

Research Article
Effects of The Covid-19 Pandemic on Health Facilities Preparedness Against an Epidemic of SARS-COV and Cholera in The Dschang Health District
- Loic Douanla Pagning 1,3*
- Earnest Njih Tabah 2,3
- Djam Chefor Alain 3
- François Fouda 2,3
- Irine Ngani Nformi 2
- Colin Tsago Nzoyem 2,3
- Melvis Ndifor 2
- Jerome Ateudjieu 3,4,5
1GRA (Global Research Agency), Cameroon.
2National Yaws, Leprosy, Leishmaniasis and Buruli Ulcer Control Programme, Ministry of Public Health, Yaounde Cameroon.
3Department of Public Health, University of Dschang, Cameroon.
4M.A. SANTE (Meilleur accès aux soins de Santé), Yaoundé, Cameroon.
5Division of Health Operations Research, Ministry of Public Health, Cameroon.
*Corresponding Author: Loic Douanla Pagning, National Yaws, Leprosy, Leishmaniasis and Buruli Ulcer Control Programme, Ministry of Public Health, Yaounde Cameroon.
Citation: Loic D Pagning, Earnest N Tabah, Djam C Alain, Fouda F, Irine N Nformi, et al. (2023). Effects of The Covid-19 Pandemic on Health Facilities Preparedness Against an Epidemic of Sars-Cov and Cholera in The Dschang Health District, Journal of Clinical Research and Clinical Trials, BioRes Scientia publishers. 2(3):1-10. DOI: 10.59657/2837-7184.brs.23.015
Copyright: © 2023 Loic Douanla Pagning, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 24, 2023 | Accepted: August 08, 2023 | Published: August 28, 2023
Abstract
Context and Justification: Coronavirus disease 2019 (COVID-19) is an epidemic that came on abruptly and therefore affected the world in a short period. To respond effectively to this type of epidemic, healthcare facilities need to prepare properly before and during the epidemic. The level of preparedness determines the response to the problem and the effectiveness of that response.
General objective: To assess the effect of COVID-19 on healthcare facilities’ preparedness against an epidemic of cholera and SARS-CoV in the Dschang health district.
Methodology: This was an observational, cross-sectional descriptive study with an analytical component that compared the state of preparedness of healthcare facilities against an epidemic before and during COVID-19. The target was the healthcare facilities of the Dschang Health District. A questionnaire was administered face-to-face to those in charge of the healthcare facilities according to an exhaustive sampling of the healthcare facilities. Descriptive statistics were used to present data for the descriptive section. The preparedness progress was determined by comparing means and proportions of variables before and during COVID-19.
Results: A total of 72 healthcare facilities were surveyed. Of these, 31 (43.1%) had a ward for the isolation of patients and 58 (80.6%) had a focal point responsible for epidemiological surveillance. Regarding access to water, hygiene, and sanitation, 45 (62.5%) had access to an improved water source and 72 (100.0%) had at least one toilet. During the outbreak, face masks and protective suits respectively were unavailable in 40 (54.1%) and 64 (85.5%) healthcare facilities. There has been a significant improvement in hygiene. The availability of hand washing points and hand sanitizers increased significantly from 23 (31.9%) and 13 (18.1%) to 71 (98.6%) (P-value = 0.000) and 54 (75.0%) (P-value = 0.000) respectively.
Conclusion: Even though the availability of resources for epidemic preparedness remains insufficient, they have been significant improvements in the availability of hand washing points and hand sanitizers with the onset of the COVID-19 pandemic.
