

Case Report
Giant Paraovarian Cyst in a Teenage Girl: A Case Report, Minimal Access Surgical Technique and Review of the Literature
- Moad Belouad 1*
- Hossin Oukili 1
- Abdelhamid Benlghazi 1
- Saad Benali 1
- Yassine Bouhtouri 1
- Hamza Messaoudia Abdelkrim Laalou 2
- MLY Mehdi Elhassani 1
- Jaouad Kouach 1
1Department of Gynecology and Obstetrics, Military Hospital of Instruction Mohamed V, Rabat.
2Department of visceral surgery, gynaecology, proctology and sterilisation oued eddahab military hospital, Morocco.
*Corresponding Author: Moad Belouad, Department of Gynecology and Obstetrics, Military Hospital of Instruction Mohamed V, Rabat.
Citation: Belouad M, Oukili H, Benlghazi A, Benali S, Bouhtouri Y, et, al. (2024). Giant Paraovarian Cyst in a Teenage Girl: A Case Report, Minimal Access Surgical Technique and Review of the Literature. Journal of Women Health Care and Gynecology, BioRes Scientia Publishers. 4(3):1-3. DOI: 10.59657/2993-0871.brs.24.068
Copyright: © 2024 Moad Belouad, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 12, 2024 | Accepted: December 13, 2024 | Published: December 21, 2024
Abstract
Paraovarian cyst are frequent and require imaging for diagnostic and sometimes surgical exploration. We report the surgical management of a giant paratubar cyst in a 16-year-old girl. The lesion is discovered in front of a significant abdominal distension. Magnetic resonance exploration shows a lesion evaluated at 25 cm. The usually benign nature of these lesions made us choose a minimally invasive surgery with a very short suprapubic laparotomy. The operative consequences were simple, the pathological examination confirming the benignity of the paraovarian cyst.
Keywords: paraovarian cyst; adolescent; MRI; surgery
Introduction
Background
Paratubal cysts are a frequent lesion, often confused with ovarian cysts when they are giant [1], generally benign but may be responsible for other complications: torsion [2], rupture, degeneration …
We report the case of a 16-year-old girl with a 25 cm paratubal cyst at the time of radiological exploration with minimal-access surgery.
Case Presentation
Miss Z, 16 years of age, with no notable medical or surgical history, had her menarche at 12 years of age with a regular cycle and no contraceptive methods, consulted with abdominal distension and a sensation of heaviness. Inspection revealed a distended abdomen, while palpation showed a supple abdomen with a painless mobile mass extending 05 cm beyond the umbilicus. The rectal examination provided little information (the vaginal examination was not performed: the patient claimed to be a virgin). Abdomino-pelvic ultrasound revealed a normal-sized uterus with homogeneous echostructure, the left ovary was unremarkable, and the right ovary was indistinct, with a latero-uterine mass measuring 26 cm, anechoic with a regular wall and no vegetations. A complementary MRI was requested, which revealed a well-limited abdomino-pelvic mass reaching the uterus, hypo signal T1 hyper signal T2 homogeneous with no fleshy component or vegetations nor enhancement after injection measuring 25x18x08 cm in favour of a simple ovarian cyst or serous cystadenoma.
Figure 1a & Figure 1b: MRI performed on a 16-year-old female patient with abdominal distension showing a large abdominopelvic mass with no fleshy component: a: frontal section; b: sagittal section.
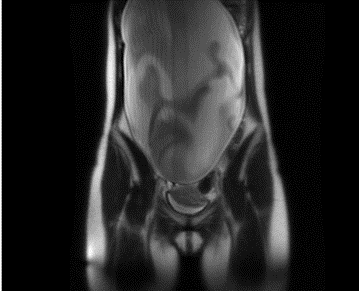
Figure 1a: frontal section.
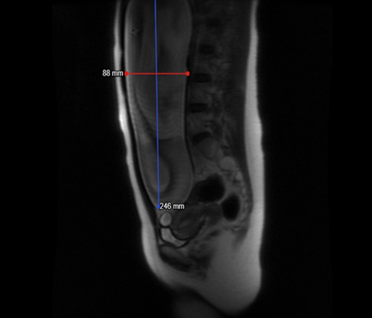
Figure 1b: sagittal section.
Tumor markers were negative, and given the usually benign nature of the mass, surgical exploration was decided under general anesthesia. We performed a suprapubic mini-laparotomy to explore the presence of a regular mass with minimal pelvic effusion. The left adnexa were unremarkable, while the right ovary was also normal and the mass was at the expense of the right tube, with the presence of a cleavage plane. We performed a cystectomy without salpingectomy, with peritoneal biopsies. The post-operative course was straightforward, and the patient resumed transit the following day, leaving the hospital on the third day.
