

Research Article
Knowledge, Attitude and Practice Regarding the Factors and Management of Maternal Mortality Amongst Degree and Diploma Nursing Students at A University
1University of Namibia, Windhoek, Namibia.
2School of Nursing and Public Health, Faculty of Health Sciences and Veterinary Medicine, University of Namibia.
*Corresponding Author: Joseph Galukeni Kadhila, School of Nursing and Public Health, Faculty of Health Sciences and Veterinary Medicine, University of Namibia.
Citation: Tjomombura E, Joseph G Kadhila. (2023). Knowledge, Attitude and Practice Regarding the Factors and Management of Maternal Mortality Amongst Degree and Diploma Nursing Students at A University. Addiction Research and Behavioural Therapies, BRS Publishers. 2(1); DOI: 10.59657/2837-8032.brs.23.004
Copyright: © 2023 Joseph Galukeni Kadhila, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 08, 2022 | Accepted: January 20, 2023 | Published: January 24, 2023
Abstract
Background: Maternal death is a major health problem in Namibia as it is the case in most countries. The rate at which women are dying due to pregnancy related causes is high and the cause as well as risk factors are not well explored. Despite the introduction of several interventions by the Ministry of Health and Social Services to prevent the maternal deaths, according to the Namibian Demographic Health Survey (NDHS) (2013) the maternal mortality ratio was 249 in 1992, 271 in 2000, 449 in 2006-2007 and 385 in 2013 respectively. It was against this background that the researcher conducted this to determine the knowledge, attitude and practice regarding the factors and management of maternal mortality amongst the 2nd year degree and diploma nursing students at a university, Windhoek, Namibia.
Aim: Assess the knowledge, attitude and practice of 2nd year degree nursing students and diploma nursing students at university regarding the factors and management of maternal mortality.
Objective: This project is a report of a study to determine the knowledge and practice of 2nd year diploma and degree nursing students regarding factors and their management and to evaluate the attitude and assess the practice of the 2nd year diploma and degree nursing at a university regarding factors and management of maternal mortality.
Methodology: In this study Quantitative approach was used so as to collect numerical data from the participants descriptive cross-sectional design was used to obtain data. Quantitative approach is the mathematical method of measuring and describing the observation of materials or characteristics. The target population of this study was the 2nd year diploma and degree student at the University of Namibia, main campus, Windhoek. Data was collected from the 13th of August 2022 to the 12th of October 2022 and was collected online using google forms. Researcher used probability sampling approach as a process of selecting the sample from the population. Descriptive statistics was used to determine the relationships between independent and dependent variables.
Results: A response rate of 54% was achieved. Out of 79 participants, 87.3% (n=69) were female and they were dominating while 12.7% (n=12) were male nursing students. All participants were Namibian. The majority of the participants had grade 12 certificate as the highest qualifications abstained. The study reveals that there was good display of knowledge, practice and attitude on the identification of factors related to maternal mortality.
Conclusion: lack of knowledge, practice and attitude on identification and proper management of factors associated with maternal mortality were revealed in the study. 34.6% of the participants failed to identify puerperal sepsis as an infection that can lead to maternal mortality while 65.4% were able to identify it correctly.
Keywords: maternal mortality; nursing students; factors; knowledge; practice and attitude
Introduction
The World Health Organisation defined maternal death as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes (Kornelius, 2018). The maternal death reviewed by the United Nations high Commissioner for Refugees (2020) estimated that half a million women die every year during pregnancy and childbirth, and an addition of above seven (7) million who survive childbirth suffer serious health problems. Maternal mortality deaths review provides an opportunity for health staff, family and community to learn from the tragic and prevent it from reoccurring. According to the WHO (2014) an estimated 800 women die from pregnancy or childbirth related complications around the world every day. In 2010, 28700 women died during and following pregnancy and childbirth (WHO, 2014). Furthermore, WHO (2014) stated that almost all of the deaths occurred in low resource settings. Maternal deaths due to pregnancy and child birth related complications were reported to be the major cause of death for women in the reproductive age group of 15-49 years (WHO, 2014). A study was conducted in Namibia by Mulama (2015) divulged that the direct causes of maternal mortality were haemorrhage (37.8%), eclampsia (24.4%) and puerperal sepsis (23.3%) and most of the woman affected by these conditions lived in rural areas. This complication can be avoided through proper teaching or demonstration and training of the students to be well equipped to prevent women from passing on after delivery. All women need is to have access to antenatal care in pregnancy, skilled care during childbirth and care and support in the weeks after childbirth (Mulama, 2015). In this study the researcher focused on the knowledge, attitude and practice of factors and management of the 2nd year degree and diploma university Nursing students at Windhoek.
