

Case Report
Giant Adenofibroma of The Breast in A 50-Year-Old Woman: Case Report
- Nassima Ouguerzi *
- Samia Bennaceur
- Othmane Echarfaoui
- Moad Belouad
- Moulay Mehdi Elhassani
- Jaouad Kouach
Department of Gynecology-Obstetric, Military Training Hospital Med V, Faculty of Medicine and Pharmacy, Mohammed V University, Rabat, Morocco.
*Corresponding Author: Nassima Ouguerzi, Department of Gynecology-Obstetric, Military Training Hospital Med V, Faculty of Medicine and Pharmacy, Mohammed V University, Rabat, Morocco.
Citation: Ouguerzi N, Bennaceur S, Echarfaoui O, Belouad M, Elhassani M. M, et al. (2024). Giant Adenofibroma of The Breast in A 50-Year-Old Woman: Case Report, Clinical Obstetrics and Gynecology Research, BioRes Scientia Publishers. 3(2):1-3. DOI: 10.59657/2992-9725.brs.24.012
Copyright: © 2024 Nassima Ouguerzi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 04, 2024 | Accepted: March 25, 2024 | Published: April 05, 2024
Abstract
Adenofibroma of the breast is a benign tumor common in young women, developing under the influence of hormonal variations and regressing spontaneously after the menopause. We report the case of a 50-year-old woman who presented with a palpable mass in the right breast, measuring 11 cm in diameter, mobile, firm and smooth, with clear contours and no functional signs or associated adenopathy. Radiological examinations showed a well-limited, hypoechoic nodular lesion, without microcalcifications. Biopsy confirmed the diagnosis of breast adenofibroma. The patient underwent tumorectomy, with an adequate safety margin. Histological examination confirmed the benign nature of the tumor, with no atypia or malignancy. Patient follow-up was unremarkable, with no recurrence or complications. We discuss the clinical, radiological, histological and therapeutic features of adenofibroma of the breast, as well as the differences with other breast tumors, in particular phyllodes tumor, which is a rare tumor that can reach large sizes and has the potential for recurrence and malignancy.
Keywords: adenofibroma of the breast, benign tumor, phyllodes tumor
Introduction
A breast adenofibroma, also known as a fibroadenoma or fibroma of the breast, is a benign tumor that develops from the mammary gland. It is composed of a proliferation of both glandular epithelial cells and conjunctive tissue cells [1]. Breast adenofibromas are the most common benign tumors of the breast, accounting for around 50% of palpable breast lesions in women under 30[2]. It can occur at any age, but peaks between the ages of 15 and 35 [2]. It is rare after the menopause, except in the case of hormone replacement therapy [3]. Adenofibromas of the breast most often manifest as a palpable mass in the breast, of variable size, mobile, smooth, firm, with clear contours, without functional signs or associated adenopathy. It may be single or multiple, unilateral or bilateral. It is sensitive to hormonal variations, increasing in volume during pregnancy or breast-feeding, and decreasing after the menopause [4]. There are no known risk factors for breast adenofibromas, nor any link with breast cancer [5]. We report the case of a 50-year-old woman who presented with a giant adenofibroma of the breast, measuring 11 cm in diameter, which was treated by tenonectomy.
Case Presentation
A 50-year-old female patient presented for consultation with a palpable mass in the right breast, discovered 3 months ago. She reports no personal or family history of breast cancer, and no history of hormone replacement therapy. She has no associated functional signs, such as pain, nipple discharge or skin changes. Clinical examination revealed a swelling in the upper-external quadrant of the right breast, measuring approximately 11 cm in diameter, mobile, smooth, firm, with clear contours and no axillary or supra-clavicular adenopathy. The left breast and the rest of the examination were normal (Figure 1).

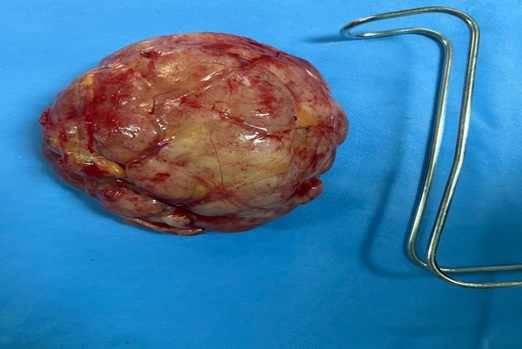
Figure 1
A mammogram and breast ultrasound were performed, showing a well-limited, hypoechoic nodular lesion with no microcalcifications or abnormal vascularization. The rest of the breast parenchyma was of normal density, with no focal abnormalities or suspicious nodes. Biopsy reveals normal epithelial and connective cells, without atypia or malignancy. The diagnosis of breast adenofibroma is made. The patient is informed that the lesion is benign, but also that it is large enough to warrant surgical removal. She gives her informed consent for a tumorectomy, which is performed under general anesthesia, with a short hospital stay. The operation is uncomplicated, and the tumour is removed in its entirety, with an adequate safety margin Histological examination confirmed the benign nature of the tumour, with no atypia or malignancy (Figure 2).
