

Case Report
Extensive Pneumobilia Secondary to a Benign Cause
1 Department of General Surgery, King Fahad Hospital, Dammam, Saudi Arabia.
2 Department of Paediatric Surgeon, Head of Paediatric Surgery, King Fahad Hospital, Dammam, Saudi Arabia.
*Corresponding Author: Alsaif Farah, Department of General Surgery, King Fahad Hospital, Dammam, Saudi Arabia.
Citation: Farah A, Abdullah A. (2023). Extensive Pneumobilia Secondary to a Benign Cause. Journal of Clinical Surgery and Surgical Research, BioRes Scientia Publishers. 2(2). DOI: 10.59657/2992-9989.brs.23.010
Copyright: © 2023 Alsaif Farah, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 30, 2023 | Accepted: May 12, 2023 | Published: May 16, 2023
Abstract
Pneumobilia is presence of air within biliary tree, there are several causes which can be iatrogenic or non-iatrogenic. We report a case of a 15- year-old boy presenting with typical symptoms of gastric outlet obstruction with finding of extensive pneumobilia on imaging, he underwent surgical exploration to relieve high grade obstruction and rule out ischemia. Spontaneous pneumobilia is rare but often present in a benign course. Conservative management is usually suitable after ruling out life threating conditions.
Keywords: pneumobilia; 15- year-old boy; gastric outlet; surgical exploration
Introduction
Pneumobilia is defined as air within the biliary tree, most of which is iatrogenic. It could represent an underlying life-threatening pathology. There are some reported cases of spontaneous pneumobilia which represent a rare, usually benign entity. Diagnosis is usually by imaging modalities. Identifying the cause is crucial and direct the management plan. We report a case of gastric outlet obstruction in a 15-year-old boy with concurrent extensive pneumobilia that turned out to be of a benign entity.
Case presentation
A 15-year-old male k/c of celiac disease, eosinophilic esophagitis and multiple food allergies. Presented to ER with sudden severe abdominal pain for 2 hours duration, 10/10 in severity radiating to his back associated with abdominal distension, nausea and vomiting of undigested food, he has no history of change in bowel motion, passing flatus, he is non-compliant to his diet and medications. He had history of similar presentation for which he has been admitted as case of gastric outlet obstruction, treated with pulse steroids and underwent duadenoplasty 6 months prior to this visit.
On examination; he was in pain but not in respiratory distress, with vital signs Blood pressure 128/91, heart rate of 120, afebrile and sating well on room air, his abdomen was distended, tense and tender. Investigations showed CRP 0.5, WBC 7.7, Hemoglobin of 13, lipase 19, lactate initially was 2 on venous blood gas and repeated from plasma was 5. His liver function test and renal were within normal ranges, chest x-rays showed hugely distended stomach. Patient was kept NPO and IV fluid initiated and nasogastric tube inserted; patient was improved dramatically after NGT and fluid resuscitation. Contrast enhanced CT scan revealed huge distension of the stomach with transition at the distal pylorus, associated with development of pylorus mural thickening, in addition to gastric pneumatosis, extensive pneumobilia, suggestive of an advanced gastric outlet obstruction. In view of that Patient was taken for exploratory laparotomy to relieve gastric outlet obstruction and rule out a life-threatening cause of pneumobilia and found to have distended stomach reaching pelvis with good vascularity and no signs of ischemia along with area of previously deudenoplasty is thickened inflamed with no evidence of a fistula. The whole bowel was healthy and no abdominal collection. Gastrojejunostomy was done to bypass the stenotic area, and feeding jejunostomy performed. Patient had uneventful post-operative course.