Background
United Nations Children’s Fund (2019) stated that maternal mortality refers to deaths due to complications from pregnancy and childbirth. From 2000 to 2017, the global material Mortality ratio declined by 38 percent- from 342to 211 deaths per 10000 lives birth (UNHCR, 2019). Between 2000 and 2017, South Asia achieved the greatest overall percentage reduction in MMR (maternal mortality ratio), with a reduction of 59 percent from 395 to 163 maternal deaths per 100,000 live births (UNICEF, 2021). In India haemorrhage, sepsis and pregnancy induced hypertension including eclampsia were found to be the direct major cause of maternal mortality (Chanam Khumanthem, & Samjetshabam, 2012). Anaemia and cardiac disease were other indirect causes (Chanam at el, 2012). According to Chanam at el, 2012 state that all maternal deaths that were caused by direct causes could have been prevented if all abortions and deliveries were conducted by qualified medical personnel (Chanam at el, 2012). According to the Namibian demographic health survey [NDHS] (2013) The maternal mortality ratio was 249 in 1992, 271 in 2000, 449 in 2006-2007 and 385 in 2013 respectively (NDHS, 2013). However, Namibia is committed to reduce maternal mortality (WHO, 2009). This is evident in the multisectoral institutional structures the country has put in place, along with training of personnel in emergency obstetric and routine maternal death reviews, an enhanced referral system, construction of new health facilities and maternity waiting homes (and renovations of existing facilities), procurement of medical equipment and essential medicines, strengthening of adolescents’ sexual and reproductive health and rights, and improved efforts to prevent mother-to-child transmission of HIV. Other health interventions undertaken to improve maternal health include enhanced antenatal, delivery, and postnatal care services; preventive treatment of malaria during pregnancy; and tetanus toxoid immunization. Despite the interventions mentioned Countries in the eastern and southern region, Namibia included, still have relatively poor maternal outcomes.
Aim
Assess the knowledge, attitude and practice of 2nd year degree nursing students and diploma nursing students at a University, Windhoek Namibia regarding the factors and management of maternal mortality.
Method
A research design is a step-by-step approach used by a researcher to conduct a scientific study (Bhasin, 2019). In this study Quantitative, descriptive cross-sectional design was used to obtain data. Descriptive statistics was used to determine the relationships between independent and dependent variables (Delportet al, 2015). Quantitative approach was used so as to collect numerical data from the participants. Quantitative approach is the mathematical method of measuring and describing the observation of materials or characteristics.
Survey
According to Simplilearn (2022) data collection is the process of gathering, measuring, and analysing accurate data from a variety of relevant sources to find answers to research problems, answer questions, evaluate outcomes, and forecast trends and probabilities. The data was collected online using google forms that consist of four (A-D) sections. The researcher started by introducing herself (name, surname, field of study and the year of study). Thereafter the research provided and option for the participants to give consent by asking them to choose to take part in the study. The researcher further explained the objectives of the topic under study (To determine the knowledge of 2nd year degree and diploma nursing students at a University regarding the factors of maternal mortality, to determine the knowledge of 2nd year degree and diploma nursing students at a University regarding the management of maternal mortality and to evaluate attitudes and asses the practice of UNAM 2nd year degree and diploma nursing students regarding the factors and management of maternal mortality).
Ethical approval
Ethical clearance was obtained through the structures of the University of Namibia. Therefore, the following ethical considerations were written, informed consent was obtained from each participant after the procedure was explained and risks were pointed out after adequate information were conveyed, possible risks were pointed out. Voluntary participation without penalty for withdrawal was pointed out.
Data collection
In this study the researcher used a questionnaire on google form to collect the data from the participants. The questionnaire consisted of structured closed ended questions. The questionnaires were divided into 4 sections. Section A was demographic data, Section B consisted of questions on the knowledge of the 2nd year degree diploma nursing students regarding the factors of maternal mortality which were linear scale (agree, neutral and disagree) and close-ended (multiple choice) questions. Section C consisted of questions on management of maternal mortality which were asked in a form of multiple choice and linear scale (strongly agree, agree, neutral, disagree and strongly disagree). Section D included questions on how to evaluate the attitude and to assess the practice of 2nd year degree and diploma nursing students regarding management of maternal mortality and they were all linear scale (agree, neutral and disagree) questions.
Data analysis
Participant’s gender
Participants were asked to indicate their gender in the questionnaire as part of the demographic data obtained.
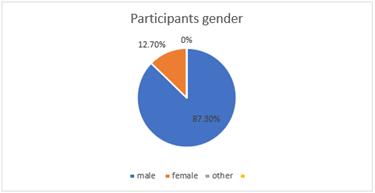
Figure 1: Participant’s gender.
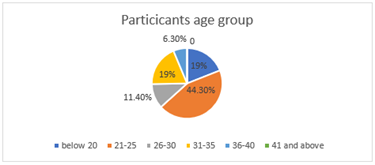
Figure 2:Participants age group.
The age group were ranging from below 20 to 41 and above. The results are shown in the pie chart above. 19% (n=15) were below 20 years, 44.3% (n=35) were 20-25 years of age and they were the dominating group, 11.4% (n=9) were 26-30 years, 19% (n=15) were 31-35 years old, 6.3% (n=5) were 36-40, which brought a total of 100% (n=79).
Participants Nationality
The participants were asked to indicate their nationality in the questionnaire and the options were provided, Namibia, SADC and others. 100% (n=79) of the participants were Namibian. The results are shown in the pie chart below.
Figure 3:Participants Nationality.
Participants highest qualifications obtained
Participants were asked to indicate their highest qualification obtained in the questionnaire as part of the demographic data obtained. 68.4% (n=54) had grade 12 certificate as their highest qualification while 31.6% (n=25) had a certificate in nursing (enrolled nurse).
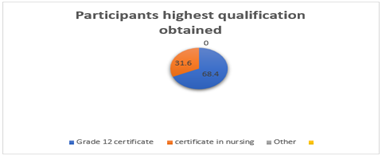
Figure 4:Participants highest qualifications obtained.
Section B: knowledge regarding the factors contributing to maternal mortality on 2nd year diploma and degree student at the University of Namibia main campus, Windhoek.
