

Research Article
Is There a Relationship between Psychological Status and Posture in Chronic Low Back Pain?
- Mehrzia Amani Khezami 1,2,3
- Emna Bahlouli 1,2,3
- Imededdine Ben Jeddou 1, 3*
- Fatma Zohra Ben Salah 1,2,3
- Mouna Soltani 1,3
- Ines Aloulou 1,3
- Leïla Ghidaoui 1,2,3
- Imen Miri 1,2
- Sonia Lebib 1,2
- Catherine Dziri 1,2,3
1.Department of Physical and Rehabilitation Medicine, National Institute of Orthopedy Mohamed KASSAB, La Manouba, Tunisia.
2.Tunis El Manar University, Faculty of Medicine of Tunis, Tunisia.
3.Laboratory for Research and Innovation on Social maladjustment and Disability, Tunisia.
*Corresponding Author: Imededdine Ben Jeddou, Department of Physical and Rehabilitation Medicine, National Institute of Orthopedy Mohamed KASSAB, La Manouba, Tunisia.
Citation: Mehrzia A Khezami, E Bahlouli, Imededdine B Jeddou, F.Z.B Salah, Soltani M, et al. (2023). Is There a Relationship between Psychological Status and Posture in Chronic Low Back Pain? Journal of Clinical Psychology and Mental Health, BioRes Scientia Publishers, 2(1):1-6. DOI: 10.59657/2993-0227.brs.23.006
Copyright: © 2023 Imededdine Ben Jeddou, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 01, 2023 | Accepted: May 16, 2023 | Published: May 22, 2023
Abstract
Context: Chronic non-specific low back pain (CNLBP) is a major public health. Numerous studies have evaluated the contribution of post urology in the assessment and the rehabilitation of this pathology. Nevertheless, the relationship between post urology and muscle assessment is still a subject of controversy and no clear cause and effect relationship between the two could be established.
Aim: The aim of our work was to investigate the relationship between post urological and muscular assessments in patients with CNLBP.
Methods: It’s about an observational, descriptive, and cross-sectional study. The muscle assessment included Quadriceps Femoris flexibility using the heel-to-buttock distance and Hamstrings flexibility using the popliteal angle. Isometric muscle strength of the extensor and flexor muscles of the trunk was assessed by the Biering-Sorensen test and the Shirado test, respectively. The evaluation of static postural control was performed by the SATEL® force platform in two conditions (opened eyes/closed mouth) and (closed eyes/closed mouth). The selected parameters were S (mm2), XY (mm), X (mm), Y (mm), support (%), and Romberg Quotient (RQ). The chi-square test or Fisher's exact test was used to assess differences between categorical variables, and means were compared using Pearson's or Spearman's correlation tests depending on the distribution of the variables. Comparison between qualitative and quantitative variables was done by ANOVA test for normally distributed variables and Mann-Whitney or Kruskall-Wallis tests for non-normally distributed data.
Results: Forty patients were included. The study of muscle flexibility according to force platform parameters showed that left Hamstring stiffness was significantly correlated with XY (p=.037) and with instability in the sagittal plane (p=.036). On the other hand, the stiffness of the anterior rectus muscles (right and/or left) was significantly correlated with XY (p=0.019 for the right muscle and 0.011 for the left muscle) and with postural instability in the frontal plane (p=.015 for the right muscle and .026 for the left muscle). We also founded a significant association between the increase in Romberg quotient and right Hamstring stiffness (p=.003).
Conclusions: Our study as well as literature findings suggest that the Quadriceps Femoris and the Hamstrings play have a significant role in core stability of patients with chronic non-specific back pain. However, the origin of the population is also an important factor in the postural evaluation. A larger number of patients and a control group would have made it possible to establish a cause- effect relationship between Quadriceps Femoris, Hamstrings and static postural control abnormalities.
