

Case Report
Heterotopic Sebaceous Glands in the Esophagus: A Case Report and Comprehensive Literature Review
1The Ohio State University College of Medicine Columbus, OH, United States.
2Division of Gastroenterology Wexner Medical Center Columbus, OH, United States.
3Division of Pathology Wexner Medical Center Columbus, OH, United States.
*Corresponding Author: Subhankar Chakraborty,The Ohio State University College of Medicine Columbus, OH, United States.
Citation: Matthew L. Yoder, Gallardo M, Chakraborty S, Yearsley M. (2023). Heterotopic Sebaceous Glands in the Esophagus: A Case Report and Comprehensive Literature Review, International Journal of Medical Case Reports and Reviews, BioRes Scientia Publishers. 2(5):1-5. DOI: 10.59657/2837-8172.brs.23.035
Copyright: © 2023 Subhankar Chakraborty, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: October 20, 2023 | Accepted: October 31, 2023 | Published: November 01, 2023
Abstract
Heterotopic sebaceous glands (HSG) are one of the rarest benign lesions discovered on endoscopy. Treatment is currently not recommended given the benign and asymptomatic presence of these lesions. We present a case of an elderly male patient who presented with symptoms of throat itching, cough, phlegm, and altered taste found to have esophageal dysmotility in the setting of multiple, diffuse HSGs in the esophagus. HSG was confirmed on histopathological examination. Functional esophageal studies revealed spastic motility of the esophageal body, poor clearance of liquids, and impaired distensibility of upper and lower esophageal sphincters. Our case illustrates that they may be responsible for symptoms and may be associated with impaired esophageal function. HSGs do not require surveillance endoscopy or treatment. They should be considered in the differential diagnosis of yellowish elevated lesions in the esophagus.
Keywords: ectopic sebaceous glands; heterotopic sebaceous glands; esophagus; endo flip; benign esophageal lesions
Introduction
Sebaceous glands are normally found in human hair follicles, most numerously on the face and scalp [1]. Sebaceous glands are found in the dermis layer of the skin attached to hair follicles and function to secrete sebum, an oily substance, which lubricates the hair [1]. Heterotopic sebaceous glands have been reported most typically around ectodermal organs such as the lips, oral cavity, parotid glands, tongue, larynx and external genitalia, consistent with their ectodermal origin.1 Patients often seek care related to their sebaceous glands from dermatologists given their role in acne vulgaris and other pathologies of the skin [2]. Their presence in the esophagus, which is endodermal in origin, is distinctly unusual [3]. When present, they are termed heterotopic indicating their ectopic location in the gastrointestinal tract. Only a few cases have been reported in the literature. We report a case of heterotopic sebaceous glands (HSGs) in the esophagus. We performed functional assessment of esophageal function and we discuss potential implication of HSGs in esophageal dysmotility. Finally, we also review the literature about HSGs in the esophagus.
Case
A 77-year-old male patient presented to the GI clinic for evaluation of a GI cause for his symptoms of cough, itchy throat, phlegm, and altered taste that had been ongoing for about 1 year. He denied dysphagia, globus sensation, and coughing or choking when eating. He had recently stopped taking a proton pump inhibitor because it was not providing adequate symptom relief. An esophagogastroduodenoscopy (EGD) 8 months earlier had normal findings. Esophageal manometry was attempted but only one swallow could be performed before it had to be removed due to poor tolerance. This brief study showed fragmented peristalsis (Figure 1A). A barium esophageal revealed poor clearance of liquid from the esophageal body (Figure 1B) but a 13 mm barium tablet passed normal. Past medical history was significant for coronary artery disease and gastrointestinal (GI) reflux disease based on symptoms. To investigate if functional abnormalities such as esophageal sphincter dysfunction or esophageal body dysmotility was playing a role in their symptom, we performed an EGD with Endo FLIP. Endo FLIP stands for endoscopic functional luminal impedance planimetry. It is a technique which allows assessment of sphincter tightness by measuring the cross-sectional area and pressure inside the FLIP balloon. This parameter is called the distensibility index (DI). A DI between 3-9 mm2/mm Hg is considered normal for the lower esophageal sphincter (LES) and more than 4 mm2/mm Hg considered normal for the upper esophageal sphincter (UES). Endoscopy revealed tiny white nummular lesions throughout the entire esophagus (Figure 2A). Biopsies were obtained. Histopathologic examination large polygonal cells with clear, vacuolated cytoplasm within the lamina propria and no increased intraepithelial eosinophils at any level of the esophagus. The appearance was consistent with heterotopic sebaceous glands (Figure 2B) [4]. Endo FLIP revealed poor distensibility of the lower and upper esophageal sphincters (Figure 3) and spastic motility pattern in the esophageal body (Figure 1A). Both the sphincters were dilated up to 20 mm with a through-the scope balloon. Other findings on EGD included an irregular squamocolumnar junction which on biopsy came back as non-dysplastic Barrett’s esophagus for which surveillance EGD was recommended in 3 years.
