

Case Report
Cutaneous Melanoma with Nras Mutation from A Giant Congenital Melanocytic Nevus
1 Medical specialist Genetics Clinic of the “Luis G Dávila” General Provincial Hospital, Tulcán-Ecuador.
2 General physician at the “Luis G Dávila” General Provincial Hospital, Tulcán-Ecuador Neonatology Service.
3 Dermatology specialist at the “Luis G Dávila” General Provincial Hospital, Tulcán-Ecuador Dermatology Service.
*Corresponding Author: Víctor Hugo Guapi Nauñay, Medical specialist Genetics Clinic of the “Luis G Dávila” General Provincial Hospital, Tulcán-Ecuador.
Citation: V.H.G. Naunay, A.J.S. Guijarro, E.A.V. Duran. (2024). Cutaneous Melanoma with Nras Mutation from A Giant Congenital Melanocytic Nevus, Journal of Clinical Research and Clinical Trials, BioRes Scientia publishers. 3(1):1-6. DOI: 10.59657/2837-7184.brs.24.025
Copyright: © 2024 Víctor Hugo Guapi Naunay, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 08, 2024 | Accepted: February 21, 2024 | Published: March 07, 2024
Abstract
Melanoma is a rare tumor in childhood and represents 0.9% of pediatric neoplasms. Giant congenital melanocytic nevus has an estimated incidence of 1 in every 20,000 births worldwide, with mutations occurring after zygote formation in the NRAS gene in 80% of cases. Cutaneous melanoma is a rare condition at birth that could go unnoticed due to lack of knowledge of its presence in inexperienced hands.
Aim: Correlate the development of cutaneous melanoma from a giant congenital melanocytic nevus.
Clinical Case: Newborn who was evaluated at 10 days of age, in whom a macular lesion was observed, with well-defined irregular edges, of non-uniform color, with dark brown and black tones, partially covered with fine, dark hair, with an approximate diameter of 23 .5 cm long x 7.5 cm that covers part of the thoracolumbar region up to the anterior limit, between the mesogastrium and the right flank, respecting the inguinal area. Within this macular lesion, an irregularly shaped nodule (1.5 x 2 cm) was evident, without ulceration, pink in color with traces of dark brown, located in the left thoracolumbar region. The histopathological study described an epithelioid nodule, in the vertical growth phase, at level III according to Clark's microstratification and with a thickness of 1.3 mm according to Breslow. Molecular analysis of the NRAS gene from genomic DNA revealed a p.Q61K mutation in a homozygous state in exon 61.
Conclusion: The patient with cutaneous melanoma from the giant congenital melanocytic nevus constitutes a case of interest because it is a rare clinical entity in the neonatal age, since showing various shades of color in the macular lesion is highly suggestive of malignancy.
Keywords: melanoma; pigmented nevus; infant, genetics; neural crest
Introduction
Melanoma is a rare tumor in childhood and represents 0.9% of pediatric neoplasms. Congenital melanocytic nevus (Congenital Melanocytic Nevi, CMN) is clinically defined as a dermatological lesion present at birth, or capable of developing during childhood from a pre-existing melanocytic injury [1]. Only 5% of diagnosed cases present multiple nevi, which are located mainly on the trunk and the proximal portion of the extremities, the scalp and neck [2]. It is usual for the CMN to be classified by its size [3].The giant congenital melanocytic nevus (Giant Congenital Melanocytic Nevus, GCMN) OMIM# 137550, reaches a diameter projection greater than 20 cm in the adult [4].The estimated incidence is 1 in every 20,000 births worldwide [5]. and in South America it is 1 for every 20,455 live births [6].The risk of developing melanoma is directly proportional to the size of the nevus, between 2.6 and 4.9% for small and medium-sized nevus, respectively, and 6 to 20% for giant nevus [7]. Mutations that occur after the formation of the zygote in the NRAS gene are the cause of CMN formation in 80% of cases, since the same mutation has been found in different skin lesions in the same individual and in neurological tissue. Other mutations located in the BRAF, TP53 and GNAQ gene loci have been shown to be involved. Variants in the melanocortin-1 receptor (MC1R) correlate nevus size and red hair color in patients with CMN [8].
