

Short Communication
Delaying Diagonal Gap Closure in Semi-Split Bulk Filling Technique: A Simple Innovative Modification for Considerable Reduction of Shrinkage Stress in Direct Oc clusal Composite Restorations
1Professor and Senior Consultant of Restorative Dentistry, Global Dental Centre, Vancouver, British Columbia, Canada.
2Professor and Senior Consultant of Dental Materials, Global Dental Centre, Vancouver, British Columbia, Canada.
*Corresponding Author: Khamis A. Hassan,Professor and Senior Consultant of Restorative Dentistry, Global Dental Centre, Vancouver, British Columbia, Canada.
Citation: Khamis A. Hassan. (2025). Delaying Diagonal Gap Closure in Semi-Split Bulk Filling Technique: A Simple Innovative Modification for Considerable Reduction of Shrinkage Stress in Direct Occlusal Composite Restorations. Dentistry and Oral Health Care, Biores Scientia Publishers 4(1):1-5. DOI: 10.59657/2993-0863.brs.25.042
Copyright: © 2025 Khamis A. Hassan, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 01, 2025 | Accepted: February 22, 2025 | Published: March 20, 2025
Abstract
Polymerization shrinkage continues to be a major problem in bulk-fill resin composites, which creates stress in the composite restoration and at its interface with tooth structure. The clinical manifestations of this stress, include marginal failure and subsequent secondary caries, marginal staining, restoration displacement, tooth fracture, and/or post-operative sensitivity. This paper proposes a modification of the semi-split bulk filling technique, which involves delaying the diagonal gap closure for 5 minutes following the first light curing for achieving a considerably higher reduction in unrestrained lateral shrinkage stress.
Keywords: bulk composite; delayed closure; diagonal gap; direct restoration; innovative; modified, occlusal; segment; semi-split; shrinkage stress, unrestrained
Introduction
The demand on bulk-fill resin composite restorations have increased dramatically in the past few years because of their improved esthetic qualities, mechanical properties, and ease of placement [1,2]. However, these materials possess the undesirable, inherent property of shrinkage upon light curing. During which, polymerization shrinkage occurs and generates stress. Shrinkage stress is defined as the pressure that builds up in tooth structure and adhesive during polymerization. It is a complex phenomenon, and depends on several factors, among which are the boundary conditions, amount of material, the polymerization reaction. They all play essential role in stress development and/or transmission to tooth structure [3,4].The magnitude of shrinkage stress is influenced by the following several factors: the composition and viscosity of composites, the elastic modulus, and the configuration factor (C-factor) where a higher C-factor means higher stress levels placed on the bonded surfaces during the polymerization process, as well as the composite placement technique, and the restoration volume, where restorations with larger diameters and depths can result in higher shrinkage stress [5-9]. Post-curing polymerization is the process by which composite resins continue to polymerize for up to 24 hours after initial light exposure. [10] During the five-minute period after light exposure, the generated shrinkage stress can increase significantly in the polymerizing composite [11]. The significantly increased shrinkage stress occurs because the polymerizing composite is restrained due to bonding to the surrounding cavity walls, resulting in its prevention from displacement [12-14]. This significantly increased stress results in the development of high strain, which leads to marginal gap formation, cuspal deflection, and enamel micro-cracking [12,13]. Using the bulk filling technique, a bulk-fill resin composite is placed in a large occlusal cavity using a single mass of 4-5 mm thickness. Upon light curing of the composite mass in occlusal cavity preparation, it hardens and undergoes restrained shrinkage due to bonding to the surrounding cavity walls. The polymerizing composite struggles to get smaller and take up less space, that results in developing a significant increase in stress (during the five minutes after light exposure). This stress puts pressure on the adhesive and surrounding tooth structure, causing several undesired clinical consequences in the final restoration/restored tooth [15]. Large occlusal bulk-fill resin composite restorations are placed using the bulk filling technique. Upon light curing of the 4 mm thick single mass of composite in the prepared cavity, it hardens and undergoes restrained shrinkage due to bonding to the surrounding cavity walls. During the five-minute period after light exposure, the polymerizing composite struggles to get smaller and take up less space, which results in developing a significant increase in stress. This stress puts pressure on the adhesive and surrounding tooth structure, causing several undesired clinical consequences in the final restoration/restored tooth, such as debonding that results in internal or marginal gaps, enamel cracks, and cuspal deflection, as well as microleakage, secondary caries, and postoperative sensitivity [16,17]. As the shrinkage stress was observed to significantly increase during the 5-minute period after light exposure [11], delaying the closure of the diagonal gap for a similar period, instead of closing it immediately as in the original semi-split bulk filling technique, is considered sufficient for increasing the gap’s effectiveness to greatly reduce the shrinkage stress and to counterbalance the significant stress increase.The objective of this paper is to propose a modification of the semi-split bulk filling technique, which involves leaving the diagonal gap open (unfilled) for 5 minutes after the first light exposure, instead of closing it immediately, for achieving a considerably higher reduction in shrinkage stress.