Keywords: chronic non-specific low back pain; posture; psychology
Introduction
Chronic low back pain (CLBP) is one of the most frequent musculoskeletal disorders. Its prevalence worldwide has been estimated in 2019 at 7.64%, i.e. approximately six hundred million people [1], of which 5% to 10% progress to chronicity [2]. These chronic forms are responsible for an alteration of life’s quality due to physical and psychological handicaps. In fact, according to the Global Burden of Disease study conducted from 1990 to 2019, chronic low back pain is among the top ten disabling diseases and is responsible for 7.41% of the total years lived with disability [3].This data underlines the importance of early and effective management of this condition. In fact, most international guidelines recommend a multidisciplinary therapeutical approach to CLBP. Therefore, psychological evaluation is one of the pillars of the evaluation and management of patients with CLBP.The interrelationship between posture and emotional processes is widely discussed in literature. However, few studies have examined the relationship between posture and psychological assessment in patients with low back pain.
Material and Methods
An observational, descriptive, and cross-sectional study conducted within the department of physical medicine and rehabilitation in KASSAB’s Institute over a period of 8 months. The patients included were those with CNLBP. We did not include patients with symptomatic spinal low back pain related to an infectious, inflammatory, tumoral or traumatic cause, those with a radicular syndrome, an advanced or relapsing go arthrosis or coxarthrosis, patients with a surgical intervention on the spine or the lower limbs in their history. The postural profile was classified according to Gagey’s classification which is a gold standard in clinical posture studies [4,5]. It distinguishes 5 clinical profiles ranging from A to E according to the sagittal profile study. Only the Gagey A profile corresponds to harmonious spinal curves (Figure 1).
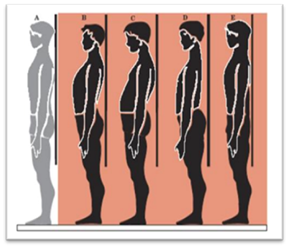
Figure 1: Classification of postural disorders according to Gagey et al.
We performed a psychological evaluation of our patients using two scales: the Hospital Anxiety and Depression Scale (HADS) and the Fear-Avoidance Beliefs Questionnaire (FABQ). The Hospital Anxiety and Depression Scale (HADS) is a generic self-administered questionnaire validated for low back pain [6]. A Tunisian dialect version of the HADS was used allowing us to calculate a sub-score for anxiety and another for depression. The Fear-Avoidance Beliefs Questionnaire (FABQ) is a self-administered questionnaire specific to low back pain. A validated Arabic version [7] was used. This scale consists of Physical Activity Subscale (FABQ-PA) and Work Subscale (FABQ-W). The overall FABQ score is calculated by adding the scores of the 15 questionnaire items. It is positively correlated with the level of fears and beliefs: the higher the score, the higher the level of fears and beliefs.
The collected data were checked for missing values and errors before being transferred to IBM SPSS Statistics version 26.0 for statistical analysis. For the descriptive study, normality was checked using the Kolmogorov-Smirnov or Shapiro-Wilk tests, depending on each test’s conditions. Absolute and relative frequencies (percentages) were calculated for qualitative variables. We calculated means, medians and standard deviations and determined extreme values for the quantitative variables. For the analytical study, Chi-square test or Fisher's exact test was used to assess differences between categorical variables, and means were compared using Pearson's or Spearman's correlation tests depending on the distribution of variables. Comparison between qualitative and quantitative variables was done by ANOVA test for normally distributed variables and Mann-Whitney or Kruskal-Wallis tests for non-normally distributed data.
In all statistical tests, the significance level was set at 0.05. Our research was carried out in accordance with the Helsinki Declaration and was approved by an appropriate ethics committee. The name of the Ethics Committee is: EHTICS COMMITTEE APPROVAL: B Department of physical and rehabilitation medicine, under Project References: IMKO-CE-2022-6.
Results
Our population included 40 patients who met our criteria with a median age of 32 years and a sex ratio of 0.43. According to the Gagey clinical classification, 34 patients (85%) had a pathological postural profile (Figure 2). The profile corresponding to a posterior scapular plane classified Gagey C was predominant (14 patients). Twenty-five patients presented Questionable or definite anxiety symptomatology while 17 others suffered from questionable or definite depressive symptomatology (Figure 3). The mean anxiety score was equal to 8.25 with extremes ranging from 2 to 19 and a standard deviation equal to 4.09 while the mean depression score was equal to 6.53 with extremes ranging from 0 to 16 and a standard deviation equal to 3.84. The FABQ-PA score was high in 21 patients, indicating a high level of fears and beliefs related to physical activity. On the other hand, the FABQ-W score indicating the level of fears and beliefs related to work was high in only 9 patients. The mean FABQ-W score was 43.80 ± 17.88, with minimum and maximum values of 15 and 84, respectively.
