

Research Article
Darier's Disease: Case Report
- Melba González Lastre 1
- Jojansy Rojo González 2
- Isis Esther Martin Alonso 1
- Elsa Rodríguez Herrera 3
- Eric Fuentes Rodríguez 4
- Frank Díaz López 5
- Daysi Pérez Sánchez 5
- Claribel Plain Pazos 5
1 Department of Comprehensive General Medicine, Faculty of Medical Sciences of Sagua la Grande, Villa Clara, Cuba.
2 Department of Comprehensive General Medicine, “Mario Antonio Pérez” Polyclinic, Sagua la Grande, Villa Clara, Cuba.
3 Department of Comprehensive General Medicine, Faculty of Medical Sciences of Sagua la Grande, Villa Clara, Cuba.
4 Department of Medicine, Faculty of Medical Sciences of Sagua la Grande, Villa Clara, Cuba.
5 Department of Comprehensive General Medicine, “Mártires del 11 de Abril” Polyclinic, Corralillo, Villa Clara, Cuba.
*Corresponding Author: Claribel Plain Pazos, Department of Comprehensive General Medicine, “Mártires del 11 de Abril” Polyclinic, Corralillo, Villa Clara, Cuba.
Citation: Melba G Lastre, Jojansy R González, IEM Alonso, Elsa R Herrera, Claribel P Pazos, et al. (2023). Darier's disease: Case report, Journal of Clinical Research and Clinical Trials, BRS publishers. 2(2); DOI: 10.59657/2837-7184.brs.23.009
Copyright: © 2023 Claribel Plain Pazos, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 11, 2023 | Accepted: April 07, 2023 | Published: April 14, 2023
Abstract
Darier’s disease, or Darier-withe disease, also known as follicular dyskeratosis is an acantholytic and dyskeratotic Geno dermatosis. associated with intrinsic lesions of the inter keratinocyte adhesion systems; Usually begins between the first and second decade of life not affecting seborrheic areas with keratotic papule, very pruritic. There is no curative treatment. The psychosocial consequences caused by the appearance of the lesions and their chronic condition constitute the greatest concern. A 58-year-old female patient with a diagnosis of Darier’s disease based on clinical and family history is presented.
Keywords: darier-white’s disease; follicular dyskeratosis; genodermatosis
Introduction
Darier's disease is also known by the names of Darier-White disease, follicular dyskeratosis, or follicular keratosis. It is an acantholytic and dyskeratotic Geno dermatosis associated with intrinsic lesions of the interkeratinocytic adhesion systems. It usually begins in childhood and adolescence, affecting seborrheic areas with very itchy keratosic papules. In addition to the classic form, there are several variants, including the localized type, also called linear, unilateral, segmental, zosteriform, or blaschkoid, which is much rarer. It occurs in all ethnic groups, with equal involvement in both sexes. Its prevalence is estimated to be between 1/50,000 and 1/100,000 inhabitants, and it generally begins before the third decade of life with a peak at puberty between 6 and 20 years of age [2]. Its diagnosis is clinical and histopathological. There is no curative treatment. Systemic retinoids are the treatment of choice. The psychosocial consequences caused by the appearance of the lesions and their chronic condition are the greatest concern [3]. Although it is a rare disease, it is interesting for the primary care physician to know its existence and the main clinical forms of manifestation in order to make a proper diagnosis. We present a case seen in our health area.
Presentation of the case
A 58-year-old female, from a rural environment, with a history of Darier's disease. Family medical history: mother, six siblings, only daughter, and granddaughter with a diagnosis of Darier's disease, with onset in childhood in all of them. The diagnosis was made in this patient based on the symptoms and her family history; no histological examination was performed. The initial symptoms began at 8 years of age, characterized by the appearance of small eruptions in the form of hyperkeratotic papules and intense itching all over the body, predominantly on the lower extremities. The clinical picture intensifies approximately 35 years ago, with extension of the lesions to other body areas, with areas of inflammation and desquamation. The patient refers to not performing regular treatment for the lesions, or general care for adequate sun protection of the skin. Current condition: patient who came to present a worsening of the lesions with intense itching, bleeding in them and signs of scratching. On physical examination we found generalized dermatosis affecting the head, trunk, and extremities; predominantly in the auricular region, forearms, hands, legs and feet, made up of brownish erythematous papules and hyperkeratotic plaques, with crusty myeliseric lesions that extend to the subcutaneous cellular tissue, with traces of secondary bleeding, scratching, accompanied by stench (Figures 1 and 2).
