

Case Report
“Managing Class II Div I Malocclusion with Clear Path Aligners Utilizing an Extraction-Based Treatment Approach: A Case Report”
- Nasreen Nagani *
- Tayyaba Waqas
- Sara Masood
Consultant Orthodontist, Dent Correct Clinic Lahore, Pakistan.
*Corresponding Author: Nasreen Nagani,Consultant Orthodontist, DentoCorrect Clinic Lahore, Pakistan.
Citation: N. Nagani, T. Waqas, S. Masood. (2023). “Managing Class II Div I Malocclusion with Clear Path Aligners Utilizing an Extraction-Based Treatment Approach: A Case Report”, Dentistry and Oral Health Care, Biores Scientia Publishers, 2(4):1-7. DOI: 10.59657/2993-0863.brs.23.024
Copyright: © 2023 Nasreen Nagani, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 21, 2023 | Accepted: December 01, 2023 | Published: December 02, 2023
Abstract
This case report is based on the clear aligner treatment of an adult patient presented with class II div I malocclusion. The case was treated with the extraction of upper first premolars and interproximal reduction in the lower arch. Total 35 sets of upper aligners and 25 sets of lower aligners were delivered with the wear time of 22 hours per day for 10 days. The entire treatment course spanned a period of 14 months. Thus, the case study underscores the reliability of orthodontic treatment with clear aligners for addressing class II malocclusion. The discreet nature of these aligners not only enhances periodontal health but also increases patient acceptance. As a result, they are more likely to embrace and adhere to the treatment, fostering better overall outcomes.
Keywords: clear aligners; malocclusion; orthodontic treatment
Introduction
Malocclusion is a broad term that encompasses any malalignment of the teeth and jaws. It can be caused by a variety of factors, including genetics, environmental influences, and oral habits. Malocclusion can range in severity from mild to severe, and can have a significant impact on a person's appearance, oral health, and overall well-being [1]. Adults seek orthodontic treatment to improve their smile, occlusion, and psychological well-being [2,3]. However, traditional fixed appliances can be uncomfortable, expensive, and unaesthetic. This can deter some people from pursuing treatment, even though it may be necessary to improve their oral health and quality of life [4]. Clear aligners, like Invisalign®, are a series of removable plastic appliances that gradually move teeth into place. Clear aligners are virtually invisible, making them a popular choice for adults who are self-conscious about their appearance [5]. Clear aligners are worn for a certain period of time each day, and are gradually replaced with a new set of aligners as the teeth move into place [6]. Clear aligners have become increasingly popular in recent years due to advances in digital 3D technologies and dental materials [7,8]. Clear aligners can now be used to treat a wide range of malocclusion cases, including mild to moderate crowding, spacing, flaring, tipping, and relapse [9]. Over the course of time, the scope of cases addressed through the use of clear aligners has broadened, extending beyond simple orthodontic conditions to encompass more intricate issues like the correction of anterior open bite, bimaxillary protrusion, excessive facial height, and severe dental crowding [10,11,12]. Managing these cases often involves treatment plans that may include premolar extraction, introducing various challenges during the treatment process. These challenges may encompass issues such as posterior anchorage control and the preservation of post-treatment stability by ensuring root parallelism of the teeth neighboring the extraction sites [13,14]. This case report describes how clear aligners were used to correct Class II division I malocclusion in a patient's dentition. It documents the process, progress, and outcomes of this specific orthodontic treatment in addressing this issue. The report will likely include details about the treatment plan, how the clear aligners were applied, how the patient responded to the treatment, any challenges that were encountered, and ultimately, how successful the treatment was in resolving the malocclusion. This information can serve as a valuable resource for other practitioners and patients considering similar treatment for such malocclusions.