Variable 1: Data on what is maternal mortality. There were 78 participants. 7.7% (n=6) answered that maternal mortality is the death of a baby after delivery. 11.5% (n=9) answered that is the death of the mother after 45 days of termination of pregnancy. Finally, 80.8% (n=63) answered that maternal mortality is the death of a woman while pregnant of or 42 days after termination of pregnancy.
Table 1: What is maternal mortality?
| What is maternal mortality | Participant | Percentage |
| Death of a woman while pregnant of or 42 days after termination of pregnancy | n=63 | 80.8% |
| Death of the mother after 45 days of termination of pregnancy | n=9 | 11.5% |
| Death of a baby after delivery | n=6 | 7.7% |
Variable 2: The second variable, which of the following is the direct cause of maternal mortality. Participants had to choose between eclampsia, HIV and pneumonia. 78 participants answered this question. 93.6% (n=73) chose eclampsia and 5.4% (n=5) chose pneumonia.
Table 2: Which of the following is the direct cause of maternal mortality
| Which of the following is the direct cause of maternal mortality | Participants | Percentage |
| Eclampsia | n=73 | 93.6% |
| HIV | 0 | 0 |
| Pneumonia | n=5 | 5.4% |
Variable 3: The third variable, which one of the following is an infection that can lead to maternal mortality. Participants had to choose between haemorrhage, puerperal sepsis and anaemia. There were 78 participants. 34.6% (n=27) chose haemorrhage and 65.4% (n=51) chose puerperal sepsis.
Table 3: Which one of the following is an infection that can lead to maternal mortality.
| Which one of the following is an infection that can lead to maternal mortality | Participants | Percentage |
| Puerperal sepsis | n=51 | 65.4% |
| Haemorrhage | n=27 | 34.6% |
| Anaemia | 0 | 0 |
Variable 4: The fourth variable, 4. Which one is a risk factors of maternal mortality? 79 participants answered this question. 6.3% (n=5) chose age between 20-25 years, 92.4% (n=73) chose above 40 years and 1.3% (n=1) chose pregnant woman who goes to her ANC visit regularly.
Table 4: Which one is a risk factors of maternal mortality?
| Which one is a risk factors of maternal mortality | Participants | Percentage |
| Age between 20-25 | n=5 | 6.3% |
| Above 40 years | n=73 | 92.4% |
| Pregnant woman who goes to her ANC visit regularly | n=1 | 1.3% |
Variable 5: The fifth variable, Identify the woman by age, marital status and other chronic conditions that can lead to maternal mortality. There were 78 participants. Out of the total population 73.1% (n=57) agreed, 20.5% (n=16) were neutral and 6.4% (n=5) disagreed.
Table 5: Identify the woman by age, marital status and other chronic conditions that can lead to maternal mortality.
| How do you identify factors related to maternal mortality? | Agree | Neutral | Disagree | Total percentage |
| Identify the woman by age, marital status and other chronic conditions that can lead to maternal mortality. | 73.1% (n=57) | 20.5% (n=16) | 6.4% (n=5) | 100% (n=78) |
Variable 6: The sixth variable, monitor the foetus conditions only. 78 participants answered and out of the total population 11.4% (n=9) agreed, 11.4% (n=9) were neutral and 77.2% (n=61) disagreed.
Table 6: Monitor the foetus condition only.
| How do you identify factors related to maternal mortality? | Agree | Neutral | Disagree | Total percentage |
| Monitor the foetus conditions only. | 11.4% (n=9) | 11.4% (n=9) | 77.2% (n=61) | 100% (n=78) |
Variable 7: The seventh variable, Monitor the mother and the foetus at every ANC visit. Total of 79 students answered this question. Out of the total population 94.4% (n=74) agreed, 3.8% (n=3) were neutral and 1.3% (n=1) disagreed which made a total of 100% (n=79).
Table 7: Monitor the mother and foetus at every ANC visit.
| How do you identify factors related to maternal mortality? | Agree | Neutral | Disagree | Total percentage |
| Monitor the mother and the foetus at every ANC visit. | 94.9% (n=52) | 3.8% (n=3) | 1.3 (n=1) | 100% (n=79) |
Variable 8: The eighth variable, advice all pregnant woman to only come for ANC visit when they are nine (9) months pregnant. Out of the total that answered 3.8% (n=3) agreed and 7.6% (n=6) were neutral and 88.6% (n=70) disagreed which brought the total to 100% (n=79).
Table 8: Advice all pregnant woman to only come for ANC visit when they are nine (9) months pregnant.
| How do you identify factors related to maternal mortality? | Agree | Neutral | Disagree | Total percentage |
| Advise all pregnant woman to only come for ANC visit when they are nine (9) months pregnant. | 3.8% (n=3) | 7.6% (n=6) | 88.6% (n=70) | 100% (n=79) |
Section C:knowledge of the 2nd year diploma and degree nursing students on management of factors causing maternal mortality.
Variable 1: Data regarding practice of the 2nd year diploma and degree nursing students on management of factors causing maternal mortality. A total of 78 participants answered this question. 76.9% (n=60) strongly agreed, 20.5% (n=16) agreed, 1.3% (n=1) were neutral and 1.3% (n=1) disagreed.