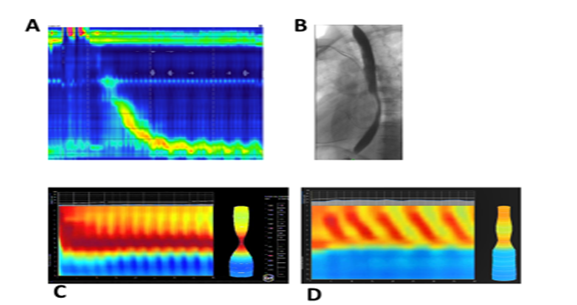
Figure 1: Multiple motility studies indicating impaired function. Esophageal manometry shows fragmented peristalsis (A). A barium esophageal revealed poor clearance of liquid from the esophageal body (B). Endo FLIP shows spastic motility pattern in the esophageal body (C). An example of normal esophageal motility by Endo FLIP is also shown (D)
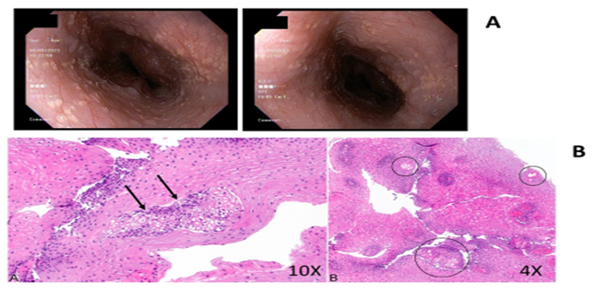
Figure 2: Upper endoscopy showing multiple yellow, raised, tiny lesions throughout the esophagus (A). Histological view of a hematoxylin and eosin-stained section revealing heterotopic sebaceous glands (B).
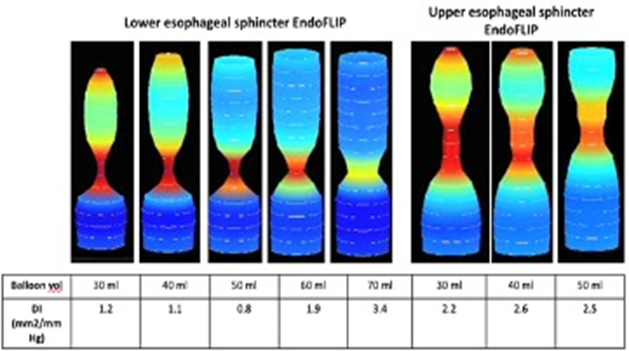
Figure 3: Endo FLIP of the lower and upper esophageal sphincters. Endo FLIP of the esophagus showing progressive distension of the lower esophageal and upper esophageal sphincters. The balloon volume refers to the volume in the Endo FLIP balloon and the distensibility index (DI) is a measure of the tightness of the sphincter. A DI between 3-9 mm2/mm Hg is normal for the lower esophageal sphincter and more than 4 mm2/mm Hg for the upper esophageal sphincter. The distensibility of both sphincters was less than normal in this patient.