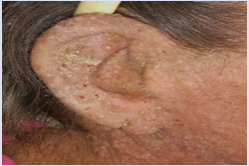
Figure 1: Symmetrical dermatosis affecting the head (including the earlobe), made up of erythematous papules and hyperkeratosis plaques, with crusty myeliseric lesions on the pinna.

Figure 2: Symmetrical dermatosis affecting the extremities, consisting of erythematous-brown hyperkeratotic plaques, with crusty myeliseric lesions, which extend to the subcutaneous cellular tissue, with traces of bleeding secondary to scratching and desquamation.
Nail condition characterized by onychorrhexis (grooved nail), associated with onychoschizia (V-notch of the free edge of the nail) and alternating red and white longitudinal bands running from the lunula to the free edge. This “sandwich” appearance is pathognomonic of the naildisease (figure 3). In addition to signs of bacterial superinfection in the regions of the groin, armpits and feet. Nail condition characterized by onychorrhexis associated with onychoschicia (V-notch of the free edge of the nail), subungual hyperkeratosis, and alternating red and white longitudinal bands running from the lunula to the free edge.

Figure 3: Nail condition characterized by onychorrhexis associated with onychoschizia.
In complementary tests performed, he presented leukocytosis with a predominance of neutrophils and mild anemia. In this new episode, he was prescribed a double antimicrobial scheme based on cephalosporins and sulfas for 7 days due to superinfection of the lesions, an antihistamine for pruritus, the local application of neomycin ointment combined with topical corticosteroids, in addition to avoiding exacerbating factors, such assun, heat or stress, trying to keep the skin cool and reducing perspiration (light cotton clothing, sunscreen) clinical improvement of symptoms such as pruritus and superinfection of lesions was observed.
Discussion
Darier's disease (DD) was first described in 1886 by Morrow, and later independently by Ferdinand Jean Darier and White. It is an autosomal dominant Geno dermatosis (disease of genetic origin, whose phenotypic expression in the skin constitutes its main clinical or diagnostic manifestation) with complete penetrance and variable expressivity [1]. A mutation in the ATP2A2 gene (12q23-q24.1) has been identified.) encoding an endoplasmic reticulum Ca2+ pump [2,4]. This mutation alters intracellular calcium signaling leading to dyskeratosis and acantholysis, fundamental but not exclusive histological findings of ED. Currently, more than 130 gene mutations have been described, it has been shown that the existence of the same mutation in this gene gives rise to different clinical expressions, with variable severity, so there must be other factors, whether genomic or environmental, that affect the expression of the disease [4].
Despite the fact that it is a hereditary disease, 47% of the patients do not have a family history of it. The presentation between siblings is not frequent, as is the case of the patient studied [5,6]. Other authors refer to up to 68% of sporadic cases or due to nov 3 mutations.
Clinically, it is characterized by presenting keratotic popular lesions in isolated seborrheic areas or in the form of crusty plaques, brown or yellowish-brown in color symmetrically [7], which sometimes become superinfected and cause bad odor. They tend to worsen with heat, sweating, friction, sun exposure or artificial ultraviolet rays. The main location is in the seborrheic areas of the trunk (chest, back) and head (scalp, neck, ears). Other areas that can be affected are the anogenital region, groin, armpits, hands and feet (small depressions or marked keratosis suggestive of the disease can be seen on the palms and soles, and less frequently hemorrhagic macules). Small whitish papules may appear on the oral mucosa, hard palate, esophagus, vulva, and rectum. The nails (mainly of the hands) are usually affected: they are more fragile and have a «V» shape and white and red bands can be seen in the longitudinal direction and subungual hyperkeratosis. Nail lesions usually facilitate the diagnosis of the disease [3], as was observed in the patient studied. Less commonly, it affects the scalp, the antecubital and popliteal fossae, and the trunk. Itching is usually present, a bad odor if they are superinfected (they are more prone to pyogenic and herpes simplex infections) and in fewer cases pain [6,8].
There are a large number of clinical forms described, the following being found in order of frequency: disseminated popularized, pustulobullous, unilateral, zoniform, hypertrophic, localized, acral, and hemorrhagic [7]. Generalized forms present in 90% of cases and only 10% the presentation is localized or linear [9].