Keywords: effect; healthcare facilities; preparedness; epidemic; cholera; sars-cov; dschang
Introduction
An epidemic is a significant increase (above the usual threshold) in the notification of confirmed cases of a given disease, over a specific period in a clearly defined population or geographical area[1–3]. Since 1940, the frequency of epidemics and the diversity of infectious disease pathogens have increased considerably [4]. In December 2019, a cluster of atypical pneumonia cases was reported in people who had contact with the Huanan seafood market in Wuhan, China. The causative agent was quickly identified as being Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), a new member of the β -coronaviridae family [5]. At the end of January 2020, the WHO declared the epidemic a public health emergency of international concern, and on March 11, 2020, a true pandemic [6]The number of cases and deaths is inexorably increasing, endangering the living conditions of populations and significantly impacting economies[7]. On May 14, 2021, the estimated total number of cases were 162 338 294 worldwide including 3 366 436 death (Lethality rate, LR ≈ 2.07%) [8]. As of the 7th June 2023, the total cases in Cameroon were 125 036 and 1 972 deaths (LR=1,57)[9], The number of cases was 910 and 26 deaths in the Dschang health district (Dhd) as of December, 2021 (LR ≈ 2.86)(unpublished)
Meanwhile, the seventh cholera epidemic has been raging since the 1960s in the world, especially in developing countries [10]. Cholera is transmitted through the faeco-oral root and it is a public health emergency[11–14]. Cholera is a privileged companion of natural disasters and conflict situations with massive population displacements as could be seen in the North-West and South-West regions of Cameroon since 2016, where they experienced socio-political conflicts[15]. These sociopolitical conflicts which results to massive migration to neighbouring areas in Dhd. In 2018, 34 countries reported a total of 499,447 cholera cases to WHO, including 2,990 deaths (LR ≈ 0.6%)[16]. In Africa, 120,652 cases, including 2,436 deaths (LR≈2.0%) have been reported for cholera. Between 2010 and 2017, epidemiological surveillance in Cameroon recorded 37,396 cases with 1,646 deaths (LR≈ 4.4%), with the West region having 1,286 cases and 76 deaths (LR ≈ 5.9%) [16].
Most epidemics are successfully treated at the local or regional level [17]. For healthcare organizations, preparedness is considered essential to respond quickly and effectively to epidemics to minimize the spread of pathogens and reduce the number of people infected. Epidemics trigger anxiety in the general population and require rapid and adequate action from health organizations and health professionals [17, 18]. Preparedness requires an operational mindset focused on developing procedures and guidelines in all phases of preparedness, even during the period when there is no threat or epidemic [19, 20].
In this study, we aimed at assessing the effects of the COVID-19 pandemic on HF preparedness against an epidemic in the Dhd. Several studies on the preparedness of health facilities against epidemics have already been carried out but no such study has been carried out in this district. The results of this study will provide health authorities with knowledge of the shortcomings and which aspects needs to be accentuated for the preparedness of health facilities for an epidemic. To effectively carry out this work, we asked ourselves whether the advent of COVID-19 helped improve the preparedness of health facilities in the Dhd against an epidemic of cholera and SARS- CoV.
Methodology
Study Design
We carried out a cross-sectional observational study comprising a descriptive and an analytical component. Using a grid, the elements entering into the preparedness of a health facility were collected by asking questions to those in charge of the health facility, and other elements were observed by the investigator. The descriptive component consisted of collecting data on the distribution of response measures against an epidemic in the health facilities of the Dhd. The analytical component allowed us to use the data from the descriptive component to assess the effect of COVID-19 on the preparedness of health facilities in the Dhd against an epidemic.
Study Site
The study took place in health facilities of the Dhd. This health district (HD) is one of the biggest districts out of the 20 HD in the West region. It is located in the Menoua Division, and of the six Subdivisions that make up this Division, the Dhd covers four and a half. It is a cosmopolitan town comprising many ethnic groups. In this district, we have the University of Dschang which is one of the ten state universities. It also has a reference hospital, sub-divisional hospitals (SDH) and other integrated health centers (IHC).
Data Collection
Data were collected through an administered questionnaire face to face, first to the heads of the health facilities, then to the pharmacy manager in charge of the management of cholera and covid-19.
Data Management and Analysis
A database was created with Microsoft Excel 2013 software, and the data collected from the questionnaires were double-entered to minimize entry errors as much as possible.
The qualitative variables are represented by percentages. The description of quantitative variables is based on the mean and standard deviation. For comparison, tests were performed with a decision threshold of p <0>
Results
During our survey, we visited 72 health facilities located in 21 health areas. Among them, public health facilities were the most represented (35/72). In terms of type, health centers and integrated health centers accounted for 80.5%. Of all the 72 health facilities visited, we recorded no refusals; which gives us a response rate of 100%.
