

Case Report
Giant Heart: A Case Report
1Faculty of Medicine, Department of Pulmonary & Critical Care, Lebanese University, Beirut, Lebanon.
2Department of Pulmonary & Critical Care, Beirut Cardiac Institute, Beirut, Lebanon.
3Department of Cardiology, Beirut Cardiac Institute, Beirut, Lebanon.
*Corresponding Author: El Mawla Zeinab, Faculty of Medicine, Department of Pulmonary & Critical Care, Lebanese University, Beirut, Lebanon.
Citation: El. M. Zeinab, D. Bilal, M. Malek, K. Hassan. (2024). Giant Heart: A Case Report, Clinical Research and Reports, BioRes Scientia Publishers. 2(2):1-5. DOI: 10.59657/2995-6064.brs.24.020
Copyright: © 2024 El Mawla Zeinab, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 27, 2023 | Accepted: January 23, 2024 | Published: February 06, 2024
Abstract
Introduction: Giant left atrium (LA), by definition >80 mm, is a rare disease with an incidence of 0.3% and is often associated with rheumatic mitral valve disease.
Case Presentation: A case of a 57-year-old female patient who underwent repeated mitral valve replacement and suffered from persistent atrial fibrillation, heart failure with dyspnea and lower extremity edema. A chest X-ray showed opacification of the right middle and lower lobes. Chest CT scan showed that the atrium occupied 80-90% of the right hemithorax, and the diagnosis of giant atrium was confirmed by echocardiography.
Conclusion: Giant left and right atriums are rarely seen and typically found in patients with mitral valve disease. It may be misdiagnosed as a pleural or pericardial effusion or mass lesion on CXR. Echocardiography is the gold modality to confirm its diagnosis. Mitral valve surgery with volume reduction remains the therapeutic options with favourable outcome.
Keywords: giant atriums; mitral valve replacement; echocardiography; Lebanon; case report
Introduction
Giant left atrium (LA) is a rare disease with an incidence of 0.3%, by definition >80 mm in length, and is often associated with rheumatic mitral valve disease [1,2]. In general, 1) chronic pressure or volume overload due to mitral valve disease and/2) involvement of the LA wall due to rheumatic pan carditis, and 3) concurrent atrial fibrillation are thought to be responsible for severe LA enlargement [3]. We are presenting an adult case of giant LA and RA associated with persistent atrial fibrillation and severe functional mitral stenosis (MS) without evidence of rheumatic mitral valve disease.
Case Presentation
A 57-year-old female patient presented with increased dyspnea, shortness of breath, and lower extremity edema over the past 2 weeks. She is a heavy smoker and has a history of hypertension, persistent atrial fibrillation, and heart failure with reduced ejection fraction (40%). She underwent an unexplained mitral valve replacement when she was 18 years old; repaired twice on her 25 years old and 50 years old. No further medical information was available during her hospitalization.
Physical examination revealed dilated jugular veins, hypoxemia with oxygen saturation of 82% on room air, loss of breath sounds in the right middle lung zone and lower lung zone, lower extremity edema of 2 or more, and an apical prosthetic valve revealed a grade 2/6 holosystolic murmur.
Laboratory studies showed a brain natriuretic peptide level of 1527 pg/ml with an international normalized ratio of 5.87. Arterial blood gas analysis revealed hypoxemia and respiratory acidosis with PaCO2 of 55 mm Hg, and chest X-ray (CXR) showed complete opacification of the right middle to lower lung region and cardiomegaly (Figure 1).
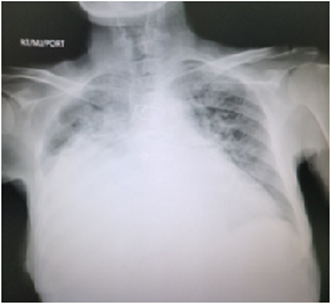
Figure 1: Chest X-ray (CXR) revealed complete opacification of right mid-to-lower lung zones and cardiomegaly.