Discussion
The (original) semi-split bulk filling technique
The shrinkage stress generated in the bulk-fill resin composite exerts tension on the bonding adhesive and the surrounding tooth structure during the polymerization process. As polymerization proceeds, the generated shrinkage stress increases. When the shrinkage stress exceeds the bond strength, a marginal gap is formed. This formation of the gap is extensive if the shrinkage stress becomes greater than the bond strength early in the polymerization process. Whereas the gap formation is limited, if the shrinkage stress becomes greater than the bond strength late in the polymerization process [18]. The original semi-split bulk filling technique can mitigate the restrained shrinkage and its deleterious effects that occur when used for placing direct placement of large posterior bulk-fill resin composite restorations. This technique was introduced in 2021 for direct restoration of large occlusal cavities with bulk-fill resin composites. It involves creation of a diagonal gap in the top half of composite mass, in advance of light exposure. The diagonal gap constitutes an integral part of the (original) semi-split bulk filling technique. The gap (1.5 mm wide and 2 mm deep) is created diagonally in the top half of the uncured composite mass using a Teflon-coated plastic filling instrument in a push stroke [19,20-23]. The created gap divides the top half of the composite mass into two separated segments, where each segment is bonded to the adjacent cavity wall only. The segmented composite is then light cured for the first time [20-23]. Following that, the segmented composite is light cured for the first time. Upon polymerization, each composite segment undergoes unrestrained shrinkage due to bonding to the adjacent cavity wall only. The unrestrained shrinkage allows development of unrestrained stress and free displacement. The free displacement starts at the diagonal gap center and proceeds in an outward direction, towards the adjacent bonded cavity wall. This results in higher volume reduction of each segment, along with increased width of the diagonal gap. Immediately following the first curing, the restoration is completed by filling the diagonal gap with the same composite, and light curing it for the second time. This technique reduces debonding and gap formation at deep pulpal floors of occlusal cavities, resulting in restorations with reduced postoperative pain and sensitivity [19].
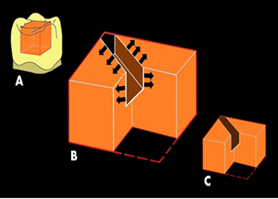
Figure 1: The original semi-split bulk fill technique, outlining the free unrestrained lateral shrinkage displacement immediately following the first light curing.
Figure 1 The original semi-split bulk filling technique, outlining the free unrestrained lateral shrinkage displacement immediately following the first light curing. (A) Single mass of bulk-fill resin composite placed directly in large occlusal cavity. (B) Composite mass with cutout corner, showing the diagonal gap created in the top half of the un-cured composite mass, which is followed by light curing for the first time. The number and direction of black arrows in each polymerizing segment represent the magnitude and direction of the free unrestrained lateral displacement. (C) Diagonal gap immediately closed with the same composite and light-cured for the second time.
The modified semi-split bulk filling technique
The modified technique is basically the same as the original semi-split bulk filling technique, with the exception that the closure of the diagonal gap is delayed for a period of 5 minutes after the first light exposure.
The rationale for the proposed modification is that delaying the diagonal gap closure for 5 minutes, following the first light curing, could allow each polymerizing composite segment the adequate time to independently undergo considerably high unrestrained lateral shrinkage, accompanied with lower stress and free displacement. The free shrinkage displacement occurs in an outward direction from the gap center and proceeds towards the adjacent bonded cavity wall, resulting in considerably higher relief of the shrinkage stress in the final composite restoration. This results in preserving the marginal integrity of the final restoration, and greatly reduce marginal gap formation, cuspal deflection, and enamel micro-cracking.
