

Research Article
Knowledge Attitudes and Practices in Ergometry Among Nurses at the Bafoussam Regional Hospital
- Fondop Joseph 1
- Atemkeng Tsatedem Faustin 1
- Lydia Auriane Kos A Kitouk 1
- Atyam EKOTO Marie christisme 2
- Banga ND 1
- Dikongue Dikongue Fred 1
- Amougou Boris 1
- Djam C. Alain 1*
- Dogmo Arlette 1
- Djientcheu Vincent de Paul 3
- Fuentes Stéphane 4
1Faculty of Medicine and Pharmaceutical Sciences, University of Dschang, Cameroon.
2Dschang Regional Annex Hospital, Cameroon.
3Yaounde General Hospital, Cameroon.
4Timone Adult University Hospital, Marseille, Cameroon.
*Corresponding Author: Djam C. Alain, Faculty of Medicine and Pharmaceutical Sciences, University of Dschang, Cameroon.
Citation: Joseph F, Atemkeng T Faustin, L.A.K.A. Kitouk, Christisme A E M, Djam C. Alain, et al. (2023). Knowledge Attitudes and Practices in Ergometry Among Nurses at the Bafoussam Regional Hospital, Journal of Clinical Research and Clinical Trials, BioRes Scientia publishers. 2(3):1-7. DOI: 10.59657/2837-7184.brs.23.014
Copyright: © 2023 Djam C. Alain, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 24, 2023 | Accepted: August 07, 2023 | Published: August 28, 2023
Abstract
Occupational medicine was born in France after the First World War and gradually the range of occupational diseases and accidents widened. Today, the community is concerned about the well-being of the workplace, and thinks in terms of occupational health. Major surveys identify not only the physical but also the psychological state of health of employees. Nurses are particularly a population at risk because of their often-morbid working conditions. The objective of our study was to raise awareness and show the importance of ergonomics by assessing practical knowledge and attitudes in ergonomics among nurses. To this end, a descriptive cross-sectional study was conducted from March 15 to June 20 at the Regional Hospital of Bafoussam (HRB) on sample of 110 nurses. A face-to-face questionnaire was administered for data collection. The data collected was analyzed by software Epi Info 7.2.2.7 and presented in table and graph form. In total, of the 110 nurses surveyed, 58, 18% [CI: 48, 39%- 67, 52%] (64/110) had a poor level of knowledge in ergonomics. 74, 55% [CI: 65, 35- 82, 37%] (82/110) had harmful ergonomic practices. 57, 27% [CI: 47, 48- 66, 66%] (63/110) suffered from musculoskeletal disorders. Ergonomics practices were significantly associated with the musculoskeletal disorders at the nurse of the Bafoussam Regional Hospital [OR: 3, 07; CI: 1, 13% - 10, 04%; P= 0,028].
Ergonomics practices are not well known in the nursing profession, and nurses need training to improve performance and reduce the occurrence of occupational accidents.
Keywords: ergonomics; knowledge; nurses; HRB
Introduction
Working conditions encompass three orientations, namely ergonomic organisation, i.e. the adaptability of an individual to work, the conditions themselves, and hygiene and health [1,2]. According to the International Ergonomics Association (IEA), ergonomics is the scientific discipline that aims at the fundamental understanding of the interactions between human beings and the components of a system, and the implementation in design of relevant theories, principles, methods and data in order to improve human well-being and the overall efficiency of systems. Furthermore, it is a discipline that is nowadays applied to all aspects of human activity [3]. Poor posture reduces the efficiency of movement and sometimes leads to injury. If maintained for too long at a workstation, poor posture leads to persistent back pain and sometimes even spinal deformity. Caregivers are a key population for ergonomic intervention studies. They are numerous, their risk of injury is high and the risk factors are relatively well known. In the United States and most other industrialised countries, the rate of low back pain and other musculoskeletal disorders (MSDs) among nurses and other categories of caregivers is very high. According to US statistics on reported cases of MSDs, healthcare occupations are among the few occupations in the US with the highest accident incidence rate and absolute number of accidents. The healthcare sector is also characterised by rapid organisational change, high economic pressure and increasing workloads in many countries. The first recognised risk factor for work-related MSDs among carers is patient handling. Indeed, lifting or transferring patients must be done several times a day. This handling is stressful: the patients are heavy, many of them weigh more than 100 kg, they are in an awkward position for lifting and transferring and may struggle during the transfer [4]. The objective of this study was to evaluate the knowledge and practical attitudes of nurses at the Bafoussam Regional Hospital in ergometry in order to prevent or minimise work-related musculoskeletal disorders during the administration of nursing care.
