

case report
Laparoscopic Cholecystectomy in a Patient with Situs Inversus Totalis: Review of the Surgical Technique
1Resident Physician General Surgery Service of the Víctor Lazarte Echegaray Base Hospital, Peru.
2Assistant physician of the General Surgery Service of the Víctor Lazarte Echegaray Base Hospital, Peru.
*Corresponding Author: Roger Leon Fernandez, Resident Physician General Surgery Service of the Víctor Lazarte Echegaray Base Hospital, Peru.
Citation: Roger L Fernandez, Walter C Inolopu, L.E.M. Huallanca. (2023). Laparoscopic Cholecystectomy in a Patient with Situs Inversus Totalis: Review of the Surgical Technique. International Journal of Medical Case Reports and Reviews, BRS Publishers. 2(4); DOI: 10.59657/2837-8172.brs.23.026
Copyright: © 2023 Roger Leon Fernandez, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 26, 2023 | Accepted: July 18, 2023 | Published: July 29, 2023
Abstract
Objective: To present a patient with situs inversus totals and symptomatic cholelithiasis treated by laparoscopy, highlighting the usefulness of minimally invasive surgery in patients with anatomical variants. Background: Situs Inversus Totalism is a rare genetic disorder that is characterized by the transposition of the thoracoabdominal organs in a sagittal direction, providing a so-called “mirror” image. Methods: Report of a 40-year- old female patient with symptomatic cholelithiasis of 3 months evolution, in whom situs inversus totals was identified, after imaging tests performed. The intervention proceeded without complications and the patient was discharged after 24 hours. Conclusions: Gallbladder lithiasis in situs inversus totals is a rare clinical condition that can be treated safely and effectively by laparoscopy. We believe that an exhaustive preoperative study is convenient to detect possible added anatomical variants in these patients, since their knowledge can help us to design the operation.
Keywords: situs inversus totals; laparoscopic cholecystectomy; surgery; anatomical variant
Introduction
Situs inversus is a rare autosomal recessive inheritance anomaly (1 / 10,000-20,000 cases) in which the thoracic or abdominal organs are inverted and symmetrical to their normal position.1 It was first described by Aristotle in animals and the first case in humans was published by Fabricius in the seventeenth century. 2,3 It can be total or partial depending on whether or not it is associated with dextrocardia. It is normally asymptomatic and can be accompanied by hepatic, cardiac, intestinal and vascular anatomical alterations, such as the absence of the vena cava, which are present in almost 80% of patients with this entity. In 25% of cases, it presents as part of Kartagener syndrome, also characterized by the presence of recurrent bronchiectasis and sinusitis. 4,5 The morbidity and mortality of surgical treatment of cholelithiasis is similar to that of other patients without this alteration. There are other anatomical abnormalities in which the gallbladder is on the left side of the body. It is called interposition when the gallbladder is located on the left side of the round ligament and below the left hepatic lobe without situs inversus [6,7]. The incidence of gallstones does not differ from that published for the general population. For these reasons, in the world literature, there are only case reports that combine patients with situs inversus totals who underwent cholecystectomy for symptomatic gallstones. The first