The mean of the FABQ-PA was equal to 15.47 ± 7.05 with extremes ranging from 3 to 38 and the mean of the FABQ-W was equal to 21.88 ± 11.53 with extremes ranging from 0 to 40. We did not objectify a significant association between the global score of fears and beliefs related to low back pain and the clinical classification of the postural profile according to Gagey (Table I). However, patients with a pathological clinical profile according to Gagey, i.e., profiles B, C, D, and E, had a significantly higher level of fears and beliefs related to physical activity (FABQ-PA) (P=.007). The multiple comparison study (Figure 4) showed that the level of fears and beliefs related to physical activity in patients classified as Gagey C and D was significantly higher than in the normal Gagey clinical profile with p equal to .008 and .004 respectively. After adjustment by Bonferroni correction, only Gagey Profile D presented a level of fears and beliefs related to physical activity significantly higher than that observed in Gagey Profile A with adjusted p equal to .042.
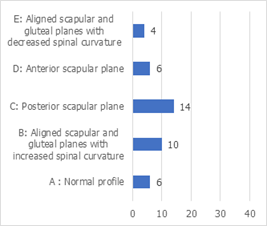
Figure 2: Distribution of postural profiles according to Gagey's classification.
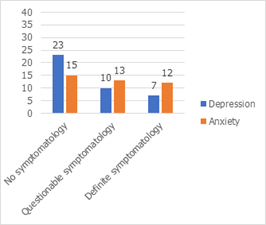
Figure 3: Distribution according to the Hospital Anxiety and Depression Scale.
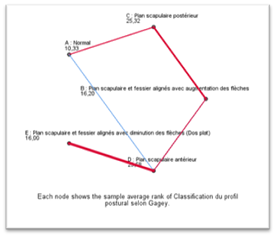
Figure 4: Multiple comparisons of the FABQ-PA scores according to Gagey’s classification.
Furthermore, we did not observe any significant associations between Gagey's clinical post urological profiles and anxiety and/or depressive symptomatology assessed by the HADS (p=.679 for the anxiety sub score and p=.317 for the depression sub score).
Discussion
The interrelationship between posture and emotional processes in CLBP is a widely debated point in the literature. In fact, according to the embodiment theory of emotions [8,9] the experience of emotional states affects the soma to visceral and motor systems (e.g., mood affects posture) which in turn influence the processing of emotional information. Several studies have asserted this bidirectional influence of the motor system and emotional processes. For example, studies on the effects of mood on the motor system have shown that experimentally induced mood states, such as sadness, happiness and pride, have effects on posture or gait [10,11]. In addition, some studies [12] have suggested a reverse-directed causal mechanism, in which the motor system had effects on emotional processes. According to RISKIND et al [13], while recalling pleasant or unpleasant life experiences, participants were instructed in one condition to have a smile on their face while upright or to have a downcast expression with head and neck bowed and body slumped in another condition. Access to pleasant or unpleasant life experiences improved when participants were positioned in postures and facial expressions congruent with the emotional valence of those life experiences, as opposed to incongruent postures and facial expressions.
These results suggest an entirely unexplored role for body postures in self-evaluation and demonstrate the importance of understanding metacognitive processes in embodiment. On the other hand, an important place is attributed to the psychological component in the genesis and maintenance of low back pain. Several studies [14,15] have shown the influence of psychological factors on the perception of pain evaluated by the Visual Analog Scale, in particular depression and anxiety, emphasizing the link that these factors have with pain, from its onset to its chronicization. Other authors suggest that pain increases the risk of depression. According to Yang et al [16], chronic pain leads to structural and functional changes in the cortico-limbic regions of the brain that may be responsible for negative affective states such as depression, anger and anxiety. In our study, 43% of patients showed depressive symptomatology and 63% showed anxiety symptomatology. However, we did not objectify significant associations between anxiety/depression and postural disorders. A larger population might have demonstrated this interrelationship.