Table 9: When a woman is haemorrhaging after delivery, you should by all means stop the bleeding as it can lead to maternal death.
| Management of factors causing maternal mortality. | 1=Strongly agree | 2=Agree | 3=Neutral | 4=Disagree | 5=Strongly disagree | Total percentage |
| When a woman is haemorrhaging after delivery, you should by all means stop the bleeding as it can lead to maternal death | 76.9% (n=60) | 20.5% (n=16) | 1.3% (n=1) | 1.3% (n-1) | 0 | 100% (n=78) |
Variable 2: The second variable, advice all pregnant women to go to any health facility when experiencing any danger signs at any time of the day. Out of the total 88.6% (n=70) strongly agreed, 8.9% (n=7) agreed, 1.3% (n=1) were neutral and 1.3% (n=1) disagreed, and in total 100% (n=79).
Table 10: Advice all pregnant women to go to any health facility when experiencing any danger signs at any time of the day.
| Management of factors causing maternal mortality. | 1=Strongly agree | 2=Agree | 3=Neutral | 4=Disagree | 5=Strongly disagree | Total percentage |
| Advice all pregnant women to go to any health. facility when experiencing any danger signs at any time of the day | 88.6% (n=70) | 8.9% (n=7) | 1.3% (n=1) | 1.3% (n=1) | 0 | 100% (n=79) |
Variable 3: The third variable, woman with hypertension is not considered as high risk in pregnancy. 79 students answered. Out of 79 participants 8.9% (n=7) strongly agreed, 3.8% (n=3) were neutral 13.9% (n=11) disagreed and 73.4% (n=58) strongly disagreed.
Table 11: Woman with hypertension is not considered as high risk in pregnancy.
| Management of factors causing maternal mortality. | 1=Strongly agree | 2=Agree | 3=Neutral | 4=Disagree | 5=Strongly disagree | Total percentage |
| Woman with hypertension is not considered as high risk in pregnancy | 8.9% (n=7) | 0 | 3.8% (n=3) | 13.9% (n=11) | 73.4% (n=58) | 100% (n=79) |
Variable 4: The fourth variable, during an ANC visit you must observe, measure and test any abnormalities of the woman and baby and intervene accordingly. 78 students answered this question, 64.1 (n=58) strongly agreed, 33.3% (n=26) agreed, 1.3% (n=1) were neural and 1.3% (n=1) strongly agreed.
Table 12: During an ANC visit you must observe, measure and test any abnormalities of the woman and baby and intervene accordingly.
| Management of factors causing maternal mortality. | 1=Strongly agree | 2=Agree | 3=Neutral | 4=Disagree | 5=Strongly disagree | Total percentage |
| During an ANC visit you must observe, measure and test any abnormalities of the woman and baby and intervene accordingly | 64.1% (n=58) | 33.3% (n=26) | 1.3% (n=1) | 0 | 1.3% (n=1) | 100% (n=78) |
Variable 5: The fifth variable, how would you prevent puerperal sepsis? A total of 79 participants answered. Out the total 77.2% (n=61) chose avoid frequent vaginal examination, 8.9% (n=7) chose to advice the woman to take in fatty diets and 13.9% (n=11) chose to administer oxytocin. Which brought a total of 100% (n=79) participants.
Table 13: How would you prevent puerperal sepsis?
| How would you prevent puerperal sepsis? | Participants | Percentage |
| Avoid frequent vaginal examination | (n=61) | 77.2% |
| Advice the woman to take in fatty diets | (n=7) | 8.9% |
| Administer oxytocin | (n=11) | 13.9% |
Variable 6: The sixth variable, what is the best management of postpartum haemorrhage after the bleeding has stopped? A total of 78 participants answered this question and 97.4% (n=76) chose to monitor the patient’s vitals until they are stable, 1.3% (n=1) chose to discharge patient and 1.3% (n=1) chose to monitor the wellbeing of the baby only. As illustrated in the pie chart above.
Table 14: What is the best management of postpartum haemorrhage after the bleeding has stopped?
| What is the best management of postpartum haemorrhage after the bleeding has stopped? | Participants | percentage |
| Monitor the patient’s vitals until they are stable | (n=76) | 97.4% |
| Discharge patient | (n=1) | 1.3% |
| Monitor the wellbeing of the baby only | (n=1) | 2.3% |
Section D: Attitude and practice of 2nd year diploma and degree nursing student on factors and management of maternal mortality.
Variable 1: Data on, a student nurse has a role in preventing maternal mortality. 79 participants answered the question. 74.7% (n=59) agreed, 24.1% (n=19) were neutral and 1.3% (n=) disagreed, making a total percentage of 100% (n=79).
Table 15: A student nurse has a role in preventing maternal mortality.
| Attitude and practice of 2nd year diploma and degree nursing student on factors and management of maternal mortality | Agree | Neutral | Disagree | Total percentage |
| A student nurse has a role in preventing maternal mortality | 74.7% (n=59) | 24.1% (n=19) | 1.3% (n=1) | 100% (n=79) |
Variable 2: The second variable was on all factors that lead to maternal mortality are regarded as obstetric emergencies. Out of the total population of 78 participants, 67% (n=53) agreed 25.6% (n=20) were neutral and 6.4% (n=5) disagreed.
Table 16: All factors that lead to maternal mortality are regarded as obstetric emergencies.
| Attitude and practice of 2nd year diploma and degree nursing student on factors and management of maternal mortality | Agree | Neutral | Disagree | Total percentage |
| All factors that lead to maternal mortality are regarded as obstetric emergencies | 67% (n=53) | 25.6% (n=20) | 6.4% (n=5) | 99.9% (n=78) |
Variable 3: The third variable was on; maternal mortality only occurs in people with colour. 79 students answered this question, 5.1% (n=4) were neutral and 94.9% (n=75) disagreed.