Availability of Resources Before and During the Pandemic
Table 1 presents the availability of human resources by category and type of HF. From this table, there was no difference in the number of health workers between the different categories of HF before and during Covid-19 (P <1>
Table 1: Comparison of the number of staff members by health facility type and category before and during COVID-19.
| HF Category | Average number of staff members before COVID-19 | Average number of staff members during COVID-19 | p-value |
| Total | 10 ± 21 | 10 ± 21 | 1.000 |
| SMC and similar | 11 ± 5 | 11 ± 5 | 1.000 |
| IHC and similar | 5 ± 2 | 5 ± 2 | 1.000 |
| DH and similar | 65 ± 58 | 65 ± 58 | 1.000 |
| HF type | Average number of staff members before COVID-19 | Average number of staff members during COVID-19 |
p-value |
| Total | 10 ± 21 | 10 ± 21 | 1.000 |
| Mission hospitals | 30 ± 37 | 30 ± 37 | 1.000 |
| Private Secular | 6 ± 4 | 6 ± 4 | 1.000 |
| Public | 9 ± 25 | 9 ± 25 | 1.000 |
HF: Health Facility, SMC: Sub divisional Medical Center, IHC: Integrated Health Center, DH: District Hospital, COVID-19: Coronavirus Disease 2019
Table 2 shows that during the pandemic there was a significant improvement in the number of beds for contagious diseases (p-value = 0.011), the number of treatment rooms (p-value = 0.014) and the number of staff trained in the management of COVID-19 (p-value = 0.000).
Table 2: Comparison of the availability of quantitative resources before and during Covid-19.
| Element | Average number before the epidemic | Average number during the epidemic | p-value |
| Average number of staff trained on ES | 1.9 ± 3.7 | 1.8 ± 3.6 | 0.408 |
| Average number of hospital wards | 5.3 ± 4.9 | 5.2 ± 5.0 | 0.413 |
| Average number of beds available in the HF | 15.9 ± 20.9 | 16.1 ± 21.7 | 0.102 |
| Average number of beds specific to contagious diseases | 0.5 ± 1.0 | 0.9 ± 1.8 | 0.011 |
| Average number of consultation rooms | 1.6 ± 2.6 | 1.6 ± 2.8 | 0.655 |
| Average number of treatment rooms | 1.2 ± 0.8 | 1.3 ± 0.8 | 0.014 |
| Average number of staff trained in cholera management | 0.5 ± 0.5 | 0.5 ± 0.5 | 0.414 |
| Average number of staff trained on COVID-19 management | 0.0 | 0.6 ± 0.5 | 0.000 |
HF: Health Facility, COVID-19: Coronavirus Disease, ES: Epidemiological surveillance
They were a significant increase from 23(31.9%) to 71(98.6%) in the availability of hand washing points before and during the Covid-19 pandemic respectively. Also, the availability of hand sanitizers in health facilities increased from 13(18.1%) to 54(75%) as seen in table 3. The availability other hygiene components such as Hygiene committee, budget for Wash did not have significant increase.
Table 3: Availability of hygiene elements before and during the Covid-19 pandemic in Health facilities.
| Situation before COVID-19 | Situation during COVID-19 | ||||||
| N | % | N | % | ||||
| Total | 72 | 100.0 | 72 | 100.0 | p-value | ||
| Availability of elements in the HF | Modalities | N | % | N | % | ||
| Hygiene committee | 29 | 40.3 | 30 | 41.7 | 0.865 | ||
| Budget for WASH | 17 | 23.6 | 18 | 25.0 | 0.846 | ||
| Maintenance Agent | 41 | 56.9 | 43 | 59.7 | 0.735 | ||
| Hand washing guide | 61 | 84.7 | 68 | 94.4 | 0.056 | ||
| Hand washing point | 23 | 31.9 | 71 | 98.6 | 0.000 | ||
| Hand sanitizer | 13 | 18.1 | 54 | 75 | 0.000 | ||
| HF cleaning program | 61 | 84.7 | 62 | 86.1 | 0.813 | ||
| Encountered difficulties in acquiring materials for WASH | 26 | 36.1 | 24 | 33.3 | 0.726 | ||
HF: Health Facility, WASH: Water, Sanitation and Hygiene, COVID-19: Coronavirus Disease 2019
Access to Water Before and During the Pandemic
The vast majority, 65(90.3%) of health facilities had a source of water. Of these, 61.1% and 62.5% were improved water sources before and during COVID-19 respectively. Almost all, 70 (97.2%) of the HF had reservoirs to store water and 25 (34.7 %) HF found the quantity of water insufficient for their activities. Drinking water was treated in three quarters (75.0 %) of HF before consumption as shown in Table 4.
