

Research
Efficacy of the use of Cervical Epidural Anesthesia in Shoulder Girdle Surgery
1Specialist in Anesthesiology and Resuscitation. Instructor Teacher. Martín Chang Puga Teaching General Hospital. University of Medical Sciences of Camagüey. Camaguey. Cuba.
2Medical student, Martín Chang Puga Teaching General Hospital. University of Medical Sciences of Camagüey. Camaguey. Cuba.
*Corresponding Author: Yuliel Varona Rodriguez,Specialist in Anesthesiology and Resuscitation. Instructor Teacher. Martín Chang Puga Teaching General Hospital. University of Medical Sciences of Camagüey. Camaguey. Cuba
Citation: : Yuliel V Rodriguez, L.M.C. Manresa. (2023). Efficacy of the use of cervical epidural anesthesia in shoulder girdle surgery. Journal of Surgical Case Reports and Reviews. BRS Publishers. 2(2); DOI: 10.59657/2993-1126.brs.23.013
Copyright: © 2023 Yuliel Varona Rodriguez, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 21, 2023 | Accepted: July 08, 2023 | Published: July 17, 2023
Abstract
Introduction: The study of the efficacy of the cervical epidural block in shoulder girdle surgery allows us to identify the most frequent complications in order to prevent them and to be able to compare this technique with others.
Objective: To describe the efficacy of the use of cervical epidural anesthesia in shoulder girdle surgery.
Methods: Observational, descriptive and cross-sectional study at the Martín Chang Pug Teaching General Hospital in the Neuritis municipality, Camagüey province, between January 2021 and December 2022. The sample consisted of 25 patients undergoing shoulder girdle surgery who underwent surgery. Cervical epidural anesthesia was applied.
Results: There was a predominance of males (18 out of 25 patients), and most of the patients were between 19 and 59 years old. Patients classified as ASA II (17 patients) predominated. Heart rate and mean arterial pressure followed a Gaussian distribution at 30 and 60 min after starting the cervical epidural block (df: 25; p>0.05). Both heart rate, mean arterial pressure, and partial oxygen saturation decreased significantly 60 min after the anesthetic technique was applied, but remained within normal limits. 100% of them reported having felt satisfied with the anesthetic procedure.
Conclusions: The hemodynamic values remained within normal limits in the first hour of the intraoperative period, and all the patients were satisfied with the results of the analgesia achieved by this method. The use of cervical epidural anesthesia in shoulder girdle surgery is effective and safe.
Keywords: cervical epidural anesthesia; shoulder girdle surgery; upper limb surgery; anesthetic cocompletions
Introduction
The use of anesthesia and epidural analgesia was introduced in 1901 by the Frenchmen Jean Athanasy Sicard and Ferdinand Cathelin. Over the years, several modifications have been made to the contribution of these doctors. Among others, those related to the methods of application, the access routes, the required doses and even the quality of the anesthetics used. All these changes have allowed anesthesiologists to take advantage of their advantages [1]. The type of regional anesthesia at the neuraxial level called, indistinctly, as epidural, extradural or epidural anesthesia consists of the introduction of a local anesthetic agent, or other drug for such purposes, into the epidural space, in order to block the nerve endings at their exit from the spinal cord [2]. In Cuba this method has been used successfully for several years, thanks to its few complications and the infrequency with which they occur. However, there are not many anesthesiologists who use it, either because they have little confidence or ability to perform this procedure [3]. Some of the general complications related to the cervical epidural block technique are hypotension, bradycardia, respiratory depression, and the most frequent neurological complications are post-puncture headache and transient neurological syndrome, therefore, every anesthesiologist should be aware of the possibility of developing them and take the necessary preventive measures, Especially in patients in whom puncture is difficult, adapting anesthetic techniques and appropriate drugs, thus improving the quality of anesthesia administered [4]. However, this type of blockis used with high safety rates in a wide variety of procedures, such as cesarean sections [5]. lower limb surgery [6]. upper limb and shoulder girdle surgery and thyroid surgery [7,8]. This is because its use allows to avoid in many occasions the use of endotracheal general anesthesia, with all the complications related to the management of the airway and the use of sedatives, neuro-muscular relaxants and opioid analgesics parenterally. The study of the efficacy of cervical epidural block in shoulder girdle surgery allows us to identify which are the most frequent complications to prevent them and to compare this technique with others, which allows us to choose the anesthetic method based on its effectiveness and safety, always taking into account the anesthetic quality and the patient's satisfaction with the analgesia received. Taking into account that some of the most serious general complications derive from respiratory and cardiovascular depression due to autonomic nerve block, this study will evaluate vital signs and their behavior during the trans operative period. Therefore, the objective of this study was to describe the efficacy of the use of cervical epidural anesthesia in shoulder girdle surgery.