Discussion
Sebaceous glands are rare in the esophageal mucosa with a reported prevalence of 0.005% to 0.05% [3,4]. They range from single lesions to over a hundred, from raised spots to plaques, and are predominantly found in the upper esophagus although they can occur anywhere in the esophagus [4]. Some cases may even have no distinguishable clinical lesions on EGD and may be found incidentally on biopsy [5]. A few studies have done follow-up endoscopies, and none have reported a malignant transformation [6,7]. It is unknown whether their presence has any significance and they do not appear to cause symptoms in most reported cases [3]. However, the lubricating, moisturizing, and anti-bacterial properties of sebum in the skin prompted further investigation into whether this represents metaplasia in the esophagus to perform these functions [1]. Ultimately, biopsy provided the definitive diagnosis, but it is worth discussing other causes of benign lesions in the esophagus. The differential diagnosis included candidiasis, squamous papilloma, glycogenic acanthosis and heterotopic gastric mucosa. Candidiasis was less likely given that this patient was immune-competent, but it remained high on the differential given the presentation of diffuse, yellow plaques [8]. Squamous papilloma commonly presents as a solitary, asymptomatic lesion, unlike multiple lesions found in our patient [9]. Glycogenic acanthosis shows up on endoscopy as multiple, uniformly sized, and round elevations, greater than 1 cm in diameter, which would look much different than the tiny lesions found [9]. A comprehensive literature review was conducted through a search of the PubMed database to identify and analyze all reported cases of heterotopic sebaceous glands. The initial query of “heterotopic or ectopic sebaceous glands” and “esophagus”’ identified 27 publications. An additional 6 articles with reported cases were identified during analysis of these publication. These 33 articles were further pared down to 22 after excluding publications that did not discuss biopsy-proven heterotopic sebaceous glands, were not in the English language, or did not present novel case reports. Reports published prior to 1990 and not otherwise listed in an earlier review of literature were not included. This identified 37 unique cases of esophageal ectopic sebaceous glands in the literature.
Table 1: Key Demographic, Clinical Description, Associated Symptomology and Functional Studies of Ectopic Sebaceous Glands in the Esophagus
| Study, year [ref.] | Case ID | Age | Gender | Race | Locatin |
| Park et.al, 20173 | 1 | 50 | Male | Asian | L |
| Park et.al, 20173 | 2 | 59 | Male | Asian | M |
| Park et.al, 20173 | 3 | 60 | Male | Asian | M |
| Park et.al, 20173 | 4 | 30 | Male | Asian | M |
| Park et.al, 20173 | 5 | 39 | Female | Asian | M |
| Hashimoto et. al, 20205 | 6 | 61 | Female | Unreported | NS |
| Hashimoto et. al, 20205 | 7 | 50 | Male | Unreported | NS |
| Hashimoto et. al, 20205 | 8 | 54 | Male | Unreported | NS |
| Hashimoto et. al, 20205 | 9 | 64 | Male | Unreported | NS |
| Hashimoto et. al, 20205 | 10 | 55 | Male | Unreported | NS |
| Hashimoto et. al, 20205 | 11 | 59 | Male | Unreported | NS |
| Hashimoto et. al, 20205 | 12 | 71 | Male | Unreported | NS |
| Hashimoto et. al, 20205 | 13 | 70 | Male | Unreported | NS |
| Fukuchi et. al, 20126 | 15 | 56 | Male | Asian | M+L |
| Lee et. al, 20147 | 14 | 45 | Female | Unreported | EE |
| Lee et. al, 20147 | 17 | 54 | Male | Unreported | M+L |
| Lee et. al, 20147 | 21 | 68 | Female | Unreported | EE |
| Lee et. al, 20147 | 22 | 59 | Male | Unreported | M |
| Lee et. al, 20147 | 23 | 44 | Female | Unreported | U+M |
| Lee et. al, 20147 | 29 | 44 | Male | Black | EE |
| Lee et. al, 20147 | 30 | 60 | Female | Black | L |
Conclusion
In summary, heterotopic sebaceous glands are a rare but benign finding in the esophagus. Their functional significance is unclear. Our case highlights the co-existence of HSGs with functional abnormalities in the esophagus. It is unknown whether HSGs develop in response to dysmotility or they simply coexist. Of note a prior EGD had not noted their presence, suggesting that HSGs may be overlooked during EGD. We hypothesize that presence of these glands was causing pruritus, coughing and throat clearing in his patient. Given no reported malignant potential, HSGs do not require surveillance. No specific treatment is available. HSGs should be considered in the differential diagnosis of tiny, elevated, yellowish or white lesions in the esophagus. Future studies should investigate the link between dysmotility and HSGs.
Disclosure
The authors report no conflicts of interest in this work.
References
- Hoover E, Aslam S, Krishnamurthy K. (2023). Physiology, Sebaceous Glands. In: Stat Pearls. StatPearls Publishing.
Publisher | Google Scholor - Zouboulis CC. (2004). Acne and sebaceous gland function. Clin Dermatol, 22(5):360-366.