His CT scan of the chest (Figure 2) was performed due to concern for a right thoracic mass or a large right pleural effusion. Results revealed severe cardiac hypertrophy with the atrium occupying 80–90% of the right hemithorax. Transthoracic echocardiogram (TTE) shows global enlargement of the left atrium (Figure 3), left ventricular ejection fraction 15%, normally functioning prosthetic mitral valve (Figure 4), with severe enlargement of the right ventricle (RV) was demonstrated and decreased RV function, mild pulmonary hypertension (systolic pulmonary artery pressure 40 mm Hg) and severe tricuspid regurgitation. She was admitted to the cardiac ward and her diuretics were started until her symptoms improved. The patient was then discharged home for follow-up in the outpatient clinic.

Figure 2: CT chest showed severe cardiomegaly where the atriums occupy 80-90% from the right hemithorax.
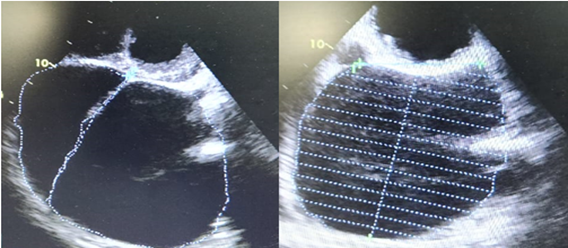
Figure 3: A transthoracic echocardiogram (TTE) showed severe left atrial enlargement.

Figure 4: A transthoracic echocardiogram (TTE) showed severe tricuspid valve regurgitation.
Discussion
Giant left atrium (GLA) is a rare disease with an incidence of 0.3% and is a long-term consequence of rheumatic heart disease with mitral valve-related complications [1]. It is rare in developed countries. GLA is recognized when the cardiothoracic ratio is >0.7 on CXR, the antero-posterior atrial wall diameter is >80 mm on chest CT, and the diameter recorded on M-mode TTE is >65 mm [2,4]. CXR findings of GLA are usually inconclusive. It may be misdiagnosed as a chest mass or pleural effusion. A careful and detailed examination of the CXR (anteroposterior and lateral views) often helps optimize the differential diagnosis. A markedly enlarged heart silhouette, widened tracheal carina angle (>70°), normal posterior costophrenic angle, and walking man’s sign are some important features that can be used to suspect the presence of GLA. Ignoring these CXR results and performing a biopsy or thoracentesis without additional imaging may result in unintended harm. This case highlights the correlation between medical history and CXR results and therefore the importance of evaluating the patient with a more detailed examination before performing an invasive procedure.
GLA is the result of volume overload due to severe sustained pressure and commonly occurs in mitral stenosis and mitral regurgitation, but also rarely occurs in mitral valve prolapse in long-standing rheumatic mitral valve disease. GLA commonly occurs in atrial fibrillation, hemodynamic and/or respiratory complications due to adjacent organ compression symptoms. Cases of dysphagia and Ortner syndrome have also been reported in some cases.5 However, a small number of cases may be asymptomatic.
The main complication of a giant left atrium is thromboembolism. Numerous examples are described in the literature. Before the widespread use of echocardiography, a large thrombosed left atrium was hidden as a mediastinal tumor [6]. Echocardiography allowed the association of left atrial thrombus with a large left atrium. This complication has been reported in patients before and after mitral valve replacement [7,8]. Kutay et al [9] reported the incidence of thromboembolic events in patients with and without a giant left atrium after mitral valve replacement without a left atrial fold. Incidence was similar in both groups and was associated with lower socioeconomic status leading to nonadherence to anticoagulant therapy. Anticoagulant therapy can effectively prevent thromboembolic complications in cases of bulky left atrium. Therefore, initiation of anticoagulation therapy is an indication of a gigantic left atrium.
Our patient showed no signs of thromboembolism. She received anticoagulation therapy and her international normalized ratio increased to 5.87.
The goals of giant left atrial surgery are to correct mitral valve abnormalities, prevent thromboembolism, restore atrial fibrillation to normal sinus rhythm, and treat compression symptoms [5].
Her two strategies are used to treat mitral valve surgery with an enlarged left atrium. The first is mitral valve surgery alone and the second is mitral valve surgery with left atrial volume reduction.
The presence of intracardiac or extracardiac compressive symptoms is the main indication for volume reduction. However, some experts believe that if mitral valve surgery alone is successful, the size of the left atrium will eventually decrease due to a reduction in volume and mean atrial pressure. The surgeon who performed the reduction of the left atrium was convinced that the effect of rheumatism on the elastic fibers of the tissue is irreversible. This process leads to overexertion and loss of tone. Therefore, enlargement of the left atrium cannot be reversed. They confirmed that by replacing the mitral valve and reducing the size of the left atrium, the influence of pressure was reduced and had a positive impact on the postoperative course [5].