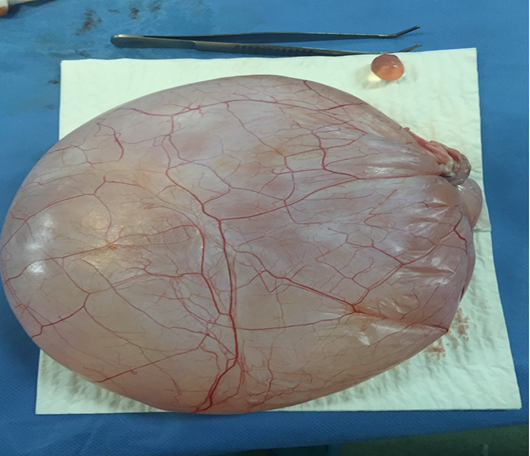
Figure 2: Paratubal cyst exteriorized after puncture in a 26-year-old girl.
Anatomopathological examination was in favour of a paratubal cyst and peritoneal biopsies with cytology of pelvic effusion fluid were without signs of malignancy.
Discussion
Paratubal cysts are common, representing around 13.1% of adnexal masses, compared with simple ovarian cysts (34%) and endometriomas (31%) [3]. Paratubal cysts are of parametronephrotic origin in 76% of cases; however, mesonephrotic and mesothelial origin are also found. In a histological study by Samaha and Woodruff, it was hypothesized that paratubal cysts may be diverticula of the normal Fallopian tube, due to the presence of a thin muscular layer around the cyst, and ciliated epithelium in the cysts [4]. Paratubal cysts are often discovered by chance or in the presence of digestive symptoms, and very rarely become complicated. However, neoplastic degeneration can sometimes occur, generally as papillary cystadenocarcinoma [5]. Most of these cysts cause light, non-specific symptoms, including abdominal distension or pain, a feeling of low abdominal pressure, and in some cases, symptoms affecting gastrointestinal or urinary transit. Usually incidental findings, but sometimes responsible for complications, notably torsion of para-tubal cysts bringing with them torsion of the tube [2].
Imaging is based on ultrasonography, which reveals a unilocular, spherical, thin-walled cyst with a hypoechoic, liquid-like appearance, with no intra-cystic septum or vegetation, combined with abdominal palpation: mobilization of the cyst allows it to be mobilized independently of the ovary, but ultrasonography is only used to make the diagnosis prior to surgery in 10% of cases, whereas in the majority of cases the lesion is considered to be of ovarian origin. [6]. MRI provides a better characterization of the cyst and, above all, enables the size of the cyst to be clearly defined, and to search for another cause of abdominal pain. In our patient's case, the MRI showed an ovarian cyst.
Operative treatment of these cysts varied according to the size of the cyst, generally by laparoscopy. In the case of small cysts measuring less than 3 cm, a simple puncture of the cyst can be performed with a micro-needle, followed by coagulation of the cyst with bipolar forceps. In the case of larger cysts, a complete extraction must be performed [7]. The difficulty of laparoscopic treatment lies in avoiding invasion of the cyst during laparoscopic trocar, transforming a limited tumour into a stage III tumour in the event of malignancy. In view of the giant size of the cyst and the reassuring radiological appearance, we performed a short suspubital laparotomy avoiding xyphopubic laparotomy
Conclusion
We conclude that paratubal cysts are rarely diagnosed. Ultrasound diagnosis of these cysts is not always feasible, and diagnosis requires recourse to MRI and even sometimes, in the presence of giant cysts, to laparoscopy, which must be cautious without cyst invasion and enables the most conservative treatment to be carried out, with a minimal suprapubic incision enabling cyst extraction avoiding a xyphopubic incision.
Declarations
Conflict of interest
No conflict of interest.
Funding
No funding
Consent
Informed written consent obtained from the patients.
References
- Letourneur B, Grandjean S, Richard P, Parant O. (2006). Prise en charge d'un kyste paratubaire géant. Gynécologie obstétrique & fertilité, 34(3):239-241.
Publisher | Google Scholor - Benkirane S, Alaoui FF, Chaara H, Bougern H, Melhouf MA. (2014). Twisted paratubal cyst : report of a rare case of difficult diagnosis. The Pan African Medical Journal, 19:25.
Publisher | Google Scholor - Seckin B, Ozdener T, Tapisiz OL, Batioğlu S. (2011). Laparoscopic treatment of ovarian cysts in adolescents and young adults. J Pediatr Adolesc Gynecol, 24(5):300-303.
Publisher | Google Scholor - Samaha M, Woodruff J. (1985). Paratubal cysts : frequency, histogenesis, and associated clinical features. Obstetrics and gynecology, 65(5):691-694.
Publisher | Google Scholor - Altaras MM, Jaffe R, Corduba M, Holtzinger M, Bahary C. (1990). Primary paraovarian cystadenocarcinoma: clinical and management aspects and literature review. Gynecologic oncology, 38(2):268-272.
Publisher | Google Scholor - Barloon TJ, Brown BP, Abu‐Yousef MM, Warnock NG. (1996). Paraovarian and paratubal cysts: preoperative diagnosis using transabdominal and transvaginal sonography. Journal of clinical ultrasound, 24(3):117-122.
Publisher | Google Scholor - Darwish AM, Amin AF, Mohammad SA. (2003). Laparoscopic management of paratubal and paraovarian cysts. JSLS: Journal of the Society of Laparoendoscopic Surgeons, 7(2):101.
Publisher | Google Scholor