Conclusion
Chronic low back pain is a frequent pathology with heavy consequences. An adequate and early management of this pathology could eventually limit the repercussions of this disabling disease. Our study has shown an important role of emotions in posture. A multidimensional social, psychological and biological approach in the management and evaluation of CCL based on validated scores could avoid the risk of transition to chronicity and improve the resulting disability.
List of abbreviations
CNLBP: Chronic non-specific low back pain;
RQ: Romberg Quotient;
HADS: Hospital Anxiety and Depression Scale;
FABQ: Fear-Avoidance Beliefs Questionnaire ;
FABQ-PA: Fear-Avoidance Beliefs Questionnaire of Physical Activity Subscale;
FABQ-W: Fear-Avoidance Beliefs Questionnaire Work Subscale;
CCL: Cognition, Comportements, Langage.
Declarations
I declare that all data are available.
Authors say they have no competing interests.
No funding has been allocated to this research.
References
- GBD Compare IHME Viz Hub.
Publisher | Google Scholor - Low back pain-EM consult.
Publisher | Google Scholor - GBD 2019 Diseases and Injuries Collaborators. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet, 396(10258):1204‑1222.
Publisher | Google Scholor - Gagey PM, Baron JB, Ushio N. (1980). Introduction to clinical posturology. Agressologie, 21(E):119‑123.
Publisher | Google Scholor - Posturology, Book.
Publisher | Google Scholor - Turk DC, Dworkin RH, Trudeau JJ, Benson C, Biondi DM, Katz NP, et al. (2015). Validation of the Hospital Anxiety and Depression Scale in Patients with Acute Low Back Pain. The Journal of Pain, 16(10):1012‑1021.
Publisher | Google Scholor - Alanazi F, Gleeson P, Olson S, Roddey T. (2017). Translation and Validation of the Arabic Version of the Fear-Avoidance Beliefs Questionnaire in Patients with Low Back Pain. Spine, 42(7):411‑416.
Publisher | Google Scholor - Niedenthal PM. (2007). Embodying Emotion. Science, 316(5827):1002‑1005.
Publisher | Google Scholor - Niedenthal PM, Barsalou LW, Winkielman P, Krauth-Gruber S, Ric F. (2005). Embodiment in Attitudes, Social Perception, and Emotion. Pers Soc Psychol Rev, 9(3):184‑211.
Publisher | Google Scholor - Oosterwijk S, Rotteveel M, Fischer AH, Hess U. (2009). Embodied emotion concepts: How generating words about pride and disappointment influences posture. European Journal of Social Psychology, 39(3):457‑466.
Publisher | Google Scholor - Michalak J, Mischnat J, Teismann T. (2014). Sitting Posture Makes a Difference—Embodiment Effects on Depressive Memory Bias. Clinical Psychology & Psychotherapy, 21(6):519-524.
Publisher | Google Scholor - Reed CL, Moody EJ, Mgrublian K, Assaad S, Schey A, McIntosh DN. (2020). Body Matters in Emotion: Restricted Body Movement and Posture Affect Expression and Recognition of Status-Related Emotions. Frontiers in Psychology. Available from: https://www.frontiersin.org/articles/10.3389/fpsyg.2020.01961
Publisher | Google Scholor - Riskind JH. (1983). Nonverbal expressions and the accessibility of life experience memories: A congruence hypothesis. Social Cognition, 2:62‑86.
Publisher | Google Scholor - Linton SJ. (2000). A Review of Psychological Risk Factors in Back and Neck Pain. Spine, 25(9):1148-1156.
Publisher | Google Scholor - Nassar N, Assaf N, Farrag D, Ibrahim D, Al-Sheekh A. (2019). Depression in patients with chronic low back pain. Egypt RheumatolRehabil. Janv, 46(1):48-54.
Publisher | Google Scholor - Yang S, Chang MC. (2019). Chronic Pain: Structural and Functional Changes in Brain Structures and Associated Negative Affective States. International Journal of Molecular Sciences. Janv, 20(13):3130.
Publisher | Google Scholor