Table 17: Maternal mortality only occurs in people with colour.
| Attitude and practice of 2nd year diploma and degree nursing student on factors and management of maternal mortality | Agree | Neutral | Disagree | Total percentage |
| Maternal mortality only occurs in people with colour | 0 | 5.1% (n=4) | 94.9% (n=75) | 100% (n=79) |
Variable 4: The fourth variable, do you yell at women in labour to improve her pushing effort to prevent complications including maternal deaths. A total of 79 students answered this question. Out of the total population 19% (n=15) agreed, 25.3% (n=20) were neutral and 55.7% (n=44) disagreed.
Table 18: Do you yell at women in labour to improve her pushing effort to prevent complications including maternal deaths.
| Attitude and practice of 2nd year diploma and degree nursing student on factors and management of maternal mortality | Agree | Neutral | Disagree | Total percentage |
| Do you yell at women in labour to improve her pushing effort to prevent complications including maternal deaths | 19% (n=15) | 25.3% (n=20) | 55.7% (n=44) | 100% (n=79) |
Variable 5: The fifth variable, do you do vulva swabbing on patients who are in active labour and postnatal to prevent puerperal sepsis. 79 participants answered this question. Out of the total, 79.7% (n=63) agreed, 15.2% (n=12) were neutral and 5.1% (n=4) disagreed.
Table 19: Do you do vulva swabbing on patients who are in active labour and postnatal to prevent puerperal sepsis.
| Attitude and practice of 2nd year diploma and degree nursing student on factors and management of maternal mortality | Agree | Neutral | Disagree | Total percentage |
| Do you do vulva swabbing on patients who are in active labour and postnatal to prevent puerperal sepsis | 79.7% (n=63) | 15.2% (n=12) | 5.1% (n=4) | 100% (n=79) |
Results & Discussion
The researcher collected data using questionnaire (quantitative method). This questionnaire was distributed to 146 participants of the selected simple size, where by 79 (54%) students completed the questionnaire. 69 (46%) students did not complete the questionnaire that was shared using a link due to lack of internet access. Out of the total participants 54 (68.4)) were 2nd year degree nursing students while 25 (31.6%) of the participants were 2nd year diploma nursing students.
Section A: Demographic Data
Gender
As interpreted in chapter 4, majority of the participants were female nursing students with 83.3% (n=69) of the total population and 12.7% (n=12) were male nursing students. Nursing have been portrayed as a feminine occupation ever since the appearance of Nightingale nursing training style in the mid nineteenth century which favoured women over men to become nurses (Barrett-Landau & Henle, 2014). According to Barrett-Landau and Henle (2014) men continue to be a minority in the nursing profession. This could be the reason why female students are dominating in this study.
Age group
As shown in chapter 4 the age group were ranging from below 20 to 41 and above. The results are shown in the pie chart above. There were 19% (n=15) students who were below 20 years, 44.3% (n=35) of them were 20-25 years of age and they were the dominating group, 11.4% (n=9) were 26-30 years, 19% (n=15) were ranging from 31-35 years old, 6.3% (n=5) were 36-40 years old and finally no one was above the age of 41. The reason why the age range “between” 20-25 is dominating is because most of the participant just recently graduated high school (54 participants have a grade 12 certificate as their highest qualification) and could be the reason why this age group is dominating. Diploma students have a certificate and worked as enrolled nurses and their age is “between” 26-40.
Nationality
As illustrated in chapter 4, all the participants were Namibian 100% (n=79). This study was conducted in Namibia only, this could be the reason why all participants are Namibian and they were willing to learn and explore new knowledge, practice and attitude on factors related to maternal mortality.
Highest qualifications obtained.
As presented in chapter 4, 68.4% (n=54) had grade 12 certificate as their highest qualification while 31.6% (n=25) had a certificate in nursing (enrolled nurse). Meaning there are a lot of participants, who have obtained secondary qualification compared to all the qualifications. The participant age group can also help indicate that most of them are new high school leaver, that’s why most of them have secondary qualification. Which indicate that most of the students who took part are degree nursing students.
Section B: Knowledge Regarding the Factors Contributing to Maternal Mortality On 2nd Year Diploma and Degree Student at The University of Namibia Main Campus, Windhoek.
What is maternal mortality?
The study results illustrated that out of the 78 the participants, 80.8% (n=63) know the definition for maternal mortality. 11.5% (n=9) answered, death of mother after 45 days of termination of pregnancy and 7.7% (n=6) chose the death of a baby after deliver. The World Health Organisation defined maternal death as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes (Kornelius, 2018).
Which of the following is the direct cause of maternal mortality?
The study reveals 93.6% (n=73) chose eclampsia as a direct cause of maternal mortality, which indicates good knowledge participants possessed that eclampsia is a direct cause of maternal mortality. This can be supported by a study that was conducted in Namibia by Mulama (2015) divulged that the direct causes of maternal mortality were haemorrhage (37.8%), eclampsia (24.4%) and puerperal sepsis (23.3%). The 6.4% (n=5) chose pneumonia which is incorrect. According to Laibl (2015) pregnant women do not get pneumonia more than non-pregnant women.
Which one of the following is an infection that can lead to maternal mortality?
The study reveals that out of 78 participants 65.4% (n=51) chose puerperal sepsis as an infection that can cause maternal mortality, which illustrated good knowledge that puerperal sepsis is an infection that can lead to maternal mortality, and 34.6% (n=27) chose haemorrhage.
