correlated with old age [11]. It has been reported in association with ADPKD in an elderly male [5]. PDP can be associated with other organs’ cysts including kidney and liver [10]. Management of both liver and pancreas cysts focused on symptomatic patients and includes aspiration, sclerosis and surgical excision and some cases may end with kidney and liver transplant [9,10].
Case presentation
A 47-year-old lady from Khartoum- Sudan, who is a mother of five sons and daughters, came complaining of right hypochondrial pain for eleven years. The pain was mild dull achy associated with upper abdominal swelling. No other symptoms referable to the other systems. On physical examination she was apparently fine and fit. Her pulse rate was 74 beats/min, regular and of good volume. Blood pressure was 115/80, liver is grossly enlarged. Renal function test (RFT), Liver function test (LFT), Thyroid function test (TFT) and complete blood count (CBC) were normal; Hemoglobin 12.9 gm/dL, Platelets 190000/cmm. Hepatitis viruses screening was negative. Percutaneous liver biopsy revealed benign cyst with no evidence of malignancy.
Ultrasound scan, CT-scan and MRI of the abdomen and pelvis (Figures 1 a-b) showed hugely enlarged liver with multiple different sizes cysts compatible with polycystic liver disease. Gallbladder is enlarged, contracted and packed with multiple stones. Normal pancreas with simple cyst. Normal kidneys with bilateral multiple different sizes simple- looking cortical cysts compatible with polycystic kidney disease.
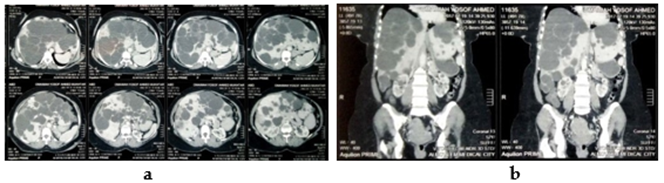
Figure 1: CT-Scan of the Abdomen (a and b) show multiple cysts in the Liver, Pancreas, and Kidneys.
Discussion
Cystic formation has variable effects on each organ. Polycystic disease of the kineys may end up with end stage renal failure. By the age of 70 years, half of the patients with ADPKD will require renal dialysis or transplant [7].
Polycystic disease of the pancreas is rare, and in general pancreatic cysts have been increased recently with different prevalence of asymptomatic pancreatic cysts [10, 11]. Surgery is indicated in cases of cysts which are rapidly increasing in size, symptomatic cysts, and in cases of advanced age [10].
This lady presented with multiple organs polycystic disease including kidney, liver and pancreas; which raised the suspicion of ADPKD [3,4,7,8]. Use of renin angiotensin aldosterone system (RAAS) is beneficial for uncontrolled hypertension associated with ADPKD [7].
Because of late discovery, and that her symptoms were not related to the pancreatic or renal cysts but to the liver and the symptoms were mild. Hence, she did not need any surgical intervention. She was already menopause; hence no preventive measures of family planning were used. She is lucky that none of her kids had the disease. In similar cases, patients may need counselling for scheduling their kids for early detection of the disease; as some complications are preventable!
Conclusion
Multiple organs polycystic disease is a rare condition. Each case has to be assessed and managed accordingly. Patients with organs function disturbances have to be followed up regularly with special attention that they may develop organ failure, mainly kidneys and liver, that may necessitate surgical intervention in form of organ transplant. Otherwise, patents need symptomatic treatment or no treatment at all.
References
- Bergmann C, Guay-Woodford L M, Harris P C, Horie S, Peters D J M, Torres V E. (2019). Polycystic Kidney Disease. NatRevDisPrimers, 4(1):50.
Publisher | Google Scholor - Neumann H P H, Jilg C, Bacher J, Nabulsi Z, Malinoc A, Hummel B, et al. (2013). Epidemiology of autosomal-dominant polycystic kidney disease: an in-depth clinical study for south-western GermanyNephrology and Allergic Transplantation, 28(6):1472-1487.
Publisher | Google Scholor - Abdul-Majeed S, Nauli S M. (2011). Polycystic Diseases in Visceral Organs. Obstet GynecolIntern.
Publisher | Google Scholor - Parminder K Judge, Charles H S Harper, Benjamin C Storey, et al. (Biliary Tract and Liver Complications in Polycystic Kidney Disease. JAmSocNephrol, 28(9):2738-2748.
Publisher | Google Scholor - Gupta R, Singh A K, Verma P, Mistry K, Pokharia P. (2018). Polycystic Disease of the Pancreas: A Case Report.JGastrointestDigSyst, 8(1):552.
Publisher | Google Scholor - Perrone R D. (1997). External Manifestation of ADPKD. Kidney International, 51:2022-2036.
Publisher | Google Scholor - Halvorson C R, Bremmer M S, Jacobs S C. (2010). Polycystic kidney disease: inheritance, pathophysiology, prognosis, and treatment. International Journal of Nephrology and Rheumatology, 3:69-83.
Publisher | Google Scholor - Sathialakshmi V, Swayam Jothi S, Saroja Sundararajulu, Kafeel Hussain A, Sree Lekha D, Rajeshwar Rao, N Sssmc, Ri. (2015). Cystic Diseases of the Organs. IOSR-JPBS, 10(1):13-16.
Publisher | Google Scholor - Cheung J, Scudamore C H, Yoshida E M. (2004). Management of Polycystic Liver Disease. Canadian Anjo Urnalofga Stroenterology, 18(11):666-670.
Publisher | Google Scholor - Sonavane A D Amarapurkar D N, Amarapurkar A D. (2016). Polycystic Pancread. ACG CaseReportsJournal, 3(3):199-201.
Publisher | Google Scholor - Zanini N, Giordano M, Cipolia d’Abruzzo G, et al. (2015). Estimation of the Prevalence of Asymptomatic Pancreatic Cysts in the Population of San Marino. Fakritology, 15(4):417-422.
Publisher | Google Scholor