Patients with CMN present characteristic facial features since the multipotent cells of the ectoderm are affected, from which melanocytes and osteocytes are derived for the development of facial bones and cartilage. Melanoblasts come from migrating neural crest cells [9], Proliferation and differentiation is regulated by complex gene interactions that control the MAP-Ras (mitogen activated protein kinase, MAPK) kinase cascade [10,11]. The treatment of GCMN has been and still is the cause of strong controversy. There are two possible approaches: surgical and conservative [12]. By conservative attitude we mean not only periodic monitoring by the doctor, since it also involves self-monitoring by the patient's parents. The final decision must be the result of an individualized assessment, considering the size, location, risks derived from a surgical intervention, the risk-benefit ratio and the patient's life expectations. Cutaneous melanoma is a rare condition at birth that could go unnoticed due to lack of knowledge of its presence in inexperienced hands. The objective of the present investigation was to correlate the development of cutaneous melanoma from a giant congenital melanocytic nevus in a ten-day-old patient.
Clinical Case
A newborn who was 10 days old was consulted at the genetics service, with the history, mother was 35 years old and father was 43 years old, not consanguineous, with no family history of melanoma or any other type of neoplasia. The pregnancy recorded seven prenatal check-ups since the beginning, with four normal ultrasounds; the mother without a history of alcohol or tobacco consumption during pregnancy; The TORCH (Toxoplasma, Rubeola, Cytomegalovirus and Herpes virus) study was negative and an episode of urinary tract infection was treated in the second trimester of pregnancy. NB product of third pregnancy of 38.4 weeks according to date of last menstruation, born by eutocic delivery, with clear amniotic fluid, with anthropometry that corresponded to a full-term newborn appropriate for gestational age (RNTAEG), with weight: 2,950 g, height: 48 cm, head circumference: 34 cm, abdominal perimeter: 31.5 cm, Apgar: 8 at one minute and five minutes.
On initial physical examination, upon admission to the service, he appeared generally well, with vigorous crying that was easy to console. Hemodynamically stable and well hydrated. In the segmental physical examination, a macular lesion was observed, with well-defined irregular edges, of non-uniform color, with dark brown and black tones, partially covered with fine, dark hair, with an approximate diameter of 23.5 cm long x 7.5 cm. cm that covers part of the right dorsolumbar region and the left dorsolumbar region completely, extending along the homolateral flank to the anterior limit, between the mesogastrium and the right flank, respecting the inguinal area. Within this macular lesion, an irregularly shaped nodule (1.5 x 2 cm) was evident, without ulceration, pink in color with traces of dark brown, located in the left thoracolumbar region. (Figure 1). In addition, papules were observed, round in shape, with an average diameter between 2.5 and 3 cm, well-defined, dark brown in color, completely covered with hair (thick, long and black), in number of six, distributed three on the hemibody. left: shoulder, posterior thoracic region and in the gluteal fold, the other three papules with centrifugal distribution on the right hemibody: lower third of the arm on the lateral aspect, upper third of the thigh and on the posterior aspect of the leg above the heel. Also, small nevic lesions were observed distributed in healthy skin spaces on the body, with a predominance in the lower extremities (Figure 1).

Figure 1: Lateral view of neonate exhibiting giant melanocytic nevus (a). Posterior view showing a nodule in the left thoracolumbar region and papules on the extremities (b)s.