Table 4: Water availability before and during the pandemic in the health facilities.
| Situation before COVID-19 | Situation during COVID-19 | ||||||
| N | % | N | % |
p-value | |||
| Total | 72 | 100.0 | 72 | 100.0 | |||
| Elements | N | % | n | % | |||
| Main water source available | 65 | 90.3 | 65 | 90.3 | 1,000 | ||
| Main Water Source improved | 44 | 61.1 | 45 | 62.5 | 0.579 | ||
| Existence of a secondary water source | 29 | 40.3 | 29 | 40.3 | 1,000 | ||
| Amount of water sufficient | 47 | 65.3 | 47 | 65.3 | 1,000 | ||
| Existence of tanks to store water | 70 | 97.2 | 70 | 97.2 | 1,000 | ||
| Water treated before drinking | 50 | 69.4 | 54 | 75 | 0.457 | ||
COVID-19: Coronavirus Disease 2019
Availability of Sanitation Items Before and During the Pandemic
All of the facilities had at least one toilet. These toilets were cleaned at a frequency of <2>
Table 5: Availability of sanitation elements before and during the pandemic in the health facilities
| Situation before COVID-19 | Situation during COVID-19 | |||||
| N | % | N | % | |||
| p-value | ||||||
| Total | 72 | 100.0 | 72 | 100.0 | ||
| Elements | Modalities | N | % | n | % | |
| Are there toilets | Yes | 72 | 100.0 | 72 | 100.0 | 1,000 |
| Types of toilets | Dry latrines | 34 | 47.3 | 34 | 47.3 | 1,000 |
| Dry latrines and WC | 14 | 19.4 | 14 | 19.4 | ||
| WC | 24 | 33.3 | 24 | 33.3 | ||
| Frequency of toilet cleaning | ˂twice a day | 56 | 77.8 | 56 | 77.8 | 1,000 |
| ≥2 times a day | 16 | 22.2 | 16 | 22.2 | ||
| Water stored in toilets | Yes | 41 | 56.9 | 41 | 56.9 | 1,000 |
| No | 31 | 43.1 | 31 | 43.1 | ||
| Presence of an incinerator | Yes | 41 | 56.9 | 40 | 55.6 | 0.867 |
| No | 31 | 43.1 | 32 | 44.4 | ||
| Sharps objects disposal means | Incineration | 53 | 73.6 | 55 | 76.4 | 0.896 |
| Landfill | 7 | 9.7 | 7 | 9.7 | ||
| Send to District | 12 | 15.3 | 10 | 12.5 | ||
| Disposal method for contaminate waste | Landfill | 38 | 52.8 | 35 | 48.6 | 0.654 |
| Throw in the pit | 26 | 36.1 | 31 | 43.1 | ||
| Incineration | 8 | 11.1 | 6 | 8.3 | ||
| Household waste disposal method | Composting | 60 | 83.3 | 65 | 90.3 | 0.218 |
| Others | 12 | 16.7 | 7 | 9.7 | ||
COVID-19: Coronavirus Disease, WC: Water Closet
Availability of Items for Epidemiological Surveillance Before and During the Pandemic
To quickly detect and treat diseases with pandemic potential, it is crucial for health facilities to implement epidemiological surveillance of these diseases. Before the Covid-19 outbreak in the Dhd, 41 (56.9%) HF had the case definition forms for cholera, and 36 (50.0 %) HF had taken the guide for the management of this disease. Notification and investigation forms were present in 35 (48.6%) and 26 (36.1%) HF respectively as shown in detail in figure 1.
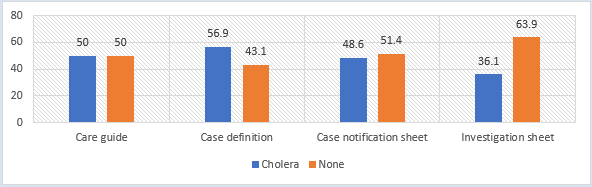
Figure 1: Availability of cholera surveillance items before the COVID-19 outbreak.
We can see in figure 2 that with the arrival of the COVID-19 pandemic, 38(52.2%) HF had obtained the guide for the management of this disease, and the case definition sheets were present in 50(68.1%) HF. On the other hand, 20(27.8%) and 33(45.8%) of HF did not have notification and investigation forms respectively.