Methods
An observational, descriptive, longitudinal and prospective study was conducted at the Martín Chang Puga Teaching General Hospital in the municipality of Nuevitas, province of Camagüey, between January 2021 and December 2022.The universe consisted of31 patients undergoing shoulder girdle surgery with open reduction and internal fixation, in which cervical epidural anesthesia was used in the study period. An intentional non-probabilistic sampling was applied by investigator's criteria, in which 6 patients did not meet the inclusion criteria, so the sample was made up of 25 patients. Patients 18 years of age and older, classified with American Society of Anesthesiologist (ASA) stages ASA I and ASA II, and who agreed to participate in the study by signing an informed consent were included in the study. Those patients with contraindications for the practice of regional anesthesia were excluded, as well as those with a history of allergy to the drugs used. Patients who presented any surgical complication in the trans operative period that required modification of the initial anesthetic method were defined as exit criteria.
Description of the technique
With the patient in sitting, after asepsia and antisepsis of the cerico-dorsal region, the spinous process of C6-C7/C7-T1 was located, at this point and after performing the anesthetic wheal with lidocaine SP 1 0 mg, it was punctured with Tuohy needle No. 18 G by medial approach; the epidural space was located using the technique of the hanging drop and of Gutierrez, then proceeded to the placement of epidural catheter of caliber No. 22 G multiperforated, leaving 3 cm in this space, for which lidocaine SP 1% 1.5 ml with epinephrine 1: 200 000 was injected as a test dose with the aim of diagnosing a possible intravascular or subarachnoid injection. Bupivacaine 0.4 % 8 ml case anesthetic agent was administered. It was placed supine and subsequently the anesthetic sensory level was purchased. Throughout the surgical procedure, heart rate (HR), mean arterial pressure (TAM) and oxygen saturation (SpO2) were monitored using conventional non-invasive methods, in the proposed times of 30 and 60 min. All patients were administered advance analgesia with tramadol 100 mg plus diclofenac 75 mg intravenous (IV) infusion., in addition to oxygen by nasal catheter at 4 L / min and water supply with crystalloiddes during the trans operative. Before the surgical intervention, in the absence of complications, bupivacaine 0.25 % 5ml was administered by epidural catheter with the aim of maintaining postoperative analgesia. For the collection of the primary data, the medical histories of the patients were reviewed prospectively and collected in a form designed by the authors, these data included the following variables: age, sex, operative diagnosis, physical state according to the classification of the American Society of Anesthesiologists (ASA), heart rate at 30 min after the procedure, heart rate at 60 min of procedure, mean arterial pressure at 30 min of procedure, mean blood pressure 60 min after procedure, partial oxygen saturation 30 min after procedure, partial oxygen saturation 60 min after procedure, Anesthetic quality and patient satisfaction. For the processing and analysis of the information, a database was created in the statistical package SPSS version 25.0; Descriptive indicators such as absolute and relative frequencies and percentages were obtained. To determine whether the quantitative variables followed a normal distribution and to rule out the presence of aberrant values in the sample, the Shapiro-Wilk test was performed. Paired variables (before/after) that were normally distributed were subjected to the Student's T-test for related samples, while variables that were distributed differently than normal were subjected to the Wilcoxon's sign range test. Bilateral asymptotic significance values were established when p ≤ 0.05. All statistical processing was carried out with 95% reliability. For the realization of this research, the approval of the Medical Ethics and Research Committee of the Martín Chang Puga Teaching General Hospital was requested. All the information obtained was used for scientific purposes only and took into account the ethical principles set out in the Declaration of Helsinki (which have been set out in the 2013 declaration).
Results
There was a predominance of males in the sample, while most patients were between 19 and 59 years old. Only 2 patients were 60 years or older, with a mean age of 40.3 ± 13.4 years. The minimum age was 19 years and the maximum age was 65 years (Table 1).
| Age groups | Sex | Total No. (%) | |
| Female No (%) | Male No (%) | ||
| From 19 to 29 years old | 1 (14,3) | 5 (27,8) | 6 (24,0) |
| From 30 to 39 years old | 1 (14,3) | 5 (27,8) | 6 (24,0) |
| From 40 to 49 years old | 1 (14,3) | 4 (22,2) | 5 (20,0) |
| From 50 to 59 years old | 4 (57,1) | 2 (11,1) | 6 (24,0) |
| From 60 to 69 years old | 0 (0,0) | 2 (11,1) | 2 (8,0) |
| Total | 7 (100,0) | 18 (100,0) | 25 (100,0) |
| The percentages were calculated according to the total of the columns. | |||
Source: Data collection model.