The neurological examination revealed preserved primitive postural reflexes (Moro reflex, asymmetric tonic cervical reflex) and cutaneous or tactile reflexes (sucking, searching, crossed extension). The basic laboratory tests they had performed reported a blood count in the normal range. With lactate dehydrogenase (LDH) levels at 2,250 IU/l (160-1,500 IU/l). The histopathological study described an epithelioid nodule, in the vertical growth phase, at level III according to Clark's microstratification and a thickness of 1.3 mm according to Breslow, with no signs of invasion. The molecular study was carried out by extracting genomic DNA from a skin sample (nodule that was inside the macular lesion, pink in color with traces of dark brown) fixed with formalin and impregnated in paraffin (FFPE) using a kit. QIAamp DNA FFPE Tissue. To flank the direct mutagenesis site, two primers were used to introduce a nucleotide change on chromosome 1:115256535 C>G or on chromosome 1:115256532 G>T creating a recognition site for the restriction enzyme Hpy166ll and BsrG1. (New England Biolabs, Ipswich, MA), in the sequence GTNNAC and TGTACA, respectively. The molecular analysis was performed by Sanger sequencing, on the ABITM 3130 Genetic Analyzer of the NRAS gene from the patient's genomic DNA, which showed a p.Q61K mutation in a homozygous state in exon 61. (figure 2).

Figure 2: Chromatogram with genomic DNA sequence showing homozygosity for the mutation c.181C>A, p.Q61K.
Simple magnetic resonance imaging (MRI) of the head and spine identified the absence of lesions in the brain parenchyma and spinal cord, respectively. The Dermatology service reported that a globular reticulum structure was observed in the dermoscopy of the nevi. Based on the clinical findings and the histopathological report, it was concluded that it was a T2bN0M0 melanoma in stage IIA. Therefore, the patient started treatment with Trametinib, according to the dose suggested by the manufacturer. Once the results of the initial examinations and medical evaluations were obtained, the patient was sent home in stable condition, with the pertinent recommendations and clearly defined medical check-ups every three months.
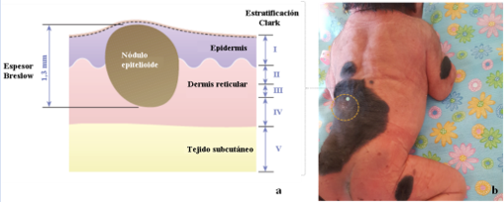
Figure 3: Schematic representation of the epithelioid nodule located within the macular lesion (a), in the left thoracolumbar region (b).
When monitored by a multidisciplinary team, at three months of age, the lesions have increased in proportion to the patient's growth, without the appearance of new lesions. The research protocol was sent to the ethics committee for comment, review and approval; allowing the registration of data about the case and its relatives with the publication of the results later.
Discussion
Malignant melanoma is rare in the pediatric population, accounting for 1% of malignant neoplasms in childhood. It can present from birth as a result of early degeneration of the CMN. In general, 50% of cases with melanoma in childhood come from pre-existing lesions, predominantly from a GCMN, present in 0.1% of births in the world. The nevi are located on the head or neck and are equal to or larger than the palm of the hand, or cover more than 5% of the body surface if they are located on the trunk or extremities [13]. Cutaneous melanoma should be suspected based on the ABCDE criteria (Asymmetry of shape, Irregular edge, Non-uniform color, Large diameter and Elevation); When considering a presumptive diagnosis of cutaneous melanoma based on CMN, it is essential to perform a biopsy (with excision if possible), accompanied by a histopathological study by at least two experts. The literature describes that nodular melanoma (satellite melanoma) is located in the subcutaneous tissue, with the presence of mutations in the NRAS gene, between 80% and 95% of cases diagnosed with GCMN, as one of the main causes in the formation of the CMN [14].