Case Report
A 26-year-old woman in good health sought our dental services, expressing concerns about her front teeth sticking out and crowding. Her medical history was largely unremarkable, and there were no reported family or dental issues. Upon extraoral examination, we noted a mesencephalic head shape, mesotrophic face form, symmetrical frontal view, convex profile, medium nose, and competent lips (figure:1). The interlabial gap was within the average range, and there were no reported symptoms or issues with the temporomandibular joint. During smile analysis, we observed adequate incisor display, but the teeth were not optimally aligned. The smile arc appeared harmonious. Intraoral examination revealed fair oral hygiene and an average periodontal status. Class II relationships were noted for both molars and canines, along with Class II div I incisors. The overjet was excessive at 6mm, while the overbite was 50%. Notably, the maxillary teeth midline deviated 1mm to the right of the patient's facial midline. Mild crowding was evident in the upper arch, and the lower arch showed moderate crowding. A panoramic radiograph confirmed a healthy periodontal condition without cavities, root resorption, or any dental abnormalities. Cephalometric analysis indicated a skeletal Class I relationship and a normo divergent facial pattern with proclined upper anteriors.
Treatment objectives
The primary objective of the orthodontic treatment was to address malocclusion using clear aligners. Secondary objectives encompassed achieving a sustainable, functional, and healthy bite, along with improving dental aesthetics. Correction of midline was not an objective.
Treatment options
We explored different treatment options with the patient, considering:
The first choice entailed traditional braces for orthodontic intervention, but the patient rejected this option as they favored a more aesthetically pleasing appliance. The second option involved the use of clear aligners, aligning with the patient's preference for a more aesthetic solution. In each of the treatment options, extraction of upper first premolars were planned with type B anchorage along with the interproximal reduction (IPR) in order to address the issues of proclined upper anterior, crowding and malalignment.
Treatment procedure
After history taking & examination, we proceeded to gather intraoral and extraoral photographs and polyvinyl silicone impressions. These collected records were transmitted to the Clear Path facility for the formulation of a customized treatment plan. The panoramic X-ray affirmed the presence of ample bone structure and showcased average oral hygiene, thereby meeting the essential criteria for orthodontic treatment. No further dental procedures were required, rendering the case suitable for the continuation of clear aligner treatment. After submitting the records, a 3D treatment plan was generated. This plan involved 35 stages in the upper and 25 stages in the lower arch. The case was treated with the bilateral extraction of upper first premolars and IPR in the lower arch. A treatment simulation (figure: 2) was presented to the patient for her review, and upon her satisfaction, approval was granted. The treatment plan was received and discussed with the patient within 7 days of the data submission. The patient expressed high levels of satisfaction with the proposed treatment plan, and no modifications were deemed necessary. A total treatment duration of 14 months was recommended to the patient, which she readily approved. Consequently, treatment commenced shortly thereafter.
IPR Technique
Interproximal reduction is a technique of carefully removing thin enamel layer interproximal between the neighboring teeth to unravel crowding [15]. There are different methods of IPR including burs, discs and abrasive strips [16]. In this study IPR was achieved using thin diamond coated double sided abrasive strip. It was measured using IPR gauge, followed by the application of topical fluoride to avoid any adverse effects.
EBT Technique
The elastic button technique (EBT) is a method used in clear aligner treatment to correct specific orthodontic problems. It involves attaching small buttons to certain teeth and using elastics to apply force between them. This force helps to move the teeth into the desired position [17]. In this case, stainless steel buttons were bonded onto the buccal surfaces of the upper canines and first molars, thus facilitating reciprocal movements to achieve the space closure.
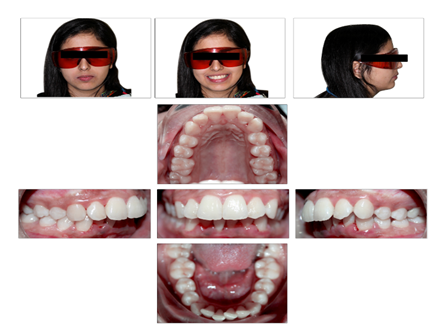
Figure 1: Pretreatment extraoral & intraoral photographs.

Figure 2: 3D treatment plan (a) Before & After, (b) Superimpositions.