Table 1: Distribution of patients according to age groups and sex.
Regarding the distribution of patients according to operative diagnosis and ASA classification, it was observed that most were classified as ASA II, with clavicle fracture and humerus fracture predominating as operative diagnosis (Table 2).
| Operative diagnosis | SO | Total No (%) | |
| I No (%) | II No (%) | ||
| Acromioclavicular fracture | 0 (0,0) | 2 (11,8) | 2 (8,0) |
| Humerus fracture | 0 (0,0) | 4 (23,5) | 4 (16,0) |
| Radius fracture | 1 (12,5) | 1 (5,9) | 2 (8,0) |
| Sternoclavicular dislocation | 0 (0,0) | 1 (5,9) | 1 (4,0) |
| Acromioclavicular dislocation | 1 (12,5) | 2 (11,8) | 3 (12,0) |
| Clavicle fracture | 6 (75,0) | 5 (29,4) | 11 (44,0) |
| Metacarpal fracture | 0 (0,0) | 2 (11,8) | 2 (8,0) |
| Total | 8 (100,0) | 17 (100,0) | 25 (100,0) |
| The percentages were calculated according to the total of the columns. | |||
Source: Data collection model.
Table 2: Distribution of patients according to operative diagnosis and classification of the American Society of Anesthesiologist s (ASA).
To determine whether the values of the vital signs followed a normal distribution, the Shapiro-Wilk test was applied, which allowed to identify that the heart rate followed a Gaussian distribution at 30 and 60 min after the start of the cervical epidural block (gl: 25; p=0.886), as well as mean blood pressure values (GL: 25; p=0.623). Partial oxygen saturation was distributed differently from normal, and the test was statistically significant (p=0.000) (Table 3).
| Variables | Shapiro-Wilk test | ||
| Statistical | Gl | p | |
| Heart rate at 30min | 0,980 | 25 | 0,886 |
| Heart rate at 60 min | 0,944 | 25 | |
| Mean blood pressure at 30 min | 0,969 | 25 | 0,623 |
| Mean blood pressure at 60 min | 0,958 | 25 | |
| Partial oxygen saturation at 30 min | 0,731 | 25 | 0,000 |
| Partial oxygen saturation at 60 min | 0,640 | 25 | |
| GL: Degrees of Freedom. | |||
Source: Statistical processing.
Table 3: Normality tests for vital signs compared to 30 and 60 min after cervical epidural block began.
Vital signs were within normal limits during the first hour of cervical epidural block. It was observed that both heart rate, mean blood pressure and partial oxygen saturation decreased significantly at 60 min of applied the anesthetic technique, compared to the values determined at 30 min (Table 4 and Fig.).
| Variables | Media | Dev. Deviation | p |
| Heart rate at 30min | 90,5 | 9,588 | 0,000a |
| Heart rate at 60 min | 78,7 | 6,134 | |
| Mean blood pressure at 30 min | 84,7 | 5,452 | 0,000a |
| Mean blood pressure at 60 min | 76,8 | 4,589 | |
| Partial oxygen saturation at 30 min | 99,4 | 0,577 | 0,001b |
| Partial oxygen saturation at 60 min | 98,8 | 0,663 | |
| a Student’s T-test for related samples. b Wilcoxon’s sign range test. | |||
Table 4: Variations in vital signs at 30 and 60 min after cervical epidural block.
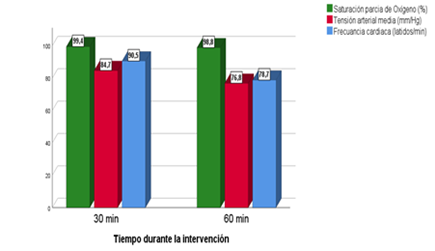
Figure: Variations in vital signs at 30 and 60 min after cervical epidural block.