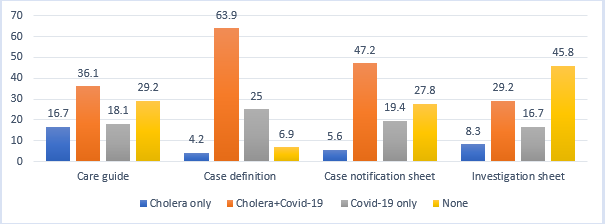
Figure 2: Availability of cholera and COVID-19 surveillance items during the COVID-19 pandemic.
Availability of Communication Tools Before and During the Pandemic
Almost all 70(97.2%) HF implemented health education for sensitization on the disease, with a predominance of 23 (31.9%) HF for interpersonal communication. More than a quarter of HF, 27(37.5%) had no communication tools before the epidemic, but this situation has been improved significantly (p-value = 0.028). Table 6 shows all the communication data in details.
Table 6: Availability of communication elements before and during the pandemic
| Situation before COVID-19 | Situation during COVID-19 | |||||
| N | % | N | % | p-value | ||
| Total | 72 | 100.0 | 72 | 100.0 | ||
| Elements | Modalities | n | % | N | % | |
| Effectiveness of communication | Yes | 71 | 98.6 | 70 | 97.2 | 0.56 |
| Mode of communication | Mass communication | 28 | 38.9 | 29 | 40.3 | 0.744 |
| Both mass& Interpersonal | 24 | 33.3 | 20 | 27.8 | ||
| Interpersonal communication | 20 | 27.8 | 23 | 31.9 | ||
| Availability of Communication tools | Yes | 45 | 62.5 | 57 | 79.2 | 0.028 |
COVID-19: Coronavirus Disease 2019
Distribution of the Availability of Care Items During the Pandemic
Regarding the elements of case management common to both epidemics, all of the HF had Ringer lactate, the infuser, the syringe and the care gloves. On the other hand, as presented in figure 3, protective suits and face masks were available in 13% and 49% of health facilities respectively.
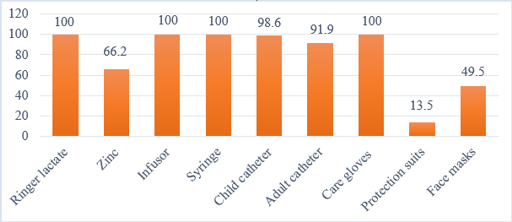
Figure 3: Availability of common management elements for cholera and COVID-19.
Figure 4 shows the availability of specific elements for the management of cholera, the oral rehydration solution was available in 48(66.2%) HF. Swabs and Doxycycline were available respectively in 62(83.8%) and 57(77.0%) health facilities.
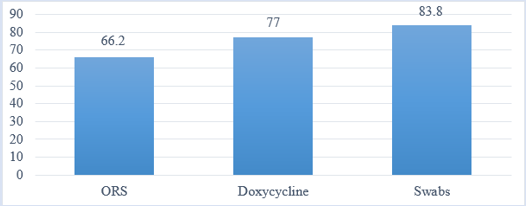
Figure 4: Availability of elements specific to the management of cholera.
ORS = Oral rehydration solution
For the management of COVID-19, 4(5.4%) health facilities had in their possession chloroquine or hydroxychloroquine. Rapid diagnostic tests and oxygen concentrators were available in 17(23.0%) and 7(9.5%) HF, respectively. The rest of the elements are visible in figure 5.
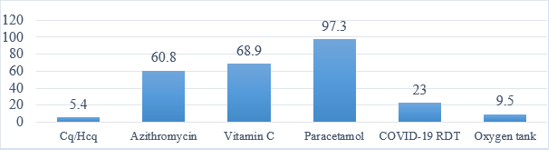
Figure 5: Coverage of the availability of case management items specific to COVID-19.
Cq / Hcq = Chloroquine / Hydroxychloroquine COVID-19 RDT = Corona virus disease Rapid Diagnostic Test
Discussion
The proportion of health facilities with at least one room for isolating patients was 43.1% during the pandemic, this proportion remains very low as in the event of a proven epidemic, rooms for isolating suspected cases of these diseases are very necessary. This is similar to a work carried out by Umar et al [21] in a study conducted in 2020 on Nigerian preparedness against Ebola and Covid-19 pandemic, where he found out that the availability of isolating rooms in 45.5% of health facilities was low. This low proportion can be explained by the fact that HF were not sufficiently prepared.