Methodology
This was a descriptive cross-sectional study by collecting data during the period from 15 March to 20 June 2020 at the Bafoussam Regional Hospital (HRB). The HRB is located in West Cameroon. This health facility has several departments including: reception, security, radiology, maternity, paediatrics, surgery, physiotherapy, internal medicine, neuropsychiatry, hepato-gastroenterology, emergency, nutrition, diabetology, cardiology, gynaeco-obstetrics, morgue, pharmacy and the administrative block. The 224 nurses working at the HRB who gave their consent constituted our study population. Any staff working at the HRB who were not nurses, any nurses who refused to participate in the study and any cases of drop-out were excluded from the study.
Our sample size was non-exhaustive. The sampling method adapted to the study was non-probability. All nurses interested in the study were asked to complete a questionnaire. For data collection, we used mainly three tools: 1) A questionnaire designed by the principal investigator and pre-tested for validity and composed of 23 questions divided into 4 parts, namely: part A containing socio-demographic characteristics, parts B and C assessing knowledge and practical attitudes on ergonomics and part D which identified musculoskeletal disorders related to poor ergonomic attitudes
After the collection phase, each questionnaire was coded according to the order of arrival of the responses. The data was processed anonymously and collated
With regard to the level of knowledge, each of the 5 questions on respondents' knowledge was rated out of 2 for a total score of 10. The level of knowledge according to the score was assigned as follows:
- Less than 50% correct answers = Low;
- Less than 65% correct answers = Insufficient;
- Less than 85% correct answers = Average;
- More than 85% correct answers = Good [5].
With regard to the participants' level of practice, each of the 5 questions was rated out of 2 for a total score of 10. The level of practice according to the total score was assigned in three levels (harmful, inadequate, adequate) [5].
The data were analysed using Epi Info version 7.2.2.7 and represented in tables and graphs using Excel and Word 2013. This study respected ethical considerations such as: Social value, Scientific value, Confidentiality, Risks and avoidance measures, Benefits. The required administrative procedures were followed.
Results
During the data collection, we sampled 128 nurses, 110 of whom agreed to participate in the study, i.e., a participation rate of 85.93% and a non-response rate of 14.07%.
Socio-demographic characteristics
- Of the 110 nurses surveyed, 85 were female and 25 were male.40.91% (45/110) of the participants were aged between [21-30], 49.09% (54/110) between [31-40], 9.09% (10/110) between [41-50] and 0.91% (1/110) of the participants between [51-60].
- 64% (16/25) of men were single, 36% (9/25) were married. 44.71% (38/85) of the women were single, 54.12% (46/85) were married and 1.17% (1/85) were widowed.
- 34.55% (38/110) of the participants had a normal BMI, 44.55% (49/110) were overweight, 15.45% (17/110) were obese class I, 4.55% (5/110) were obese class II and 0.90% (1/110) were obese class III.
16.36% (18/110) of the participants worked in surgery, 12.73% (14/110) in emergency, 11.82% (13/110) in diabetes, 10.91% (12/110) in neuropsychiatry, 9.09% (10/110) in cardiology, 9.09% (10/110) in pediatrics, 8.18% (9/110) in gastroenterology, 5.45% (6/110) in general medicine, 5.45% (6/110) in internal medicine, 4.55% (5/110) in neonatology, 4.55% (5/110) in maternity, 1.82% (2/110) in gynaecology and obstetrics (Figure 1).