The presence of blood clots and a history of thromboembolic events is the second indication for volume reduction. Reducing left atrial volume could theoretically reduce intraatrial stasis and prevent recurrent thrombosis. However, these can be difficult to recognize because such patients are already taking warfarin. Additionally, a large atrial size reduces the success rate of cardioversion and increases thromboembolic risk [5].
A giant right atrium [10,11] can be due to Ebstein anomaly, pulmonary hypertension or tricuspid regurgitation. In our case, the right atrial enlargement was the result of pulmonary hypertension as a consequence of severe tricuspid regurgitation and mitral stenosis.
Conclusion
Nowadays, giant left and right atriums are rarely seen and require a high degree of suspicion. It usually occurs in patients with mitral valve disease. Currently, routine CXR alone cannot accurately diagnose the large left atrium. It may be misdiagnosed as a pleural effusion, pericardial effusion, or mass lesion. Echocardiography is an excellent method to confirm the diagnosis, assess the etiology, and guide appropriate treatment. Minimally invasive mitral valve replacement strategies remain an active research topic and may provide better treatment options for high-risk patients.
Declarations
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review upon request by the Editor-in-Chief of this journal.
Ethics Approval and Consent to Participate
Ethical approval was not applicable.
Conflict of Interest
The authors declare that they have no conflict of interest.
Financial Disclosure
The authors declared that this study has received no financial support.
Authors’ Contributions
Malek Moussa (MM) and Hassan Kazem (HK) contributed to the management of the case. Zeinab El Mawla (ZM) and Bilal Damen (BD) contributed to the conceptualization and planning of the case report. ZM provided the preparation of manuscript. All authors read and approved the final manuscript.
Acknowledgments
Not applicable.
Provenance and Peer Review
Not commissioned, externally peer reviewed.
References
- Ahmed El Maghraby RH. (2012). Giant Left Atrium: A Review. Hear Views, 13(2):46-52.
Publisher | Google Scholor - G P Piccoli, C Massini, G Di Eusanio, L Ballerini, G Iacobone, A Soro AP. (1984). Giant left atrium and mitral valve disease: early and late results of surgical treatment in 40 cases. J Cardiovasc Surg, 25(4):328-336.
Publisher | Google Scholor - Hurst JW. (2001). Memories of Patients with a Giant Left Atrium. 104:2630-2631.
Publisher | Google Scholor - Oh JK. (1992). Echocardiographic evaluation of morphological and hemodynamic significance of giant left atrium. 86(1):328-330.
Publisher | Google Scholor - Efstratios Apostolakis JHS. (2008). The surgical management of giant left atrium. Eur J Cardiothorac Surg, 33(2):182-190.
Publisher | Google Scholor - P R Schvartzman RDW. (2001). Giant left atrium. 104(6):28-29.
Publisher | Google Scholor - Kaan Okyay, Atiye Cengel YT. (2007). Images in cardiology. A giant left atrium with two huge thrombi without embolic complications. Can J Cardiol, 23(13):1088.
Publisher | Google Scholor - Bogdan A Popescu, Ioana Lupescu, Serban Al Georgescu CG. (2010). Giant left atrium with calcified walls and thrombus in a patient with an old, normally functioning ball-in-cage mitral valve prosthesis. 122(24):579-580.
Publisher | Google Scholor - Veysel Kutay, Kaan Kirali, Hasan Ekim CY. (2005). Effects of giant left atrium on thromboembolism after mitral valve replacement. Asian Cardiovasc Thorac Ann, 13(2):107-111.
Publisher | Google Scholor - Vignendra Ariyarajah, Anita Soni AM. (2008). Giant right atrium in an adult. Echocardiogr, 25(10):1121-1123.
Publisher | Google Scholor - Sean Gomes, Hugh Wolfenden JL. (2012). Giant right atrium in an adult: case report of a rare condition. Hear Lung, 21(1)50-52.
Publisher | Google Scholor