Of all the HF surveyed, 90.3% of them had at least one water source. Among these, 62.5 % of these sources were improved water sources. To compensate for the numerous interruptions of the main water source, 40.3% of the HF depended on a second source, and 97.2% of the HF had tanks to store water for use in the event of an outage. But these interruptions sometimes lasted a long time, so the quantity of water becomes insufficient for the activities of the HF, water being an important component to stop the spread of infectious diseases [22, 23]. The low availability of water in health facilities were also documented in other studies [24, 25].
The availability of hand washing stations and hand sanitizers significantly increased from 31.9% to 98.6% (p=0.000) and 18.1% to 75.0 % (p=0.000) respectively in health facilities with the occurrence of COVID-19. These improvements could be due to the joint actions of the government and the elites of the different localities as a donation to health facilities as well as sensitization through education of the community on the importance of hand washing.
They was a good availability of toilets in the surveyed health facilities, since all of them had at least one toilet. This result is almost identical to those found by Ateudjieu et al [26], where he was assessing the preparedness of HF against cholera in 4 cholera prone districts of Cameroon and Kayiwa et al [27] on their assessment of water, hygiene and sanitation services in HF in greater Kampala, Uganda, where they observed that only 4(3%) and 1(1.7%) health facilities respectively did not have toilets. This high proportion availability of toilets can be explained by the fact that they are an essential element for hygiene in a health facility [22, 23]. Of all the HFs, only 41(55.6%) had an incinerator, while 10(12.5%) sent their sharp wastes to the Health District for disposal. This transaction is dangerous, having a high risk of infection in the event of improper transport of these wastes [28, 29].
A focal point responsible for epidemiological surveillance was present in 58(80.6%) health facilities. During this period of the COVID-19 pandemic, 10(13.9%) HFs did not have the case definition sheet for this disease, and 35(47.8%) did not have the case management guide for COVID-19. The study conducted by Ateudjieu et al [26] on cholera in Cameroon also found 25(26.1%) and 53(39.6%) HF having case definition guides and case reporting forms respectively. The low availability of these surveillance items is a problem because early detection and management can control and prevent the spread of the epidemic [30-32].
For items used in the management of COVID-19, Azithromycin, vitamin C and paracetamol were present in respectively 60.8%, 68.9% and 97.3% of health facilities surveyed. These drugs, although useful in the treatment of COVID-19 and other diseases [33], were out of stock in some HF hence these proportions are not at all sufficient. The unavailability of ORS for example in some HF can lead to an alarming situation in the event of a cholera outbreak [34-36]. The availability of personal protective equipment namely: face masks and protective suits was in 45.9% and 13.5% of HF. This was similar to the results of a study conducted by Shang et al [37] on covid-19 preparedness in home health care in the United States, where he found 44.6% of the health facilities having low mask rate. The reasons for the unavailability of this equipment were mainly due to lack of funding and secondarily the materials being out of stocks [37].
Conclusion
We wanted to assess the effect of COVID-19 on the preparedness against an epidemic outbreak of health facilities in the Dschang health district. It emerges that several shortcomings were observed before the epidemic and these have not experienced significant changes with the advent of COVID-19.
These shortcomings relate in particular to the availability of resources with 56.9% of health facilities not having an isolation room for patients.
For access to water, 36.5% of HF did not have access to an improved water source. The coverage of the elements necessary for the management of patients suffering from diseases also suffers from weaknesses, in particular personal protective equipment (PPE), rapid diagnostic tests, and drugs.
Despite these shortcomings, there have been significant improvements in some aspects of preparedness of health facilities for cholera and SARS-COV epidemic, such as the availability of hand washing points, hand sanitizers, and the availability of communication tools.
Abbreviations
COVID-19: Corona virus Disease 2019, Dhd: Dschang health district, SDH: Sub divisional Hospital, HD: Health District, HF: Health facility, IHC: Integrated health center, LR: Lethality rate, SARS-CoV: Severe Acute Respiratory Syndrome Coronavirus, WaSH: Water sanitation and hygiene, WHO: World Health Organisation.
Declarations
Acknowledgments
Our gratitude goes to the following: -The parents of the corresponding author for their support during data collection for this research, all the local health authorities in the study zone including the district medical officer and chief of the bureau of health for Dschang health district and all the chief of centers for their collaborations facilitating the data collection.