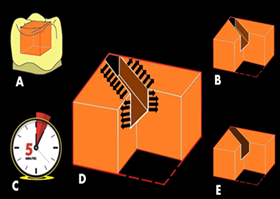
Figure 2: The modified semi-split bulk filling technique, outlining the free unrestrained lateral shrinkage displacement after waiting for 5 minutes, following the first light curing.
Figure 2 The modified semi-split bulk filling technique, outlining the considerably increased unrestrained lateral shrinkage displacement after waiting for 5 minutes, following the first light curing. (A) Single mass of bulk-fill resin composite placed directly in large occlusal cavity. (B) Composite mass with cutout corner, showing the diagonal gap created in the top half of the un-cured composite mass, which is followed by light curing for the first time. (C) Gap closure delayed for 5 minutes, after the first curing. (D) The increased number of black arrows and direction in each polymerizing segment represent the magnitude and direction of the considerably increased unrestrained lateral shrinkage displacement, resulting in greatly increased stress reduction. (E) Diagonal gap closed with the same composite and light-cured for the second time.
In the original semi-split bulk filling technique, where the gap is closed immediately following the first light exposure, the diagonal gap results in reduction of the shrinkage stress. This agrees with the findings of a research study that compared microleakage in large occlusal bulk-fill resin composite restorations placed using two insertion techniques, where the marginal microleakage and microleakage on the pulpal floor were effectively reduced, as compared to the conventional bulk filling technique [24]. In contrast to the original semi-split bulk filling technique where the gap’ effectiveness is not fully utilized, in the modified technique, the modified semi-split bulk filling technique is anticipated to substantially increase the gap’s effectiveness by delaying the closure of diagonal gap for 5 minutes after the first curing. This delay is expected to considerably relieve the shrinkage stress, resulting in better adaptation to cavity walls and margins, and considerable reduction of marginal gap formation, cuspal deflection, and enamel micro-cracking.
Conclusion
The proposed modification of the semi-split bulk filling technique is simple and beneficial. It involves delaying of the diagonal gap closure for 5 minutes, following the first light exposure. This modification would considerably reduce the shrinkage stress, leading to a final restoration with greatly reduced marginal gaps, cuspal deflection and enamel micro-cracking.
References
- Taubock TT, Jager F, Attin T. (2019). Polymerization shrinkage and shrinkage force kinetics of high- and low-viscosity dimethacrylate and ormocer based bulk-fill resin composites. Odontology,107:103-110.
Publisher | Google Scholor - Goncalves F, Campos LM, Rodrigues-Junior EC, Costa FV, Marques PA, Francci C, Braga RR, Boaro LC. (2018). A comparative study of bulk-fill composites: degree of conversion, post-gel shrinkage and cytotoxicity. Braz Oral Res, 32:e17-e26.
Publisher | Google Scholor - Stansbury JW, Trujillo-Lemon M, Lu H, Ding X, Lin Y, Junhao G. (2005). Conversion-dependent shrinkage stress and strain in dental resins and composites. Dent Mater, 21:56-67.
Publisher | Google Scholor - Watts DC. (2005). Reaction kinetics and mechanics in photo-polymerised networks. Dent Mater, 21:27-35.
Publisher | Google Scholor - Manhart J, Chen HY, Hickel R. (2010). Clinical evaluation of the posterior composite Quixfil in class I and II cavities: 4-year follow-up of a randomized controlled trial. J Adhes Dent, 12:237-43.
Publisher | Google Scholor - Al Sunbul H, Silikas N, Watts DC. (2016). Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composites. Dent Mater, 32:998-1006.
Publisher | Google Scholor - Schneider LF, Cavalcante LM, Silikas N. (2010). Shrinkage Stresses Generated during Resin-Composite Applications: A Review. J Dent Biomech, 1-14.
Publisher | Google Scholor - Oliveira KMC, Lancellotti ACRA, Ccahuana-Vásquez RA, Consani S. (2013). Influence of filling techniques on shrinkage stress in dental composite restorations. J Dent Sci, 8:53-60.