Treatment progress
After approval of the treatment simulation in the Clin Check, we received the IPR and MRF forms (figure:3 and 4) from the aligner facility, along with 35 sets of upper and 25 sets of lower aligners. The recommended wear time for each set was 22 hours per day for ten days. The patient received comprehensive guidance on oral hygiene and periodontal health. Initially, the patient was provided with the first set of aligners and was scheduled for an IPR appointment before starting the second set. IPR was performed in the lower arch at five points, reducing 0.6mm between the premolars bilaterally and 0.6mm between the lateral and central incisors bilaterally. 0.6mm was also reduced from the lower second premolar and first molar on the left side. Subsequently, the patient received the next sets of aligners and was evaluated for periodontal health and aligner tracking every three months, with satisfactory results. The extraction of upper first premolars was done with the placement of buttons on the upper canines and molars bilaterally before providing the next batch of aligners. 3/16 elastics (medium) were recommended with a wear time of 18 hours to achieve type B anchorage with reciprocal movements. The patient demonstrated good compliance, and the treatment was successfully completed. Following the treatment, two sets of retainers were issued. The patient was instructed to wear them full time for the first six months, followed by night-time wear for three months, and then alternate-night-time wear for the remaining three months.
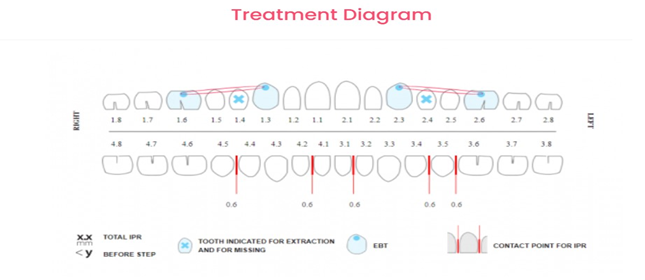
Figure 3: IPR form
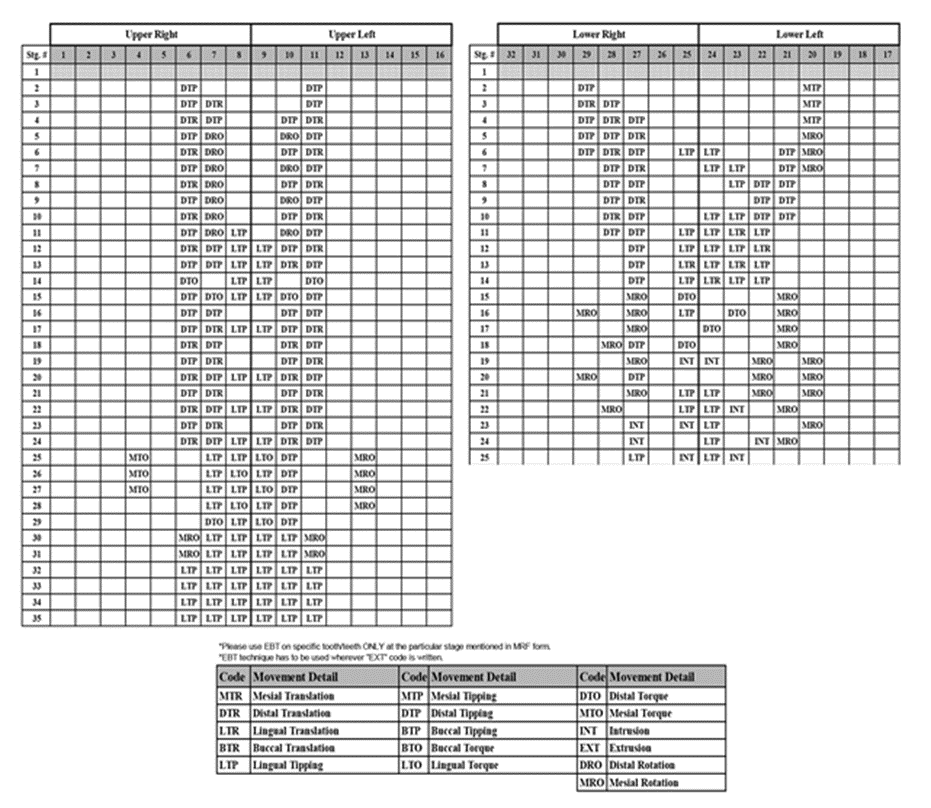
Figure 4: Movement Record Form
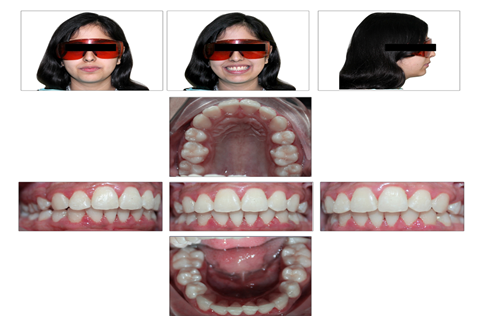
Figure 5: Post treatment records; extra oral and intra oral photographs.