The histopathological study of our case reported the presence of a nodular melanoma, in the vertical growth phase, at level III according to Clark's microstratification and a thickness of 1.3 mm according to Breslow, findings similar to those described in the first case in a research by Belysheva T, et al.(fifteen). There are few cases diagnosed with GCMN that report an autosomal recessive inheritance pattern (due to gonadal gene mosaicism) with loss of heterozygosity of the normal allele [16]. The vast majority are sporadic cases that occur due to genetic mosaicism in melanocytes. Postzygotic mutations in the NRAS gene and possibly in the BRAF, MC1R, TP53, and GNAQ gene loci highlight the importance of NRAS in cell proliferation and differentiation in CMN (17). In research by Kisler VA, et al. Two missense mutations are mainly proposed due to substitution or change in codon 61 of the NRAS oncogene. In 80% of diagnosed cases, the c.181C>A, p.Q61K mutation is present, and in less percentage c.182A>G, p.Q61R [18], There is a greater probability of progression towards malignancy when there is loss of heterozygosity. The individual characteristics of CMN (including the different degrees of severity of each nevus) with the same mutation (c.181C>A) speaks in favor of the variable expressivity and penetrance of this genetic condition.
In an investigation of variants in the MC1R gene, Kinsler VA, et al (2012a) reports the presence of V92M or the R allele (D84E, R151C, R160W, D294H), which is strongly correlated, between the size of the nevus (in northern children of Europe) and the red hair color [19] However, our reported case (of mixed ethnicity) presented black hair, which according to the origin of this ethnic group is 66% native Amerindian, 30
Conclusion
The patient with cutaneous melanoma from the CMN constitutes a case of interest because it is a rare clinical entity in the neonatal age, since showing various shades of color in the macular lesion is highly suggestive of malignancy. Biopsy of the nevus is indicated, even more so when malignant changes are suspected, allowing adequate staging to be defined as a starting point to evaluate the future evolution of the lesion.
Declarations
Protection of people and animals
The authors declare that the procedures followed were in accordance with the ethical standards of the responsible human experimentation committee and in accordance with the World Medical Association and the Declaration of Helsinki.
Data confidentiality
The authors declare that they have followed workplace protocols regarding the publication of patient data.
Right to privacy and informed consent
The authors have obtained informed consent from the patients and/or subjects referred to in the article. This document is in the possession of the corresponding author.
Conflict of interests
The authors declare no conflict of interest.
References
- Price H. (2016). Congenital melanocytic nevi: update in genetics and management. Curr Opinion Pediatr, 28:476-482.
Publisher | Google Scholor - Newton J. (2011). Melanocytic naevi and melanoma. In: Irvine A, Hoeger P, Yan A, editors. Harper's textbook of Pediatric Dermatology. 3rd ed. United Kingdom: Wiley-Blackwell, 1230-1254.
Publisher | Google Scholor - Kopf A, Bart R, Hennessey P. (1979). Congenital nevocytic nevi and malignant melanomas. J Am Acad Dermatol, 1:123-130.
Publisher | Google Scholor - Online Mendelian Inheritance in Man [database on the Internet].
Publisher | Google Scholor - Morelli J. (2013). Cutaneous nevi. In: Kliegman R, Behrman R, Jenson H, Stanton B, editors. Nelson treatise on Pediatrics. 18th ed. Wisconsin: Elsevier Saunders, 2674-2678.
Publisher | Google Scholor - Castilla E, da Graca Dutra M, Orioli-Parreiras I. (1981). Epidemiology of congenital pigmented naevi: I. Incidence rates and relative frequencies. Brit J Derm, 104:307-315.
Publisher | Google Scholor - de la Rosa Carrillo D, Vindenes H, Kinsler VA, Rønnestad A, Ringstad G, Müller L, et al. (2018). Aggressive melanoma in an infant with congenital melanocytic nevus syndrome and multiple, NRAS and BRAF mutation-negative nodules. Pediatr Dermatol, 35:281-285.
Publisher | Google Scholor - Kinsler VA, Abu-Amero S, Bubb P, Jackson IJ, Ring SM, Northstone K. (2012). Germline Melanocortin-1-receptor genotype is associated with severity of cutaneous phenotype in congenital melanocytic nevi: a role for MC1R in human fetal development.J Invest Dermatol, 132:2026-2032.