laparoscopic cholecystectomy (LC) in SI was attributed to Campos and Sipes in 1991 [8]. Since then, the number of published cases is estimated to be less than 100, with the finding of malposition, duplication or bifurcation of the cystic artery being relatively frequent in many [9]. During laparoscopic cholecystectomy, in patients with orthotopic gallbladder or situs solidus (usual location of intra-abdominal organs) [10]. The surgeon's left hand generally handles the instrument inserted through the right subcostal portal, with which the traction maneuvers are performed. and mobilization of the gallbladder, and the right hand manipulates the instrument introduced through the subxiphoid port, with which the dissection and section of the different anatomical structures is carried out. Changes in the position of the intra-abdominal organs generate changes in the approach or in the laparoscopic surgical technique [11].
Clinical case
This is a 40-year-old female patient, operated on for open appendectomy 3 years ago, who consulted for pain in the epigastrium and left hypochondrium of colic type of 14 days of evolution, intermittent, associated with the consumption of fatty foods. Physical examination revealed pain on deep palpation of the epigastrium and left hypochondrium, without visceromegaly or peritoneal irritation, negative Murphy. Abdominal ultrasound confirmed the clinical suspicion of chronic lithiasic cholecystopathy without acuity criteria and the alteration in the distribution of intra-abdominal organs. During the pre- operative protocol, a contrasted thoracic-abdominal-pelvic tomography was performed, which documented situs inversus totalis and gallstones (Figures 1 and 2). Laboratory results reported liver function testes without alternation
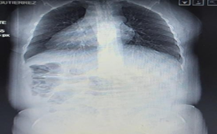
Figure 1: Situs inversus totalis radiography.
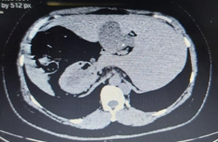
Figure 2: Situs inversus totalis tomography.
The patient was scheduled for elective LC two months after admission. The intervention was performed under general anesthesia, in the American and Fowler position. Umbilical approach with Hasson technique. Pneumoperitoneum with CO2 up to 12 mmHg. 10mm umbilical port placement and 30° camera introduction. The main surgeon was located on the left side of the patient. Stomach and liver were found in reverse position, the gallbladder in segment III of the liver, with the body and fundus adjacent to the falciform ligament (figure 3), then adding an ectopia vesicular. When the patient was placed in Fowler's position and side 15 degrees to the right, the handles were moved in order to clear the work area. The remaining ports were placed as follows (Figure 4): P2 in the left subcostal region, P3 in the left flank and P4 in the right flank, the left hypochondrium port was used for dissection and the assistant used P4 for fundus retraction. vesicular. Upon obtaining the critical safety view, it was observed that the cystic artery was located anterior to the cystic duct (figure 5), the cystic duct was ligated in two strands and the cystic artery was electrofulgurated (figure 6), gallbladder ectomy and extraction were performed. of the piece according to the usual technique. It is worth mentioning that the dominant hand of the surgeon was the right. The operative time was 60 minutes. The patient evolved favorably, tolerated a soft diet after 6 hours and was discharged from hospital after 24 hours without any complications.