The patient is seen in post-operative consultation, and presents no pain or complications. She is satisfied with the esthetic result. She is informed of the need for regular surveillance by clinical examination and breast imaging, to detect any other benign or malignant lesions of the breast.
Discussion
Adenofibroma of the breast is a benign tumour common in young women, which develops under the influence of hormonal variations and regresses spontaneously after the menopause. It usually appears as a palpable mass in the breast, of variable size of variable size [2], mobile, smooth, firm, with clear contours and no functional signs or associated adenopathy. Diagnosis is based on clinical examination, breast imaging and biopsy. Treatment should be conservative, depending on the characteristics of the tumour and the patient's choice. We report the case of a 50-year-old woman who presented with a giant adenofibroma of the breast, measuring 11 cm in diameter, which was treated by lumpectomy. This is a rare case, as adenofibromas of the breast are usually small (lessthan 3 cm) [6], and are uncommon after menopause, except in cases of hormone replacement therapy. The patient had no risk factors or signs of malignancy. Surgical excision confirmed the diagnosis and treated the tumour, with a satisfactory esthetic and functional outcome. In a retrospective study of giant breast masses over a 20-year period (1980-2000), RM Hannab et al met 18 patients with fibroadenomas. The majority were adolescents and young adults. The bimodal age incidence seen in Caucasians was not found. Masses varied in size from 6 to 15 cm [7].
Adenofibromas of the breast must be distinguished from other breast tumors, in particular from phyllodes, a rare tumor that can grow to large size, with the potential for recurrence and malignancy. Phyllodes tumors develop from the breast stroma, not the gland. It appears as a palpable mass in the breast, rapidly growing, irregular, hard, adherent to the deep planes, sometimes with inflammatory or haemorrhagic signs. Imaging shows a poorly defined, heterogeneous nodular lesion, with necrotic or hemorrhagic areas, and abnormal vascularization. Biopsy is essential to confirm the diagnosis and determine the histological grade of the tumor, which determines prognosis and treatment [8]. Phyllodes tumors are treated surgically, by mastectomy or wide lumpectomy, with a large safety margin. There is no effective adjuvant treatment, either chemotherapy or radiotherapy. The prognosis of phyllodes tumors depends on the histological grade, the status of surgical margins and the presence or absence of metastases. The rate of local recurrence is high, especially for high-grade tumors, and the rate of distant metastases is 10-20% [9].
Conclusion
Adenofibroma of the breast is a benign tumour common in young women, which develops under the influence of hormonal variations and regresses spontaneously after the menopause. It usually manifests itself as a palpable breast lump of variable size. Diagnosis is based on clinical examination, breast imaging and biopsy. The prognosis is excellent, with no risk of malignant transformation or recurrence after removal. Breast adenofibromas must be distinguished from other breast tumours, in particular from phyllodes, a rare tumour that can grow to large size, with the potential for recurrence and malignancy.
Declarations
Conflict of Interest
No conflict of interest.
Funding
No funding.
Consent Informed
Written consent obtained from the patient.
References
- Morris A, Shaffer K. (2007). Recurrent Bilateral Giant Fibroadenomas of The Breasts. Radiology Case Reports. 2(3):96.
Publisher | Google Scholor - Organ Jr CH, Organ BC. (1983). Fibroadenoma of the Female Breast: A Critical Clinical Assessment. Journal of the National Medical Association. 75(7):701.
Publisher | Google Scholor - Stachs A, Stubert J, Reimer T, Hartmann S. (2019). Benign Breast Disease in Women. Deutsches Ärzteblatt International. 116(33-34):565.
Publisher | Google Scholor - Paepke S, Metz S, Brea Salvago A, Ohlinger R. (2018). Benign Breast Tumours-Diagnosis and Management. Breast Care. 13(6):403-412.
Publisher | Google Scholor - Dupont WD, Page DL, Parl FF, Vnencak-Jones CL, Plummer WD, et al. (1994). Long-Term Risk of Breast Cancer in Women with Fibroadenoma. N Engl J Med. 331(1):10-15.
Publisher | Google Scholor - Park CA, David LR, Argenta LC. (2006). Breast Asymmetry: Presentation of A Giant Fibroadenoma. The Breast Journal. 12(5):451-461.
Publisher | Google Scholor - Hanna R, Ashebu S. (2002). Giant Fibroadenoma of The Breast in An Arab Population. Australasian Radiology. 46(3):252-256.
Publisher | Google Scholor - Panda KM, Naik R. (2016). A Clinicopathological Study of Benign Phyllodes Tumour of Breast with Emphasis on Unusual Features. Journal of Clinical and Diagnostic Research: JCDR. 10(7):EC14.
Publisher | Google Scholor - Paepke S, Metz S, Brea Salvago A, Ohlinger R. (2018). Benign Breast Tumours-Diagnosis and Management. Breast Care (Basel). 13(6):403-412.
Publisher | Google Scholor