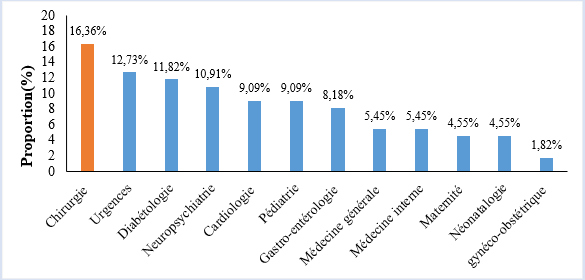
Figure 1: Distribution of the population by service.
- 41.82% (46/110) of respondents had heard of ergonomics, compared to 58.18% (64/110) who said they had never heard of it.
- 36.36% (40/110) of the participants knew what is called ergonomics against 63.64% (70/110) who did not,
- 39.09% (43/110) of the participants said they knew that ergonomics was beneficial to their job, while 60.91% (67/110) thought it was not.
- 35.45% (39/110) of the participants said that poor ergonomics had an impact on health, while 64.55% (71/110) thought that it did not have an impact on health.
- Depending on the department, 83.33% of the participants working in the internal medicine department had a good level of ergonomic knowledge, while participants working in the gynaecological-obstetrics, gastroenterology and maternity departments had no knowledge at all (Figure 2).
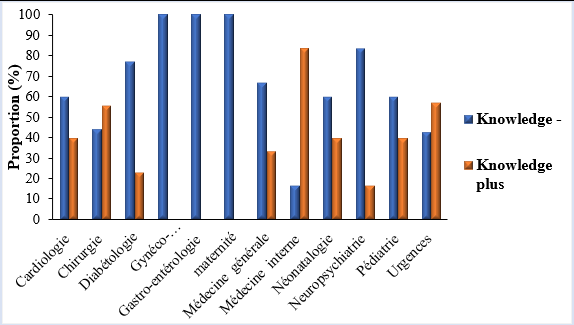
Figure 2: Distribution of the level of knowledge according to the services.
For the knowledge of ergonomics by nurses, 28.18% (31/110) of the participants had a good level; 8.18% (9/110) had an average level, 5.45% (6/110) had an insufficient level and 58.19 (64/110) had a poor level (Table 1).
Table 1: Distribution of the population according to the level of knowledge of ergonomics.
| Knowledge level Ergonomics | Frequencies(n) | Percentage (%) | 95% CI |
| Good | 31 | 28,18 | 20,02 - 37,56 |
| Medium | 9 | 8,18 | 3,81 - 14,96 |
| Insufficient | 6 | 5,45 | 2,03 - 11,49 |
| Bad | 64 | 58,19 | 48,39 - 67,52 |
| Total | 110 | 100 |
Description of the practical attitudes of HRB nurses in ergonomics
During the administration of care, 16.36% (18/110) adopted a sitting posture to administer care, 36.36% (40/110) had a bent posture and 47.28% (52/110) had a standing forward leaning posture (Table 2).
Table 2: Distribution of the population according to the posture adopted during care.
| Posture during care | Frequencies(n) | Percentage (%) | 95% CI |
|---|---|---|---|
| Sitting | 18 | 16,36 | 10,00 - 24,62 |
| Curved | 40 | 36,36 | 27,40 - 46,08 |
| Standing bent over | 52 | 47,28 | 37,68 - 57,02 |
| Total | 110 | 100 |
- While filling out the charts, it was found that: 34.55% (38/110) of the participants adopted a standing posture to fill out the patients' charts, 47.27% (52/110) adopted a forward-leaning sitting posture, 4.55% (5/110) were bent over, and 13.64% (15/110) sat with their trunk at 90°.
- For heavy lifting 68.18% (75/110) of the participants carried the heavy loads in a bent position, 25.45% (28/110) had bent knees and 6.36% (7/110) were in a straddle position.
- The distribution of the level of practice of ergonomics is different from one department to another, the staff of the paediatric department has the best knowledge (40%) and those working in the gynaecological-obstetric, maternity, neuro-psychiatric and emergency departments had a poor knowledge (Figure 3).