Authors’ contributions
JA conceived and designed the study, and contributed to the writing of the manuscript, LDP contributed to the conception and designing of the study, collected data, analyzed data, and led the writing of the manuscript, ENT contributed to data curation, data analysis and writing of the manuscript, DCA contributed to writing the manuscript. FF contributed to the writing of the manuscript, IGN contributed to the writing of the manuscript, CTS contributed to the writing of the manuscript, JMN contributed to the writing of the manuscript. All authors have read and approved the manuscript.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
- World Health Organization (WHO) 2023.
Publisher | Google Scholor - Green MS, Swartz T, Mayshar E, Lev B, Leventhal A, Slater PE, et al. (2002). When is an epidemic an epidemic. Isr Med Assoc J, 4:3-6.
Publisher | Google Scholor - Zhang SX, Arroyo Marioli F, Gao R, Wang S. (2021). A Second Wave? What Do People Mean by COVID Waves ? – A Working Definition of Epidemic Waves. Risk Management and Healthcare Policy, 14:3775-3782.
Publisher | Google Scholor - Smith KF, Goldberg M, Rosenthal S, Carlson L, Chen J, Chen C, et al. (2014). Global rise in human infectious disease outbreaks. J R Soc Interface, 11:20140950.
Publisher | Google Scholor - Zhou P, Yang X-L, Wang X-G, Hu B, Zhang L, Zhang W, et al. (2020). A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature, 579:270-273.
Publisher | Google Scholor - Nations Unies. (2021). Journée internationale de la préparation aux épidémies.
Publisher | Google Scholor - Khetrapal S, Bhatia R. (2020). Impact of COVID-19 pandemic on health system & Sustainable Development Goal 3. Indian J Med Res, 151:395.
Publisher | Google Scholor - OMS. (2021). Coronavirus disease (COVID-19).
Publisher | Google Scholor - WHO. (2023). Coronavirus (COVID-19) Dashboard.
Publisher | Google Scholor - Pierre Aubry, Bernard-Alex Gaüzère. Choléra. 2020.
Publisher | Google Scholor - Fung IC-H. (2014). Cholera transmission dynamic models for public health practitioners. Emerging Themes in Epidemiology, 11:1.
Publisher | Google Scholor - Nelson EJ, Harris JB, Glenn Morris J, Calderwood SB, Camilli A. (2009). Cholera transmission: the host, pathogen and bacteriophage dynamic. Nat Rev Microbiol, 7:693-702.
Publisher | Google Scholor - Blake Pa, Rosenberg Ml, Costa Jb, Ferreira Ps, Guimaraes Clevy, Gangarosa Ej. (1977). Cholera in portugal, 1974 : i. Modes of transmission. American journal of epidemiology, 105:337-343.
Publisher | Google Scholor - Rabbani G, Greenough W. (1999). Food as a Vehicle of Transmission of Cholera. Journal of Diarrhoeal Diseases Research, 17:1-9.
Publisher | Google Scholor - The socio-political Crisis in the Northwest and Southwest Regions of Cameroon, Assessing the Economic and Social Impacts.
Publisher | Google Scholor - Djao R, Dunoyer J, Green K, Rossi M, Lucaccioni H. (2018). CHOLÉRA FACTSHEET CAMEROUN.
Publisher | Google Scholor - Bults M, Beaujean DJ, de Zwart O, Kok G, van Empelen P, van Steenbergen JE, et al. (2011). Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands: results of three consecutive online surveys. BMC Public Health, 11:2.
Publisher | Google Scholor - International Federation of Red Cross and Red Crescent Societies, Geneva.
Publisher | Google Scholor - Belfroid E, Timen A, Van Steenbergen JE, Huis A, Hulscher MEJL. (2017). Which recommendations are considered essential for outbreak preparedness by first responders? BMC Infectious Diseases, 17:195.
Publisher | Google Scholor - Munier A, Njanpop-Lafourcade B-M, Sauvageot D, Mhlanga RB, Heyerdahl L, Nadri J, et al. (2017). The African cholera surveillance network (Africhol) consortium meeting, 10–11 June 2015, Lomé, Togo. BMC Proceedings, 11:2.
Publisher | Google Scholor - Umar SS, Muhammad BO, Babandi ZS. (2020). Preparedness of Nigerian Health Institutions toward managing Lassa Fever Epidemic and Covid‑19 Pandemic. Niger J Med, 29(2).