Publisher | Google Scholor - de la Garza C, Arriaga J, Martínez M, Flores L, Leyva A. (2013). Development of the nervous system. In: Arteaga S, García M, editors. Human embryology and developmental biology.Mexico: Panamericana, 467-470.
Publisher | Google Scholor - Tidyman W, Rauen K. (2009). The RA Sopathies: developmental syndromes of Ras/MAPK pathway dysregulation. Genet Develop, 19:230-236.
Publisher | Google Scholor - Dessars B, De Raeve L, Morandini R, Lefort A, El Housin H, Ghanem G, et al. (2009). Genotypic and gene expression studies in congenital melanocytic nevi: insight into initial steps of melano tumori genesis. J Invest Dermatol, 129:139-47.
Publisher | Google Scholor - Martín A, Bocian M, Bettina A. (2014). Childhood skin tumors. In: JP, Sánchez V, Beltramino N, Copto A, editors. Meneghello Pediatrics. Santiago de Chile: Panamericana, 2447-2453.
Publisher | Google Scholor - Monteagudo B, Labandeira J, Peteiro C, de las Heras C, Cacharrón J. (2009). Giant congenital melanocytic nevus associated with angiolipomas.Med Cut Iber Lat Am, 37:1-7.
Publisher | Google Scholor - Püttgen K, Cohen B. (2012). Cutaneous Congenital Defects. In: Gleason C, Devaskar S, editors. Avery's diseases of the newborn. 9th ed. Philadelphia: Elsevier Saunders, 1406-1421.
Publisher | Google Scholor - Belysheva T, Vishnevskaya Y, Nasedkina T, Emelyanova M, Abramov I, Orlova K, et al. (2019). Melanoma arising in a giant congenital melanocytic nevus: two case reports. Diagnostic Pathology, 14(21):1-9.
Publisher | Google Scholor - Frieden IJ, Williams ML. (1994). Familial site-specific congenital melanocytic nevus: report of two families. Arch Dermatol, 130:1075-1076.
Publisher | Google Scholor - Karp G. (2010). Cell signaling and signal transduction: communication between cells. In: Karp G, editor. Cell and molecular biology. 6th ed. United States of America: Wiley, 605-649.
Publisher | Google Scholor - Kinsler V, Thomas A, Ishida M, Bulstrode N, Loughlin S, Hing S, et al. (2013). Multiple congenital melanocytic nevi and neurocutaneous melanosis are caused by postzygotic mutations in codon 61 of NRAS. J Invest Dermatol, 133:2229-2236.
Publisher | Google Scholor - Kinsler V, Abu-Amero S, Bubb P, Jackson IJ, Ring SM, Northstone K. (2012). Germline Melanocortin-1-receptor genotype is associated with severity of cutaneous phenotype in congenital melanocytic nevi: a role for MC1R in human fetal development. J Invest Dermatol, 132:2026-2032.
Publisher | Google Scholor - Santangelo R, González F, Börstinga C, Torronib A, Pereira V, Morlinga N. (2017). Analysis of ancestry informative markers in three main ethnic groups from Ecuador supports a trihybrid origin of Ecuadorians. Forensic Science International: Genetics, 31:29-33.
Publisher | Google Scholor - Lalor L, Busam K, K S. (2016). Prepubertal melanoma arising within a mediumsized congenital melanocytic nevus. Pediatr Dermatol, 33:372-374.
Publisher | Google Scholor - Kinsler V, Bulstrode N, Calonje J, Chong W, Hargrave D, Jacques T, et al. (2017). Melanoma in congenital melanocytic naevi. Br J Dermatology Linked Comment, 176:1131-1143.
Publisher | Google Scholor - Mir A, Agim N, Kane A, Josephs S, Park J, K L. (2019). Giant congenital melanocytic nevus treated with trametinib. Pediatricia, 143(3):1-4.
Publisher | Google Scholor