Darier's disease is frequently associated with disorders, especially those of an affective type such as bipolar disorder, schizophrenia, psychosis, and suicidal tendencies; other associated diseases are rare, epilepsy, mental retardation, encephalopathy and brain atrophy predominate. Other authors point out the association with circumscribed plantar keratoderma, multiple epidermal cysts, filiform palmoplantar hyperkeratosis, dermatofibroma protuberans, multiple warts, cutis verticisgyrata, dimorphic leprosy, and gynecomastia [10]. Although it does not constitute a disease that predisposes to malignant tumors, its association with basal cell carcinoma has been described. Dolci et al., in 2004, published the first case of Darier-White disease and squamous cell carcinoma, both in the oral mucosa [1,8,9].
The positive diagnosis of the disease is based on the suspicion before a picture clinically reminiscent, it is almost always confirmed by a fairly typical but non-specific histological image, due to abnormal, early and individual keratinization of the cells of the epidermis [5]. In the case of the patient studied, it was performed due to the clinical manifestations and family pathological history.
The histological differential diagnosis should be considered with other Geno dermatoses and dermatoses that present a suprabasal cleft with acantholysis and with those that show the lesser tissue reaction pattern acantholytic dyskeratosis [9]. The clinical differential diagnosis should be made with: verruciform acro keratosis, epidermal nevus, verrucous dyskeratoma, Hailey-Hailey disease, Grover's acanthotic dermatosis, and dyskeratotic comedones.
ED usually follows a chronic course with exacerbations and remissions. One third of the patients reported improvement with age, another third suffered worsening of the lesions and the remaining third showed no changes. In general, worsening occurs in excessively hot climates, as is the case in our country, sun exposure, in our case the patient did not apply adequate skin protection, drugs such as lithium and steroids, menstrual period, and pregnancy. Spontaneous remissions are sometimes observed. The response to the different treatments is variable [4,10].
The approach is symptomatic, since there is no known curative treatment, avoiding the triggering factors and oral retinoids are the bases of treatment, improving the appearance of the skin, symptoms and infectious complications. If there is bacterial or fungal superinfection, topical antibiotics or antifungals can be used. If the skin infection is extensive or does not respond to topical treatment, systemic treatment may be needed [4]. The case presented evolved satisfactorily with local and systemic treatment based on antibiotics.
Conclusion
Darier's disease is a rare disease with a low incidence. It has no curative treatment. The psychosocial consequences caused by the appearance of the lesions and their chronic condition are the greatest concern of patients with this disease, so as primary care physicians it is important to consider it within our differential diagnoses and identify it in a timely manner.
References
- García Arpa M, Flores Terry MA, Villasanti Rivas N, de la Cruz Gómez E, Ramos Rodríguez C. (2017). Enfermedad de Darier lineal en 5 pacientes. Piel, 32(9):535-539.
Publisher | Google Scholor - Castano M.B, Litvack D, Consigli J, Manrique VDL, Pereyra S. (2016). Enfermedad de Darier. Presentación en dos hermanos. Arch. Argent. Dermatol. 66(6):182-186.
Publisher | Google Scholor - Olivares L. (2009). Enfermedad de Darier-White clásica y lineal. Rev. argent. Dermatol, 90(6):21-24.
Publisher | Google Scholor - Valois A, Girault PY, Morand JJ. (2016). Enfermedad de Darier. Reporte de un caso. EMC-Dermatología, 50(2):1-10.
Publisher | Google Scholor - Pérez Martín DA, Agüeros Fernández MJ, Avellaneda Fernández A, López Lanza JR, Izquierdo Martínezdy M, Peña Irún A. Enfermedad de Darier. Rev Espmed genyfam, 5(3):113-115.
Publisher | Google Scholor - Blasco Morente G, Garrido Colmenero C, Pérez López I, Martínez López A, Ruiz Villaverde R. (2015). Enfermedad de Darier segmentaria tipo 1: una enfermedad infrecuente. Dermatol Rev Mex, 59:592-594.
Publisher | Google Scholor - Di Martino B, Giardina R, Flores De Lacarrubba L. (2010). Enfermedad de Darier-White (queratosis folicular). Descripción de un caso y revisión de los diagnósticos diferenciales. Rev Esp Patol, 43(3):176-179.
Publisher | Google Scholor - González Escudero M, Betancourt Pérez A, Peraza Cruz D. (2014). Informe de caso. Enfermedad de Darier-White de la vulva. Presentación de una paciente. Rev Acta Médica del Centro, 8(2):81-84.
Publisher | Google Scholor - Castillo Tapia AN, Silva JA. (2018). Enfermedad de Darier. Reporte de un caso. Rev Mex Pediatr, 85(1):21-24.
Publisher | Google Scholor