Which one of the following is a risk factor of maternal mortality?
The study reveals that this question was well answered and participants showed knowledge, as 92.4% (n=73) chose the risk of maternal mortality above 40 years. 6.4% (n=5) chose age between 20-35 and 1.3% (n=1) chose, pregnant woman who goes to her ANC visit regularly as a risk for maternal mortality. A United States showed that the factors that were associated with an increase in maternal mortality in the United States were, women over the age of 40 (Davis, Moniz & Nelson, 2018).
Identify the woman by age, marital status and other chronic conditions that can lead to maternal mortality
The study reveals that out of the total population of 78 participants, 73.1% (n=57) agreed to identify the woman by age, marital status and other chronic conditions that can lead to maternal mortality while 20.5% (n=16) were neutral and 6.4% (n=5) disagreed on this statement. This question was answered as a study conducted in the United States showed that the factors that were associated with an increase in maternal mortality in the United States were, women over the age of 40, women with diabetes and pregnancy related hypertension, African American women, and women with poor antenatal visits, smoking (Davis, Moniz & Nelson, 2018).
Monitor the foetus conditions only.
On this statement 78 participants answered and out of the total population 11.4% (n=9) agreed, 11.4% (n=9) were neutral and 77.2% (n=61) disagreed. This revealed good knowledge of participants 77.2% disagreed to the statement. According to Diana (2020) maternal mortality could be prevented though early detection to identify high risk factors such as woman’s age, medical condition and condition of the foetus at every ANC visit.
Monitor the mother and the foetus at every ANC visit.
Out of the total 79 participants, 94.4% (n=74) agreed that mother and foetus must be monitored at every ANC visit, 3.8% (n=3) were neutral and 1.3% (n=1) totally disagreed.
Advice all pregnant woman to only come for ANC visit when they are nine (9) months pregnant.
The study reveals that 88.6% (n=70) disagreed to this statement, while 3.8% (n=3) agreed and 7.6% (n=6) were neutral. It is an indication that participants have understanding on when pregnant woman should start ANC visits.
Section C: Knowledge of the 2nd Year Diploma and Degree Nursing Students on Management of Factors Causing Maternal Mortality.
When a woman is haemorrhaging after delivery, you should by all means stop the bleeding as it can lead to maternal death.
Out of the total of 78 participants, 76.9% (n=60) strongly agreed and 20.5% (n=16) just agreed, this revealed that there was good knowledge on how to manage haemorrhage. While 1.3% (n=1) was neutral and 1.3% (n=1) disagreed to the above-mentioned statement.
Advice all pregnant women to go to any health facility when experiencing any danger signs at any time of the day.
This study reveals that out of the total of 78 participants, 88.6% (n=70) strongly agreed, 8.9% (n=7) just agreed while, 1.3% (n=1) were neutral and 1.3% (n=1) disagreed. Good practice on management of factors that can lead to maternal mortality was illustrated.
Woman with hypertension is not considered as high risk in pregnancy.
Out of the total of 79 participants, 73.4% (n=58) strongly disagreed and 13.9% (n=11) just disagreed, while 8.9% (n=7) strongly agreed and 3.8% (n=3) were neutral. This revealed good practice on identifying factors that lead to maternal mortality.
During an ANC visit you must observe, measure and test any abnormalities of the woman and baby and intervene accordingly.
This study illustrated that out of the total of 78 participants, 64.1 (n=58) strongly agreed, 33.3% (n=26) just agreed while, 1.3% (n=1) were neural and 1.3% (n=1) strongly agreed. Participants showed good nursing practice. A study done in Ethiopia defined antenatal care (ANC) as special care for pregnant women with the aim of preventing, detecting and treating health problems in both the foetus and mother. Early ANC attendance promotes early detection and treatment of complications which result in proper management during delivery and puerperium (Wolde, 2019). Health interventions undertaken to improve maternal health include enhanced antenatal, delivery, and postnatal care services; preventive treatment of malaria during pregnancy; and tetanus toxoid immunization have been put in place.
How would you best prevent puerperal sepsis?
This study reveals that the majority of the participants showed good nursing practice as, 77.2% (n=61) chose avoid frequent vaginal examination to avoid cross infections. Study done in Tanzania have reported that risk factors contributing to puerperal sepsis include prolonged labour, early rupture of membrane for more than 24 hours and repeated vaginal examination for more than five times during labour (Nchimbi, 2022).
What is the best management of postpartum haemorrhage after the bleeding has stopped?
A total of 78 participants answered this question. The study reveals that students had good practical understanding as, 97.4% (n=76) chose to monitor the patient’s vitals until they are stable, 1.3% (n=1) chose to discharge patient and 1.3% (n=1) chose to monitor the wellbeing of the baby only. According to WHO (2015) primary goals for postpartum haemorrhage is to identify and correct the source of the bleeding, restore blood volume and stabilize vital signs and level of consciousness.
Section D: Attitude and Practice Of 2nd Year Diploma and Degree Nursing Student on Factors and Management of Maternal Mortality
A student nurse has a role in preventing maternal mortality
Total participants were 79. This study showed that the participants have good understands as, 74.7% (n=59) agreed, 24.1% (n=19) were neutral and 1.3% (n=1) disagreed. Midwives and nurses have a specific duty to support women’s health and to advocate for the resources necessary to reduce maternal mortality, increase access to family planning, and elevate the pursuit of gender equity and women’s rights around the globe (Erin, 2022).