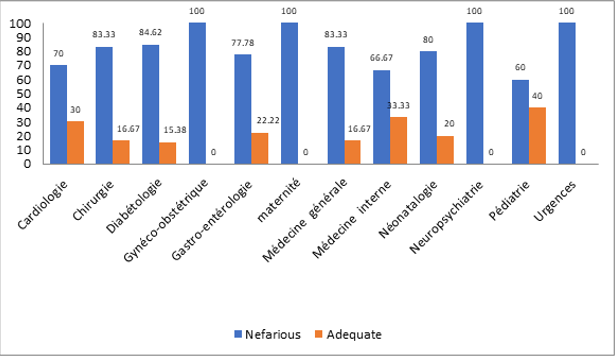
Figure 3: Distribution of the level of ergonomics practice by service.
For the HRB nurses' practice in ergonomics: it is found that 2.73% (3/110) of the nurses had an adequate level of practice in ergonomics, 22.73% (25/110) had an inadequate level, and 74.55% (82/110) had an adverse level (Table 3).
Table 3: Distribution of the population according to the level of practice in ergonomics.
| Level of practice | Frequencies(n) | Percentage (%) | 95% CI |
| Suitable | 3 | 2,75 | 0,57 - 7,76 |
| Inadequate | 25 | 22,7 | 15,28 - 31,70 |
| Nefarious | 82 | 74,55 | 65,35 - 82,37 |
| TOTAL | 110 | 100 |
According to the services, the frequency of Musculoskeletal Disorders (MSD) per service is: 15.87% versus 15.91% of surgical staff had MSDs while only 9.52% out of 18.18% of participants working in the emergency department did not have them. The same is true for the gastroenterology department where only 4.76% of patients had them (Figure 4).
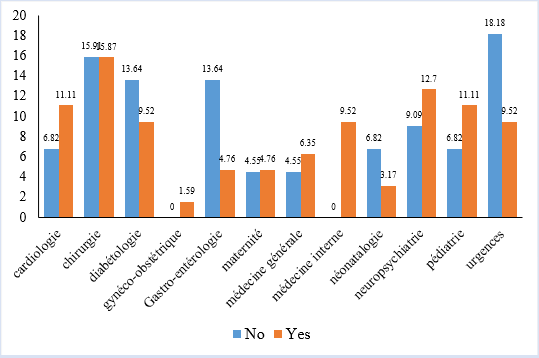
Figure 4: Distribution of MSD occurrence by service.
The frequency of occurrence of MSDs in the total population indicates that 57.27% (63/110) of participants had MSDs and 42.73% (47/110) did not.
Association between level of ergonomic knowledge and musculoskeletal disorders: according to the table below, there is no association between the level of knowledge and the occurrence of musculoskeletal disorders among nurses in the HRB [OR= 1.04; CI: 0.46% - 2.22%; P-Value = 0.486] (Table 4).
Table 4: Relationship between level of knowledge and MSD occurrence.
| Variables | Musculoskeletal disorders | Total | OR (95% CI) | P-Value | ||
|---|---|---|---|---|---|---|
| Yes | Not | |||||
| Level of knowledge | Good | 23(20,21%) | 40(36,36%) | 63(56,57%) | 1,0147 (0,4626-2,2259) | 0,486 |
| Bad | 17(13,43%) | 30 (30%) | 47(43,43%) | |||
| Total | 40(33,64%) | 70(66,36%) | 110(100%) | |||
Association between ergonomic practices and musculoskeletal disorders shows that [OR=3.07; CI:1.13% -10.04%; P-Value=0.028] would be significantly associated with musculoskeletal disorders among nurses in the HRB.
Table 5: Relationship between ergonomic practices and MSD occurrence.
| Variables | Musculoskeletal disorders | Total | OR (95% CI) P-VALUE² | P-Valu²e² | ||
| Yes | No | |||||
| Ergonomic practices | Adequate | 14(12,72%) | 4(3,65%) | 18(16,37%) | 3,0714 (1,1266- 10,0385)0,028 | 0,028 |
| Nefarious | 49(44,54%) | 43(39,09%) | 92(83,63%) | |||
| Total | 57,26% | 42,74% | 110(100%) | |||
Discussion
A total of 110 nurses were included out of which 85 (77.27%) were female and 25 (22.73%) were male with a sex ratio M/F of 0.29 which is contrary to the study conducted by Rakhshaan K et al. in Pakistan in which male predominance was observed (210/344) 61.04% [6]. Nurses are more represented by female gender in the hospital in the same proportions. The most represented age group was 31-40 years with 54/110 (49.01%) participants. Regarding marital status, 55/110 (50%) were married and 49/110 (44.55%) were overweight.