Treatment Result
The entire treatment course spanned a period of 14 months, with each aligner being worn for a substantial 22 hours per day and replaced every 10 days. By the conclusion of this treatment, the initial crowding issues and proclination of upper anterior teeth were successfully addressed, leading to the establishment of class II molar and class I canine relationships. The result was an achievement of an ideal overjet and overbite, ensuring proper alignment and bite function (figure: 5). Furthermore, the treatment concluded with the harmonious centering of the maxillary and mandibular arches, enhancing both the esthetic and functional aspects of the patient's smile. Importantly, the periodontal health was carefully maintained throughout the treatment, with no evidence of gum recession or the formation of periodontal pockets, ensuring the overall well-being of the patient's oral health.
Discussion
The aim of this study was to evaluate the reliability of clear aligners in the treatment of class II div I malocclusion using extraction-based approach. Class II Division I malocclusion is a specific type of dental malalignment classified within the field of orthodontics. This malocclusion is characterized by a prominent upper jaw and protruding upper front teeth relative to the lower front teeth. The features of Class II Division I malocclusion include an increased overjet, where the upper front teeth are positioned significantly forward in relation to the lower front teeth, and a deep overbite, where the upper front teeth excessively overlap the lower front teeth vertically. In this specific case involving class II div I malocclusion and moderate crowding, clear aligners were successfully employed over a duration of 14 months. Extraction of upper first premolars were done to retract the anterior teeth utilizing type B anchorage plan. Crowding was alleviated through a combination of arch expansion and interproximal reduction in the lower arch. A total of 35 sets of aligners were provided for the upper and 25 sets for lower arch. While alternative treatment options were presented to the patient, they opted for clear aligners due to their discreet, hygienic, and comfortable nature. Clear aligners represent a unique treatment approach for adult orthodontic patients, addressing aesthetic, hygiene, and metal allergy concerns while offering a treatment duration comparable to traditional fixed appliances [18]. In clear aligner treatment, patient compliance is of paramount importance. Patient education can serve as a motivational tool, influencing patient acceptance of the appliance and improving compliance [19]. In this case, the patient's active involvement and interaction with their orthodontist significantly contributed to the treatment's success. The patient was engaged with the CLIN Check software, which visually demonstrated the anticipated tooth movement and progress throughout the treatment. This underscores the value of CLIN Check as an educational tool to illustrate the final treatment objectives to the patient. However, it is worth noting that the clear aligner system does have certain limitations. It may be less predictable in cases involving severe derotations, complex extrusions, or significant translations, which might necessitate additional treatment modalities [18]. Despite potentially higher laboratory fees compared to conventional appliances, the virtual treatment setup, ease of use, and high patient acceptance can often offset the additional cost. This setup not only aids in diagnosis but also serves as an educational tool for patients. Furthermore, patient cooperation is crucial for the overall success of the treatment, which, in this case, was excellent due to the patient's enthusiasm for the process.
Conclusion
In summary, this case study underscores the reliability of orthodontic treatment with clear aligners for addressing class II div I malocclusion. The discreet nature of these aligners not only enhances periodontal health but also increases patient acceptance. Moreover, the precise control of orthodontic movements, with minimal risk of losing anchorage, makes it a compelling option for clinicians when managing moderate crowding cases.
Consent & Conflict of Interest
A written consent form was signed from the patient for use of the dental records for publications & social media marketing. Also, there is no conflict of interest with this paper.
References
- Johal A, Joury E. (2015). What factors predict the uptake of orthodontic treatment among adults? Am. J Orthod Dentofacial Orthop, 147:704-10.