Publisher | Google Scholor - Kaisarly D, El Gezawi M, Keßler A, Rösch P, Kunzelmann KH. (2017). Shrinkage vectors in flowable bulk-fill and conventional composites: bulk versus incremental application. Clin Oral Investig, 25:1127-1139.
Publisher | Google Scholor - Kaviani A, Goudarzi P. (2022). Effect of Shade on Immediate and Post-Curing Polymerization Shrinkage of Composite Resin. J Iran Dent Assoc, 34:27-35.
Publisher | Google Scholor - Cunha, LG, Alonso RCB, de Souza Junior, EJC, Neves ACE, Sobrinho LC, Sinhoreti MAC. (2008). Influence of the curing method on the post-polymerization shrinkage stress of a composite resin. J Appl Oral Sci, 16:266-270.
Publisher | Google Scholor - Goncalves F, Campos LM, Rodrigues-Junior EC, Costa FV, Marques PA, Francci C, Braga RR, Boaro LC. (2018). A comparative study of bulk-fill composites: degree of conversion, post-gel shrinkage and cytotoxicity. Braz Oral Res, 32:e17-e26.
Publisher | Google Scholor - Menees TS, Lin CP, Kojic DD, Burgess JO, Lawson NC. (2015). Depth of cure of bulk fill composites with mono wave and poly wave curing lights. Am J Dent, 28:357-61.
Publisher | Google Scholor - Monteiro R V, Taguchi C M C, Gondo R, Monteiro-Junior S. (2019). Bulk-fill composite restorations step-by-step description of clinical restorative techniques case reports. Odovtos Int J Dent Sci, 21:23-31.
Publisher | Google Scholor - Soares CJ, Faria-E-Silva AL, Rodrigues MP, Vilela ABF, Pfeifer CS, Tantbirojn D, Versluis A. (2017). Polymerization shrinkage stress of composite resins and resin cements – What do we need to know?. Braz Oral Res, 31:e62.
Publisher | Google Scholor - Alomari, Q. D., Barrieshi-Nusair, K. & Ali, M. (2011). Effect of C-factor and LED Curing Mode on Microleakage of Class V Resin Composite Restorations. European J Dent, 5:400-8.
Publisher | Google Scholor - Malhotra, N., M, K. & Acharya, S. (2010). Strategies to Overcome Polymerization Shrinkage − Materials and Techniques. A Review. Dent Update, :115-125.
Publisher | Google Scholor - Irie M, Tanaka J, Maruo Y, Nishigawa G. (2014). Vertical and horizontal polymerization shrinkage in composite restorations. Dent Mater, 30:e189-e198
Publisher | Google Scholor - Hassan KA, Khier SE. (2021). Semi-split bulk filling technique in large occlusal bulk-fill resin composite restorations. J Oral Med and Dent Res, 2:1-9.
Publisher | Google Scholor - Hassan KA, Khier SE. (2021). Semi-split bulk filling technique: a key to achieve occlusal bulk-fill resin composite restorations free of postoperative sensitivity and pain. J Clin Res Dent, 4:1-3.
Publisher | Google Scholor - Hassan KA, Khier SE. (2023). Direct bulk-fill resin composite restorations: characterization of pulpal floor gaps in deep occlusal cavities and current restorative minimization strategies - An overview. Saudi J Oral Sciences, 10:59-65.
Publisher | Google Scholor - Hassan KA, Khier SE. (2023). Gap-Modified Bulk Placement Technique for Reducing Shrinkage Stresses in Direct Occlusal Bulk Fill Resin Composite Restorations. J Oral Dent Health Res, 5:162-166.
Publisher | Google Scholor - Hassan, K A.; Khier, S E. (2023). Direct bulk-fill resin composite restorations: Characterization of pulpal floor gaps in deep occlusal cavities and current restorative minimization strategies — An overview. Saudi J Oral Sci,10:59-65.
Publisher | Google Scholor - Patel D, Khunt A, Somani M, Kinariwala N, Joshi C, Patel A. (2022). Comparative evaluation of microleakage between novel semi-split and bulk filling technique using two different generations of the adhesive system: an in vitro study. Neuro Quant ology, 20:1480-1489.
Publisher | Google Scholor