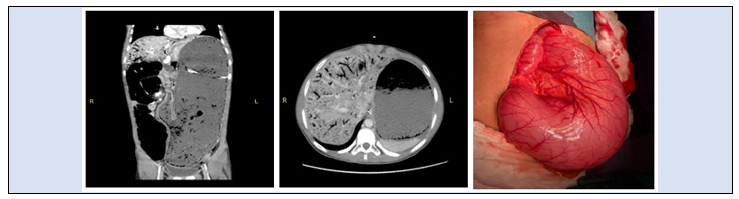
Figure: Intra-operative image showing distended stomach with no signs of ischemia
Discussion
Intra-biliary air is an ominous finding. Etiologies of such finding are divided into iatrogenic due to enter biliary system interventions i.e ERCP, surgical enter biliary fistula, or non-iatrogenic causes which include trauma, malignancy, sphincter of Oddi dysfunction, infections namely gas forming organisms in association with emphysematous cholecystitis, pyelonephritis and intestinal tuberculosis and rarely biliary brocho-plural fistula [1,2,3]. Presence of portal vein gas mandates excluding life threating conditions as bowel wall ischemia, gas gangrene or pyogenic liver abscess [4,5,6]. Nevertheless, several benign causes of portal vein gas have been identified, including gastric pneumatosis, ulcerative colitis, barium enemas, liver transplantation and CPR [7]. Differentiating pneumobilia from portal vein gas is important, the air in pnumobilia is in the direction of the bile flow, and has fewer branches. On x-rays this is known as Sabre sign, in contrast pneumatosis portalis is retrograde to the bile flow, extending both to the hepatic hilum and toward Glisson capsule and exhibit tree-like appearance in the periphery on imaging [8,9]. In our case, the patient presented with gastric outlet obstruction symptoms with imaging finding of what looks like gastric pneumatosis and pneumobilia. Gastric pneumatosis known as gastric emphesema is presence of air inside the stomach wall. Etiologies of gastric pneumatosis include gastric outlet obstruction, severe vomiting, trauma and ischemia. It is mostly described in contest of hypertrophic pyloric stenosis in infant [10]. The pathophysiology is due to breach in gastric mucosal integrity with increase in intraluminal pressure due to obstruction or trauma; the air dissects the gastric wall giving fining of gastric pneumatosis [11]. Presence of portal vein gas in concurrent in gastric outlet obstruction occurs due to presence of incompetent sphincter of Oddi or development of spontoons biliary-enteric fistula exacerbated by increase enteric intraluminal pressure. Entero-biliary fistulas are mostly asymptomatic and cholangitis occurs in < 10>
Treatment options depends on patient stability, and as most of the patient pneumobilia is incidentally found on imaging and usually asymptomatic, conservative management with follow ups and endoscopic procedure is almost always recommended. Enter biliary fistulas related to PUD usually closes spontaneously with anti- ulcer treatment [12], surgery is reserved to hemodymically unstable or patient with poorly controlled or recurrent PUD complication or biliary obstruction not resolving with drainage procedure. An exclusion gastro jejunostomy with bill roth II gastrectomy has been recommended (13), In cases of biliary obstruction, biliary decompression and internal drainage like cholecystic duodenostomy or Roux- en-Y drainage can be formed.
In our case, the patient was clinically stable but with imaging findings and high-grade pyloric obstruction, we elected to take the patient for surgery and bypassing procedure in the form of gastrojejunostomy and feeding jejunostomy tube, performed. For the pneumobilia patient may need further workup to precisely delineate the biliary tree as MRCP and endoscopy.
Conclusion
Pneumobilia could represent a range of different pathologies. Life threatening conditions should be ruled out. Benign conditions should be kept in mind and management will depend on the cause.
Acknowledgment
No conflict of interest.
References
- Yeniocak S, Az A, Canıpek E, Ekinci Biçkici B, Metiner M & Demirel A. (2019). A rare case: Asymptomatic spontaneous pneumobilia. Journal of Surgery and Medicine.
Publisher | Google Scholor - Wu CC, Hung SF. (2012). Severe emphysematous pyelonephritis combined with pneumobilia. Emerg Med J. 29(11):938.
Publisher | Google Scholor - Alvi AR, Zaidi M. (2008). A unique variant of intestinal tuberculosis. J Coll Physicians Surg Pak. 18(10):657-659.
Publisher | Google Scholor - Sheikh, A. A., Ahmed, khalid H., Avula, S., Shah, N. J., & Aloysius, M. M. (2021). Spontaneous pneumobilia: Not so benign. Cureus.
Publisher | Google Scholor - Gosink BB. (1981). Intrahepatic gas: differential diagnosis. AJR Am J Roentgenol. 137:763-767.
Publisher | Google Scholor - Meyns E, Vermeersch N, Ilsen B, Hoste W, Delooz H, Hubloue I. (2009). Spontaneous intrahepatic gas gangrene and fatal septic shock. Acta Chir Belg. 109:400-404.
Publisher | Google Scholor - Alataby H, Daniel M, Bibawy J, Diaz K & Nfonoyim, J. (2020). Gastric emphysema and hepatic portal vein gas as complications of noninvasive positive pressure ventilation. Cureus.
Publisher | Google Scholor - Rajković Z, Papes D, Altarac S, Arslani N. (2012). Abdominal pain and two x-rays: spot the difference. Ann R Coll Surg Engl. 94(2):95.
Publisher | Google Scholor - Lewandowski BJ, Withers C, Winsberg F. (1984). The air-filled left hepatic duct: the saber sign as an aid to the radiographic diagnosis of pneumobilia. Radiology. 153(2):329-332.
Publisher | Google Scholor - Ebrahimian M, Ghayebi N & Rezaee S. P. (2021). Gastric pneumatosis and concurrent Aeroportia due to gastric outlet obstruction: A case report. International Journal of Surgery Case Reports. 89:106584.
Publisher | Google Scholor - Angelino V, Volpicelli G, Cardinale L. (2017). Gastric emphysema after intubation. J Belg Soc Radiol. 101:3.
Publisher | Google Scholor - Thyssen EP, Weinstock LB, Balfe DM, Shatz BA. (1993). Medical treatment of benign gastrocolic fistula. Ann Intern Med. 118:433-5.
Publisher | Google Scholor - Kakked G. A, Bhatt N. R & Bhatt R. (2015). Pneumobilia with gastric outlet obstruction. BMJ Case Reports.
Publisher | Google Scholor