Regarding the knowledge of ergonomics by the HRB nurses, 46/110 (41.82%) participants had heard of ergonomics and 40/110 (36.36%) had knowledge of ergonomics which is in contrast to the study conducted by Rakhshaan K et al [6] in which 179/344 (52%) of the population had heard of ergonomics and 316/344 (92%) had knowledge of ergonomics. This could be explained by the different socio-demographic backgrounds of the study sites.
With regard to practical attitudes, 74.55% (82/110) of the participants had a negative level of ergonomic practice. These results can be explained by the lack of knowledge in ergonomics, but also by the lack of adequate equipment. According to a study by Nissen A et al [7], the best practices in terms of physical working conditions to be recommended to nurses include the use of electric beds with variable heights, electric patient lifts and shower trolleys with electric height adjustment.
For the frequency of MSD occurrence, 57.27% (63/110) of nurses had MSDs, ergonomic practices were significantly associated with MSD occurrence [OR=3.07; CI: 1.13% - 10.04%; p-value=0.028]. This could be explained by the fact that nurses did not adopt adequate ergonomic postures when administering care. Indeed, a study by Evanoff B et al [8] showed that in the United States and in most industrialized countries, the rate of low back pain among nurses is very high, with patient handling being the main risk factor. Indeed, lifting and transferring patients must be done several times a day, and this handling is tiring: the patients are heavy, many of them weighing more than 100 kg.
Conclusion
Our study on the knowledge and practical attitudes in ergonomics among nurses at the Bafoussam Regional Hospital led us to conclude that the level of knowledge in ergonomics of these nurses was poor, their level of practice was harmful and the frequency of occurrence of MSDs was high. In view of the impact on occupational health, it is important to extend this study to the whole of Cameroon, in order to find ways of minimising the risks of work-related diseases.
Conflict of Interest: None
Acknowledgements: We thank all the staff who agreed to participate in this study.
References
- Murengezi J. (2009). Analysis of the working conditions of medical staff in rural areas. Online thesis; Université Libre de Kigali-Licence.
Publisher | Google Scholor - Falzon P. (2004). Nature, objectives and knowledge of ergonomics. Ergonomie. 15-35.
Publisher | Google Scholor - Charrier M, Bazzaro F, Sagot J. (2018). Taking better account of people with disabilities: supporting interdisciplinarity in design and ergonomics. Sciences du Design, 2(8):91-102.
Publisher | Google Scholor - Evanoff B, Wolf F, Canos J et al. (2003). Reduction in injuryrate in nursing personnel though introduction of mechanical lifts in the workplace. Am J Ind Med, 445(5):451-457.
Publisher | Google Scholor - Essi M, Njoya O. (2013). The CAP survey (Knowledge, Attitudes Practices) in medical research. Laboratoire de Recherche sur les Hépatites Virales et Communication en Santé-FMSB ; Health Sci. Dis, 14(2):1-2.
Publisher | Google Scholor - Rakhshaan K, Ambreen S, Rehana R, Umar A. (2012). knowledge and practices of ergonomics in computer users. JPMA-Journal of the Pakistan Medical Association, 62(3):23.
Publisher | Google Scholor - Nissen A, Gérimont C, Bidee J, Hansez I, Pepermans R. (2010). Good practice in physical and psychological working conditions for nurses. Results of the study
Publisher | Google Scholor - EvanoffB, Wolf L, Canos J et AL. (2003). Reduction in injury rates in nursing personnel through introduction of mechanical lifts in the workplace. Am J IndMed, 44(5):451.
Publisher | Google Scholor