Regarding the results of the technique, all patients (100%) undergoing shoulder girdle surgery with open reduction and internal fixation reported having been satisfied with the anesthetic procedure. The anesthetic quality evaluated was also good in all cases (100%).
| Anesthetic quality | Satisfaction | ||
| Good No. (%) | Suitcase No. (%) | Satisfied No. (%) | Unsatisfied No. (%) |
| 25 (100) | 0 (0) | 25 (100) | 0 (0) |
Source: Data collection model.
Table 5: Distribution of patients according to satisfaction and anesthetic quality.
Discussion
The results of this study demonstrate the effectiveness of the use of cervical epidural anesthesia in shoulder girdle surgery. There is not much evidence of the use of this technique in this type of intervention specifically, since most of the published works focus on surgery of the upper limbs, neck and epidural block at other levels of the spine. A predominance of males was observed, aged between 19 and 59 years. Apolinario [9]. in an analysis of 100 patients undergoing upper limb and shoulder girdle surgery also studied a sample in which the male sex predominated with 61 %. In this study, 57 cases were submitted to an orthopedic procedure such as open reduction and internal fixation, while the rest were submitted to vascular surgery, plastic surgery and neurosurgery. Mejía-Gómez et al [10]. in their study on the efficacy of the management of anesthetic management with cervical epidural block in upper limb trauma surgery states that this technique, although not frequently observed, can be used in thyroid, parathyroid, breast, carotid surgery and chronic pain management, highlighting that cervical epidural anesthesia for the treatment of traumas of upper limb seems to offer some advantages such as lower pulmonary complications and a low incidence of venous thrombosis and pulmonary thromboembolism, in addition to providing greater postoperative analgesia, and good hemodynamic flexibility during the trans operative. Paredes [11]. in his study on risk factors for early complications due to epidural anesthesia obtained that compared to adults undergoing surgery under general anesthesia, concomitant epidural analgesia reduces postoperative mortality and improves amultitude of cardiovascular, respiratory and testinal gastroin morbidityendpoints compared to patients receiving intravenous systemic analgesia. In this study, patients classified as ASA II predominated, and the most frequent operative diagnosis was clavicle fracture. Schoolteacher et al [12]. In a series of cases with clavicle fracture undergoing open reduction and internal fixation under analgesia by block of the pectoral nerves suggests that for this type of intervention loco-regional methods of anesthesia such as paravertebral, epidural or terminal branch blocks are more effective and safer compared to endotracheal general anesthesia. Vela-Izquierdo et al [7].identified that in upper limb and shoulder girdle surgery, postoperative analgesia by epidural catheter in continuous infusion using local anesthetics block the entry of nociceptive stimuli into the central nervous system and the addition of opioids brings a synergistic effect and a potentiation of analgesia, reducing postoperative pain, cardiovascular, pulmonary, infectious, gastrointestinal complications and the need for complementary analgesia with opioids, improving patient satisfaction. In this work it was also identified that heart rate and mean arterial pressure followed a Gaussian distribution at 30 and 60 min after the start of cervical epidural block, this means that most of the values were close to the median, while there were extreme values less frequently. The partial oxygen saturation was distributed differently from normal, but this result is not very relevant considering that the variations in this parameter were scarce, and always being within normal limits. Zettalux [13]. Reports that epidural analgesia reduces endocrine and metabolic reactions to surgical aggression. In thoracic surgery, it allows a faster exit from the resuscitation unit and, in orthopedic surgery, a decrease in the incidence of postoperative thromboembolic episodes. Loco regional anesthesia improves the patient's long-term prognosis. It also refers that the patient who has undergone locoregional anesthesia or analgesia may suffer discomfort or complications, usually benign, secondary to locoregional anesthesia, so itis important to know them, to reassure the patient and adopt standardized strategies. The vital signs of the patients who included the sample were within normal limits during the first hour of initiating cervical epidural block. It was observed that both heart rate, mean blood pressure and partial oxygen saturation decreased significantly 60 min after applying the anesthetic technique, compared to the values determine that 30 min, but always remaining within normal. In this sense, Reyes Martínez [1]. In the analysis of his series obtained that there was a significant decrease in both heart rate and mean arterial pressure in the first hour of having performed the epidural block in patients who would undergo orthopedic surgery of the humerus, coinciding with what was found by the authors of this article. However, some authors [14,15]. Recommend using a combination of endotracheal general surgery and loco-regional block in patients undergoing orthopedic surgery and neck surgery, alluding to the importance of correct pain management and prevention of complications, although this decision is poorly supported in the literature. This study also found that all patients anesthetized with cervical epidural block undergoing shoulder girdle surgery with open reduction and internal fixation reported having felt satisfied with the anesthetic procedure. This result clearly demonstrates that the levels of analgesia achieved were optimal, since patient satisfaction is directly related to the presence or absence of pain during the trans operative period.