All factors that lead to maternal mortality are regarded as obstetric emergencies.
The study revealed that the participants had a fair understanding as, 67% (n=53) agreed 25.6% (n=20) were neutral and 6.4% (n=5) disagreed. A study contacted in Mozambique used Statistical models to assess the association between delay to reach the health facility that provides emergency obstetric care (delay type II) and delay in receiving appropriate care once reaching the health facility providing emergency obstetric care (delay type III) and the cause of maternal death within the health facility (Chavane, 2018) Treat all obstetrics emergencies as a risk potential to maternal and neonatal mortality (Chavane, 2018).
Maternal mortality only occurs in people with colour.
A total of 79 students answered this question, and participants showed excellent attitude and understanding as, 5.1% (n=4) were neutral and 94.9% (n=75) disagreed. A study conducted in the United States showed an increase in maternal mortality from 9.5 deaths per 100000 live births in 1997 to 19.9 deaths per 100000 in 2012 (Davis, Moniz & Nelson, 2018). The factors that were associated with an increase in maternal mortality in the United States were, women over the age of 40, women with diabetes and pregnancy related hypertension, African American women, and women with poor antenatal visits, smoking and obese women (Davis et al, 2018). Maternal death is still a cause for concern for most African countries. This is an indication that maternal mortality occurs in all women, black or coloured.
Do you yell at women in labour to improve her pushing effort to prevent complications including maternal deaths?
This study showed that students have good attitude towards patients as, 55.7% (n=44) disagree, 19% (n=15) agreed and 25.3% (n=20) were neutral. As survey done in Namibia reported that, (49.5%) agreed that “sometimes you have to yell at a woman in labour because she is not pushing hard enough,” and (30.1%) agreed that “pinching or slapping a woman in labour can succeed in getting her to push harder”. Furthermore, Carlough at el (2018) is of opinion that the registered and enrolled nurses are more likely at yelling to a woman in labour than medical officers. The perceived necessity of yelling at labouring women to encourage pushing was mentioned in every focus group discussion and most interviews (Carlough at el, 2018). Nurses in the focus groups also reported other disrespectful behaviours (such as hostile body language, intimidation, and “beating”), but often linked these to patient behaviours such as being “uncooperative” or unwilling to “open their legs (Carlough at el, 2018).
Do you do vulva swabbing on patients who are in active labour and postnatal to prevent puerperal sepsis?
The study illustrated good practice, as out of 79 participants, 79.7% (n=63) agreed, 15.2% (n=12) were neutral, and 5.1% (n=4) disagreed. The World Health Organization (2015) states that continual perineal swabs should be administered to women who are in active labour, have premature rupture of the membranes, or are receiving perinatal care in order to prevent infections such puerperal sepsis.
Conclusion
The main aim of this study was to assess the knowledge, attitude and practice of 2nd year diploma and 2nd year degree nursing students at the University of Namibia, main campus, Windhoek regarding factors and management of maternal mortality. The study revealed that the 2nd year degree and 2nd diploma students have good/adequate knowledge, attitude and practice regarding factors and management of maternal mortality. On this variable the participants showed perfect knowledge in identifying the direct cause of maternal mortality, 93.6% (n=73) chose eclampsia as a direct cause of maternal mortality. The rest of the participants 5.4% (n=5) chose pneumonia. Minority of the participants, showed a lack of knowledge regarding the identification of infection that can cause maternal mortality. 34.6% (n=27) identified haemorrhage as an infection that can lead to maternal mortality. 65.4% (n=51) identified puerperal sepsis as an infection that can lead to maternal mortality. Overall, the study findings show that the 2nd year degree and 2nd diploma students have adequate knowledge, attitude and practice regarding factors and management of maternal mortality.
Limitation
This study assessed the knowledge, attitude and practice of the 2nd year degree and 2nd diploma student regarding factors related to maternal mortality at UNAM, main campus Windhoek. The questionnaire could not be administered face-to-face to the targeted population due to financial constraints and as a result the questionnaire was administered online using a link and the participant’s outcome was a challenge. The questionnaire was very long and students were not willing to answer, that leads to some students answering some questions only.
Declarations
Acknowledgements
I would like to thank the second-year diploma and second year degree nursing students
Authors contributions
Eveline Tjomombura original draft preparation data analysis and writing up: Joseph Galukeni Kadhila was responsible for supervision and editing of manuscript.
Consent to publish
Not applicable
Funding
No funding was received for this study.
Availability of data materials
The data base is available on request from the corresponding author.
Ethics approval and consent
Ethical clearance was obtained from the School of Nursing and Public Health, University of Namibia Research Ethics Committee, all principles of ethical consideration were respected and adhered to. Prior to data collection all participants signed a written consent to participate in the study.
Competing interest
The authors declared no conflict of interest.
References
- Barrett-Landau, S, & Henle, S. (2014) Man in nursing: their influence in the female dominated career J Leadership Institution.
Publisher | Google Scholor - Berhan, A., &. Berhan, Y. (2014). Causes of Maternal Mortality in Ethiopia. A significant Decline in Abortion Related Deaths. Ethiopia:
Publisher | Google Scholor - Bell. S., Prata. N. & Quaiyum.A. (2014) Modeling maternal mortality in Bangladesh: the role of misoprostol in postpartum hemorrhage prevention.
Publisher | Google Scholor - Bhandari. P. (2021) Ethical considerations in Research, Types& Examples
Publisher | Google Scholor - Brink, H. Van Der Walt, C. Van Rensburg, G. (2012) Fundamentals of Research Methodology for Healthcare Professionals (3rd ed). Cape Town: Juta & Company (PTY) LTD.