Figure 3: The gallbladder in segment III of the liver, with the body and fundus adjacent to the falciform ligament.

Figure 4: Ports placement.

Figure 5: Dissection of the triangle of Calot.

Figure 6: The cystic duct was ligated in two strands and the cystic artery was electro fulgurated.
Discussion
The surgical technique of laparoscopic cholecystectomy in patients with orthotopic gallbladder or situs solitus has been described in such a way that the surgeon's right hand, located on the left side of the patient, is the one that manipulates the instrument introduced through the subxiphoid portal, with which the anterior leaf of the hepatoduodenal ligament is accessed perpendicularly during the dissection of the elements of Calot's triangle. For laparoscopic cholecystectomy, in the patient described, it was initially thought to place the trocars in "mirror image"; however, due to gallbladder ectopia (gallbladder in segment III) in addition to its situs inversus condition, the subxiphoid port was relocated to the right flank. With the latter, we were able to introduce the instrument for gallbladder fundus traction to the right, and use the ports on the left side for gallbladder mobilization and dissection. It should be noted that the surgeon was located on the left side of the patient. Although the angle of incidence of the working instruments on the elements of Calot's triangle was modified, there was no change in the visual field or greater difficulty in performing the surgical technique (dissection, cutting or coagulation maneuvers). Multiple studies report cases in which 4 trocars are used: the 10mm umbilical optical port, one subxiphoid for gallbladder dissection, one in the left hypochondrium for mobilization, and one in the left flank for the assistant. In cases in which the surgeon was left-handed and positioned on the patient's right side, he used the subxiphoid port to dissect and the left hypochondrium port to mobilize Hartman's bursa [12,13,14]. Other studies report cases in which, using 4 trocars, the surgeon is right-handed and positioned on the right side, performs the cholecystectomy using the left hypochondrium trocar as the working port, and the assistant pulls through the left flank port [15,16]. Most studies place the patient in the American position, only one describes the French position for its execution, mentioning that it is more comfortable for right-handed surgeons, when using the left hypochondrium port for dissection and cut [17]. The operative time of 60 minutes was the same as in those case reports that describe it in their operative technique [18,19]. Our case report coincides with many others, with hospital discharge at 24 hours of hospitalization, some case reports extend hospital discharge up to 48 hours post intervention. There are no reports of complications in any of them so far. No cases have been reported in which situs inversus totals and gallbladder ectopia coexist at the same time, increasing the complexity of the case, although placing the gallbladder in a position in which the surgeon feels more comfortable working on the left side, as in the usual way.
Conclusion
There is no established technique for performing laparoscopic cholecystectomy in patients with situs inversus totals. In the present case we use four ports, using the working port in the left hypochondrium. We always recommend respecting the anatomical guidelines for the laparoscopic approach and following the surgery step by step to obtain the critical view. In the case described, the different anatomical variations did not alter the surgical result or the postoperative evaluation of the patient
References
- Morris PJ, Malt RA, eds. (1949). Oxford Textbook of Surgery. New York: Oxford University Press.
Publisher | Google Scholor - Wood GO, Blalock A. (1940). Situs inverse totalis and disease of the biliary tract: survey of the literature and report of a case. Arch Surg, 40:885-896.
Publisher | Google Scholor - Mayo CW, Rice RG. (1949). Situs inversus totalis: a statistical review of data on seventy-six cases with special reference to disease of the biliary tract. Arch Surg, 58:724-730.
Publisher | Google Scholor - Kobus C, et al. (2003). irugía laparoscópica y situs inversus. Revisión de la literatura y presentación de un caso de sigmoidectomía por diverticulitis. Cir Esp, 73:381-384.
Publisher | Google Scholor - Echavarri A. et al. (2004). Colecistectomía por laparoscopía en un paciente con situs inversus total. Reporte de un caso. Rev Esp Med Quir 2004; 9:61-67.
Publisher | Google Scholor - Nguyen T., et al. (2018). Sinistroposition: a case report of true left side gallblader in a Vietnamese patient. Int J Surg Case Reports. 51:82-85.
Publisher | Google Scholor - Abongwa H., et al. (2017). Implications of left sided gallblader in the emergency setting: retrospective review and top tips for safe laparoscopic cholecystostomy. Surg Laparosc Endosc Percutan Tech. 27:220-227.
Publisher | Google Scholor - Campos L, Sipes E. (1991). Laparoscopic cholecystectomy in a 39-year-oldfemale with situs inversus. J Laparoendosc Surg, 1(2):123-136.
Publisher | Google Scholor - Alsabek MB, Arafat S, Aldirani A. (2016). A case report of laparoscopic cholecystectomy in situs inversus totalis: Technique and anatomical variation. Int J Surg Case Reports, 28:124-126.
Publisher | Google Scholor - Fulcher AS, Turner MA. (2002). Abdominal manifestations of situs anomalies in adults. Radiographics, 22:1439-1456.
Publisher | Google Scholor - Aydin U, Unalp O, Yazici P, Gurcu B, Sozbilen M, Coker A. (2006). Laparoscopic cholecystectomy in a patient with situs inversus totalis. World J Gastroenterol, 12:7717-7719.
Publisher | Google Scholor - AlKhlaiwy O. et al. (2019). Laparoscopic cholecystectomy in situs inversus totalis: case report with review of techniques. Int J Surg Case Reports, 59:208-212.
Publisher | Google Scholor - Alam A. et al. (2017). Laparoscopic cholecystectomy in a case of situs inversus totalis: a review of technical challengues and adaptations. Ann Hepatobiliary Pancreat Surg, 21:84-87.
Publisher | Google Scholor - Ren J. et al. (2017). Modified laparoscopic cholecystectomy technique for treatment of situs inversus totalis: a case report. J Int Med Res. 45:1261-1267.
Publisher | Google Scholor