Publisher | Google Scholor - Park A, Lee JH, Park A, et al. (2016). Prevalence rate and clinical characteristics of esophageal ectopic sebaceous glands in asymptomatic health screen examinees: Ectopic sebaceous gland in the esophagus. Dis Esophagus.
Publisher | Google Scholor - Yukihiro Nakanishi. (2023). Esophagus Congenital anomalies Heterotopic/ectopic sebaceous glands. Esophagus Congenital anomalies Heterotopic/ectopic sebaceous glands.
Publisher | Google Scholor - Hashimoto H, Horiuchi H, Miura S, Takayanagi S, Gunji T, Morikawa T. (2021). Clinicopathologic Characteristics of Esophageal Ectopic Sebaceous Glands: Chronological Changes and Immunohistochemical Analysis. Int J Surg Pathol, 29(4):378-384.
Publisher | Google Scholor - Fukuchi M, Tsukagoshi R, Sakurai S, et al. (2012). Ectopic Sebaceous Glands in the Esophagus: Endoscopic Findings over Three Years. Case Rep Gastroenterol, 6(1):217-222.
Publisher | Google Scholor - Lee SH, Lee DJ, Kim KM, Kim KN, Kang JK. (2014). Ectopic sebaceous glands in the oesophagus: a case report and review of literature. Scott Med J, 59(3):1-5.
Publisher | Google Scholor - Robertson KD, Nagra N, Mehta D. (2023). Esophageal Candidiasis. In: StatPearls. StatPearls Publishing.
Publisher | Google Scholor - Tsai SJ. (2015). Benign esophageal lesions: Endoscopic and pathologic features. World J Gastroenterol, 21(4):1091.
Publisher | Google Scholor - Bhat RV, Ramaswamy RR, Yelagondahally LKC. (2008). Ectopic sebaceous glands in the esophagus: a case report and review of literature. Saudi J Gastroenterol Off J Saudi Gastroenterol Assoc, 14(2):83-84.
Publisher | Google Scholor - Jeon MS, Kim GH, Jeong DY, et al. (2018). Magnifying Endoscopy for Esophageal Ectopic Sebaceous Glands. Clin Endosc, 51(5):495-497.
Publisher | Google Scholor - Hoshika K, Inoue S, Mizuno M, Iida M, Shimizu M. (1995). Endoscopic detection of ectopic multiple minute sebaceous glands in the esophagus: Report of a case and review of the literature. Dig Dis Sci, 40(2):287-290.
Publisher | Google Scholor - Thirunavukkarasu B, Nada R, Dawra S, Sinha SK. (2019). Ectopic sebaceous glands in oesophagus. BMJ Case Rep, 12(12):232736.
Publisher | Google Scholor - Montalvo N, Tapia V, Padilla H, Redrobán L. (2017). Heterotopic sebaceous glands in the esophagus, a very rare histopathological diagnosis: a case report and review of the literature. Clin Case Rep, 5(2):89-92.
Publisher | Google Scholor - Le A, Amin M, Cappell MS. (2019). Case Report of a Proposed, Novel, Endoscopic “Whitehead Pimple” Sign of Ectopic Esophageal Sebaceous Glands Based on Their Mimicking the Dermatologic and Histopathologic Characteristics of Cutaneous Whitehead Pimples/Closed Comedones. Dig Dis Sci, 64(7):2049-2053.
Publisher | Google Scholor - Kumagai Y, Makuuchi H, Ohmori T, Mukai M. (1993). Four Cases of Ectopic Sebaceous Glands Confirmed Endoscopically in the Esophagus. Dig Endosc, 5(3):238-244.
Publisher | Google Scholor - Peixoto A, Rodrigues S, Silva M, Maia T, Rios E, Macedo G. (2017). Esophageal ectopic sebaceous glands. Acta Gastro-Enterol Belg, 80(2):321.
Publisher | Google Scholor - Nakada T, Inoue F, Iwasaki M, Nagayama K, Tanaka T. (1995). Ectopic sebaceous glands in the esophagus. Am J Gastroenterol, 90(3):501-503.
Publisher | Google Scholor - Hoshihara Y, Hashimoto M, Yoshida Y, Hayakawa K, Fukuchi S, Unakami M. (1991). Ectopic Sebaceous Glands in the Esophagus: Report of Two Cases. Dig Endosc, 3(2):247-250.
Publisher | Google Scholor