Publisher | Google Scholor - Brink, S. (2017). Namibia Sees Reduction in Maternal Deaths: New Era. Retrieved October 2017 from Burns. N. A., & Grove. S.K,. (2013). Understanding Nursing Research.
Publisher | Google Scholor - Carlough, M., Hamunime, N., Katjiuanjo, P., Kalimugogo, P., McQuide, P., Viadro, C., & Wesson, J. (2018). Provider and client perspectives on maternity care in Namibia: results from two cross-sectional studies. BMC Pregnancy Childbirth 18, 363 (2018).
Publisher | Google Scholor - David .M, Moniz .M, & Nelson. D. (2018). Health Factors Linked to Maternal Morbidity and Mortality.
Publisher | Google Scholor - Diana, S. (2020). Maternal complication and risk factors for mortality. The United States national library of medicine.
Publisher | Google Scholor - Delport.C. S. L., De Vos, A. Fouche, C. B S., & Strydom, H. (2011). Research at Grass Roots. Pretoria: Van Schaik.
Publisher | Google Scholor - Bulto. G. A., Demisse. G.A, Fekene. D.B, kedir. B., & Sifer. S.D, (2018). Determinants of puerperal sepsis among post-partum women at public hospitals in west SHOA zone Oromia regional STATE, Ethiopia (institution BASEDCASE control study).
Publisher | Google Scholor - Girum. T., & Wasie. A.(2017). Correlates of maternal mortality in developing countries: an ecological study in 82 countries.
Publisher | Google Scholor - Haradhan, M. (2016). Knowledge is an essential element at present world. Retrieved 18 April 2016 from
Publisher | Google Scholor - Johnson. K., Rroydhouse. J. K., Scott. K., & White.K. (2011). Knowledge and skills of cancer clinical trials nurses in Australia.
Publisher | Google Scholor - Kornelius, L. (2018). Factors associated with maternal deaths at Intermediate Hospital Oshakati. Oshana region. Namibia. University of Namibia.
Publisher | Google Scholor - Kumar. (2015). Research Methodology, step by step guide for Beginners (3rd Ed) Los Angeles. Sage.
Publisher | Google Scholor - Kumar, P., & Singh, S (2012). Does Male Participation in Maternal Health can achieve MDGs in India. Evidence from National Family Health Survey. New Delhi
Publisher | Google Scholor - Mulama, L., N. (2015). Analysis of causes and risk factors associated with maternal deaths in Namibia. Windhoek. Namibia. University of Namibia.
Publisher | Google Scholor - Mudavanhu, Y. (2017). Quality of literature review and discussion of findings in selected papers on integration of ICT in teaching, role of mentors, and teaching science through science, technology, engineering, and mathematics (STEM). Educational Research and Reviews. 12. 189-201. 10.5897/ERR2016.3088.
Publisher | Google Scholor - Muzeya F. (2015). Knowledge, attitudes and practices of nurse-midwives related to obstetric care at Thaba-Tseka district in Lesotho.
Publisher | Google Scholor - Namibia Demographic Health Survey. (2013). The Namibian health survey. Ministry of health and social services. Windhoek. Namibia.
Publisher | Google Scholor - Nchimbi. D,.B. (2022). Puerperal sepsis-related knowledge and reported self-care.
Publisher | Google Scholor - Nkhwalume. L. & Mashalla. Y. (2019). Maternal mortality trends at the Princess Marina and Nyangabwe referral hospitals in Botswana.
Publisher | Google Scholor - Republic of Namibia. (2011). Report of the survey on the factors contributing to maternal mortality and the prevalence of missed maternal deaths. Windhoek: Ministry of Health and Social Services
Publisher | Google Scholor - Republic of Namibia. (2014). Report of the Prevalence and Contributing Factors of Facility –Based Maternal and Neonatal Deaths in Five Regions of Namibia. Windhoek: Ministry of Health and Social Services.
Publisher | Google Scholor - Republic of Namibia. (2016). Report on Joint Review of Maternal, New-born, Child & Adolescent Health and Nutrition Programmes in Namibia. Windhoek: Ministry of Health and Social Services.
Publisher | Google Scholor - Simplilearn. (2022). What Is Data Collection: Methods, Types, Tools, and Techniques.
Publisher | Google Scholor - United Nations Children’s Fund. (2019). Maternal mortality declined by 38 per cent between 2000 and 2017.
Publisher | Google Scholor - United Nations High Commissioner for Refugee. (2020). Maternal death review guidance and datacollection.
Publisher | Google Scholor - United Nations, (2012). Assessing progress in Africa toward the Millennium Development Goals. MDG Report 2012.
Publisher | Google Scholor - World Health Organisation, (2010). Trends in Maternal Mortality. Geneva: UNICEF.
Publisher | Google Scholor - World Health Organization. (2014). Maternal mortality.
Publisher | Google Scholor - World Health Organization. (2014). Trends in maternal mortality: 1990 to 2013 estimates developed by WHO, UNICEF, UNFPA and The World Bank, Geneva: WHO.
Publisher | Google Scholor - World Health Organisation media Centre, (2015). Global Strategy for Women’s, Children and Adolescents’ Health. 2016-2030. New York: United Nations
Publisher | Google Scholor - World Health Organisation. (2019). Maternal mortality.
Publisher | Google Scholor