Conclusion
Finally, it is concluded in this study that patients under cervical epidural anesthesia were mostly men, aged between 19 and 60 years. Physical status ASA II prevailed and the most frequent operative diagnosis was clavicle fracture. The hemodynamic values remained within normal limits in the first hour of the trans operative period, and all patients were satisfied with the results of analgesia achieved by this method, so it can be said that the use of cervical epidural anesthesia in shoulder girdle surgery is effective and safe.
References
- Reyes Martínez MA. (2022). Cervical epidural block for analgesia in orthopedic humerus surgery.
Publisher | Google Scholor - Salazar CRF. Genesis and evolution of lumbar epidural anesthesia in its first centenary. Rev Cubana Anestesiología y Resuscitacion, 20(3).
Publisher | Google Scholor - Cárdenas González A. (2023). Cervical epidural anesthesia, a satisfactory experience for patients and anesthesiologists. Cuban Journal of Anesthesiology and Reanimation, 12(3):192-194.
Publisher | Google Scholor - Acosta JAH, Muñoz CEM, Parreño MCC, Echeverría KEG, Jara JLM, Alejandro MRR, et al. Spinal anesthesia and its neurological complications. A literature review article. Mediciencias UTA, 6(4):9-15.
Publisher | Google Scholor - Braga A of F of A, Carvalho VH, Braga FS of S, Pereira RIC. (2023). Combined spinal epidural block for labor analgesia. Comparative study with continuous epidural block. Rev Bras Anesthesiol, 69:7-12.
Publisher | Google Scholor - Véliz IC, Rodríguez RE, Quesada SMS, Ramírez GM. (2023). Epidural anesthesia in orthopedic surgery of the lower limbs. Celia Sánchez Manduley Hospital. July- December 2019. Manzanillo. MULTIMED, 24(0).
Publisher | Google Scholor - Vela Izquierdo CE, Espinoza Aranguren VI, Constantino Ugaz JL, Aguilar Noblecilla LE, Vela Izquierdo CE, Espinoza Aranguren VI, et al. (2023). Anesthesia and cervical epidural analgesia for upper limb surgery. Journal of the Spanish Society of Pain, 26(5):304-308.
Publisher | Google Scholor - Lorda Galiano L, Navas Igarza JO, Hidalgo Herrera M, Rodríguez Fernández Y, Lorda Galiano L, Navas Igarza JO, et al. (2023). Outpatient surgical treatment in the solution of conditions of the thyroid gland. Cuban Journal of Military Medicine 51(2).
Publisher | Google Scholor - Apollinarius JM. (2023). Cervical epidural anesthesia. About 100 cases. Rev bras anesthesiol, 115-117.
Publisher | Google Scholor - Mejia-Gomez LJ. (2023). Cervical epidural block for management of upper limb trauma surgery. Rev Mex Anest,36(S1):211-215.
Publisher | Google Scholor - Walls RMA. (2023). Risk factors for early complications due to epidural anesthesia in patients treated at the Santa Rosa Hospital, Peru, during the period 2020 – 2022. Ricardo Palma University.
Publisher | Google Scholor - Schuitemaker R. JB, Sala-Blanch X, Rodriguez-Pérez CL, Mayoral R. JT, López-Pantaleon LA, Sánchez-Cohen AP. (2023). PEC II blockade as a major analgesic component for clavicle operations: description of 7 cases and literature review. Spanish Journal of Anesthesiology and Reanimation, 65(1):53-58.
Publisher | Google Scholor - Zetlaoui PJ. (2023). Locoregional anesthesia and analgesia in medical practice. EMC - Treatise on Medicine, 22(2):1-10.
Publisher | Google Scholor - Rincon Sánchez O, Escalante Elías LF, Pizaña Vázquez SA, Lucio Medina IM, Rincon Sánchez O, Escalante Elías LF, et al. (2023). Cervical epidural block for hemithyroidectomy in a patient with myasthenia Gravis. Anesthesia in Mexico, 30(3):63-67.
Publisher | Google Scholor - Rivera Díaz RC, Arcila Lotero MA. (2023).Cervical epidural infusion for treatment of herpes zoster pain. Case report with thematic review. Revista Colombiana de Anestesiología, 41(4):291-297.
Publisher | Google Scholor