Publisher | Google Scholor - Jaber ST, Hajeer MY, Burhan AS, Latifeh Y. (2022). The effect of treatment with clear aligners versus fixed appliances on oral health-related quality of life in patients with severe crowding: a one-year follow-up randomized controlled clinical trial. Cureus, 14.
Publisher | Google Scholor - Mousa MM, Al-Sibaie S, Hajeer MY. (2023). Pain, discomfort, and functional impairments when retracting upper anterior teeth using two-step retraction with Transpalatal arches versus en-masse retraction with miniimplants: a randomized controlled trial. Cureus, 15:33524.
Publisher | Google Scholor - Oliveira PG, Tavares RR, Freitas JC. (2013). Assessment of motivation, expectations a satisfaction of adult patients submitted to orthodontic treatment. Dental Press J Orthod, 18:81-87.
Publisher | Google Scholor - Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. (2015). Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod, 85:881-889.
Publisher | Google Scholor - Hajeer MY, Millett DT, Ayoub AF, Siebert JP. (2004). pplications of 3D imaging in orthodontics: part I. J Orthod, 31:62-70.
Publisher | Google Scholor - Hajeer MY, Millett DT, Ayoub AF, Siebert JP. (2004). Applications of 3D imaging in orthodontics: part II. J Orthod, 31:154-62.
Publisher | Google Scholor - Jaber ST, Hajeer MY, Khattab TZ, Mahaini L. (2021). Evaluation of the fused deposition modeling and the digital light processing techniques in terms of dimensional accuracy of printing dental models used for the fabrication of clear aligners. Clin Exp Dent Res, 7:591-600.
Publisher | Google Scholor - Pithon MM, Baião FC, Sant Anna LI, Paranhos LR, Cople Maia L. (2019). Assessment of the effectiveness of invisible aligners compared with conventional appliance in aesthetic and functional orthodontic treatment: a systematic review. J Investig Clin Dent, 10: e12455.
Publisher | Google Scholor - Harris K, Ojima K, Dan C, et al. (2020). Evaluation of open bite closure using clear aligners: a retrospective study. Prog Orthod, 21:23.
Publisher | Google Scholor - Jie RLK. (2018). Treating bimaxillary protrusion and crowding with the invisalign G6 first premolar extraction solution and invisalign aligners. APOS Trends in Orthodontics, 8:219.
Publisher | Google Scholor - Gaffuri F, Cossellu G, Lanteri V, Brotto E, Farronato M. (2020). Comparative effectiveness of Invisalign and fixed appliances in first-premolar extraction cases. J Clin Orthod, 52:294-301.
Publisher | Google Scholor - Kim TK, Kim JT, Mah J, Yang WS, Baek SH. (2005). First or second premolar extraction effects on facial vertical dimension. Angle Orthod, 75:177-182.
Publisher | Google Scholor - Oshagh M, Danaei SM, Sardarian A, Alipour A, Roeinpeykar M, Khaksar Y. (2014). Root parallelism of canine and second premolar in preadjusted and standard edgewise systems: a comparative study. Galen Med J, 3:176-181.
Publisher | Google Scholor - Meredith L, Li M, Cannon RD, Farella M. (2017). Interproximal reduction in orthodontics: why, where, how much to remove? Aust Orthod J, 33(2):150.
Publisher | Google Scholor - Lapenaite E, Lopatiene K. (2014). Interproximal enamel reduction as a part of orthodontic treatment. Stomatologija, 16(1):19-24.
Publisher | Google Scholor - Natnicha Pariyatdulapak, Pornkiat Churnjitapirom, Toemsak Srikhirin & Nita Viwattanatipa (2021) Bond strength of orthodontic buttons on clear aligner materials. Orthodontic Waves, 80:4:224-231.
Publisher | Google Scholor - RL Boyd, RS Miller, V Vlaskalic. (2020). The Invisalign system in adult orthodontics: mild crowding and space closure cases. J Clin Orthod, 34:203-213.
Publisher | Google Scholor - HG Sergl, U Klages. (1998). A Zentner Pain and discomfort during orthodontic treatment: causative factors and effects on compliance. Am J Orthod Dentofacial Orthop, 114:684-691.
Publisher | Google Scholor