Publisher | Google Scholor - Guo A, Bowling JM, Bartram J, Kayser G. (2017). Water, Sanitation, and Hygiene in Rural Health-Care Facilities: A Cross-Sectional Study in Ethiopia, Kenya, Mozambique, Rwanda, Uganda, and Zambia. Am J Trop Med Hyg, 97:1033-1042.
Publisher | Google Scholor - Huttinger A, Dreibelbis R, Kayigamba F, Ngabo F, Mfura L, Merryweather B, et al. 2017Water, sanitation and hygiene infrastructure and quality in rural healthcare facilities in Rwanda. BMC Health Serv Res, 17:517.
Publisher | Google Scholor - George CM, Jung DS, Saif-Ur-Rahman KM, Monira S, Sack DA, Rashid M, et al. (2016). Sustained Uptake of a Hospital-Based Handwashing with Soap and Water Treatment Intervention (Cholera-Hospital-Based Intervention for 7 Days [CHoBI7]): A Randomized Controlled Trial. Am J Trop Med Hyg, 94:428-436.
Publisher | Google Scholor - Nsagha DS, Atashili J, Fon PN, Tanue EA, Ayima CW, Kibu OD. (2015). Assessing the risk factors of cholera epidemic in the Buea Health District of Cameroon. BMC Public Health, 15:1128.
Publisher | Google Scholor - Ateudjieu J, Yakum MN, Goura AP, Nafack SS, Chebe AN, Azakoh JN, et al. (2019). Health facility preparedness for cholera outbreak response in four cholera-prone districts in Cameroon: a cross sectional study. BMC Health Serv Res, 19:458.
Publisher | Google Scholor - Denis Kayiwa, Mugambe K R, Mselle J, Isunju JB, Ndejjo R, Buregyeya E, et al. (2020). Assessment of water, sanitation and hygiene service availability in healthcare facilities in the greater Kampala metropolitan area, Uganda. BMC Public Health, 20:1767.
Publisher | Google Scholor - Padmanabhan KK, Barik D. (2019). Health Hazards of Medical Waste and its Disposal. Energy from Toxic Organic Waste for Heat and Power Generation, 99-118.
Publisher | Google Scholor - Diaz LF, Savage GM, Eggerth LL. (2005). Alternatives for the treatment and disposal of healthcare wastes in developing countries. Waste Manag, 25:626-637.
Publisher | Google Scholor - El-Gilany A-H. (2021). COVID-19 caseness: An epidemiologic perspective. J Infect Public Health, 14:61-65.
Publisher | Google Scholor - AlTakarli NS. (2020). China’s Response to the COVID-19 Outbreak: A Model for Epidemic Preparedness and Management. Dubai Med J, 3:44-49.
Publisher | Google Scholor - Kohler P, Renggli S, Lüthi C. (2019). WASH and gender in health care facilities: The uncharted territory. Health Care Women Int, 40:3-12.
Publisher | Google Scholor - MINSANTE/SG/DPML Cameroon - Circular letter relating to the control of the prescription of drugs used in the treatment of infection due to the new coronavirus (COVID-19).
Publisher | Google Scholor - Rakotoarisoa A, Randrianasolo L, Tempia S, Guillebaud J, Razanajatovo N, Randriamampionona L, et al. (2017). Evaluation of the influenza sentinel surveillance system in Madagascar, 2009–2014. Bull World Health Organ, 95:375-381.
Publisher | Google Scholor - Nikolay B, Salje H, Sturm-Ramirez K, Azziz-Baumgartner E, Homaira N, Ahmed M, et al. (2017). Evaluating Hospital-Based Surveillance for Outbreak Detection in Bangladesh : Analysis of Healthcare Utilization Data. PLOS Medicine, 14:1002218.
Publisher | Google Scholor - Ngwa MC, Liang S, Mbam LM, Mouhaman A, Teboh A, Brekmo K, et al. Cholera public health surveillance in the Republic of Cameroon-opportunities and challenges. Pan Afr Med J, 24.
Publisher | Google Scholor - Shang J, Chastain AM, Perera UGE, Quigley DD, Fu CJ, Dick AW, et al. (2020). COVID-19 Preparedness in US Home Health Care Agencies. JAMDA, 21:924-927.
Publisher | Google Scholor














