

Review Article
Cosmetic and Theatrical, Esthetic and Preventive, Dentistry
McGill University Faculty of Dental Medicine and Associated Oral Health Sciences, Montreal, Canada.
*Corresponding Author: Louis Z.G. Touyz,McGill University Faculty of Dental Medicine and Associated Oral Health Sciences, Montreal, Canada.
Citation: Louis Z.G. Touyz. (2024). Cosmetic and Theatrical, Esthetic and Preventive, Dentistry. Dentistry and Oral Health Care, Biores Scientia Publishers 3(3):1-8. DOI: 10.59657/2993-0863.brs.24.037
Copyright: © 2024 Louis Z.G. Touyz, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 12, 2024 | Accepted: June 29, 2024 | Published: July 13, 2024
Abstract
Cosmetics commonly perceived as beautifying artefacts for skin may but implicates teeth. Although Cosmetic Dentistry (CD) aims at providing immediate appearance improvement, CD is not permanent, may produce unwanted cellular reactions, is often gratuitously decorative, is not necessarily ideally functional and often demands tissue-accommodation. Esthetic dentistry (ED) needs no physical accommodation or tolerance, is long-term durable, provides optimal good function, emulates natural state, promotes health, is not frivolously decorative, sustains ideal form, and uses best techniques and materials. This appraisal re-affirms differences between them and indicates that the zenith of Cosmetic Dentistry is Theatrical Dentistry (TD) and the ultimate ideal of Esthetic Dentistry is Preventive Dentistry (PD).
Keywords: cosmetic; esthetic; preventive; theatrical dentistry; form; function
Introduction
Provenance
The term ‘Cosmetic’ comes from the Greek (κοσμήτικοϩ f. κοσμϵίν) meaning to adorn or arrange [1]. It indicates owning the magic or skills to beautify; any material used to glamorize skin, facial complexions or hair is called a cosmetic. In dentistry the notion of improving a smile implies Cosmetic Dentistry that tries to beautify teeth. Yet practical dental therapy has changed and matured over millennia into two manifestly different approaches, each with different guiding principles that determine policies of practice: they are regarded as Cosmetic or Esthetic Dentistry. [2,9].
Aim
This appraisal re-affirms the principal differences between Cosmetic Dentistry (CD) and Esthetic Dentistry (ED) and indicates that the zenith of CD is Theatrical Dentistry (TD), and the ideal Esthetic Dentistry (ED) is Preventive Dentistry (PD).
Discussion
Cosmetic and Esthetic Dentistry are not the same: see Table 1.
Table 1: Differences between Cosmetic and Esthetic Dentistry. From: - TOUYZ LZG, Raviv E, Raviv, M Cosmetic and Esthetic Dentistry? Quintessence International 1999. 30”:227-233 [2].
| Cosmetic Dentistry | Esthetic Dentistry |
| Minimal accommodation or tolerance | No physical accommodation or tolerance |
| Consciously temporary | Long-term durable |
| Not ideally functional | Optimal good function |
| No natural emulation | Emulates natural state |
| No health enhancement | Promotes health |
| Superfluous decoration | No decoration |
| Compromised form | Form ideal |
| Available technique and material. | Best technique and materials |
Cosmetic Dentistry always modifies appearance. Unnatural colors applied to teeth are regarded as cosmetic. See Figure 1. Frivolous decoration in Dentistry is regarded as cosmetic. This can modify selection, design and execution of full or partial prostheses. [5] See Figure1, 2 and 3.
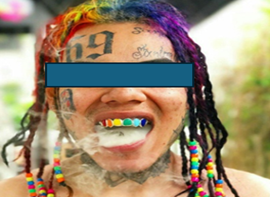
Figure 1: There are six various tooth colors placed onto the anterior maxillary incisors and canines. This is Cosmetic Dentistry and is deemed to be Theatrical Dentistry. Rainbow-teeth Hash Tags-Deskgram 2018 [5,6].

Figure 2: Inlaid Enamel into Gold: A full upper prosthesis and lower removable partial Prosthesis. This does not emulate nature even though it is a technically accomplished skill. The wavy curved gold outlines on a pink base do not mimic pristine nature. The use of metal does render strong rigidity, reduces prosthetic bulk, improves strength, and can be long-lasting, but the frivolous decoration qualifies these prostheses as cosmetic dentistry. Gratuitous ‘prettification’ is typical of Cosmetic Dentistry.

Figure 3: Cosmetic Dentistry: Upper front incisors and canines replaced with removable acrylic prosthesis, and Tooth-18 [ADA numeration] is frivolously decorated with a gold $ sign, and Tooth-19 has a class IV gold inlay on the distal and incisal edges [2].
The use of metal as shiny jewelry, diamonds, crystal or colored stones all meet the criteria of these into the category of cosmetic dentistry. See Figures 4-7.

Figure 4: Cosmetic dental diamonds. Emerald-cut diamonds, set into gold crowns on teeth 17,& 28 [ADA numeration]. This example of metal-and-diamonds. (MAD) with frivolous decoration is regarded as flippant, and deemed Cosmetic Dentistry. The dentition ideally should not be deemed as sites for jewel-placement but preferably as operating biological organs. Ref: Touyz LZG, Lamontagne P, Mojon P. Diamonds and Cosmetic Dentistry. Restorative and Aesthetic Practice. 2004 Dec. 6(4) 10-17 [8].

Figure 5: There is a circular brilliant-cut diamond set in white gold, inlaid into the natural enamel of tooth-21 [ADA tooth numerical system]. This is an example of MAD. This dentistry does not mimic unblemished nature and qualifies as Cosmetic Dentistry [7,8].

Figure 6: This is a removable, diamond-and-gold splint covering teeth -15, -16, -17; -18-, -19, -20, -21, &-22 (ADA tooth numerical system), constructed in gold and encrusted with diamonds. This GAD (gold-and diamond) is expected to be placed over natural teeth and function an adornment jewelry. It is constructed to fit onto the wearers’ anterior eight teeth. This does not copy anything in nature and accordingly it is regarded as Cosmetic Dentistry [7].

Figure 7: A metal (gold) and diamond splint (GAD) shown in Figure 10 above, is placed in situ. The GAD Shows the incisal tips of the anterior incisal teeth. This type of dentistry does not copy or enhance nature and is judged cosmetic [7].
The acme of Cosmetic Dentistry is Theatrical Dentistry [6] See Figure 8.

Figure 8: By replacing phony false tapering elongations onto the canines, an animalistic, unnatural appearance is produced. This add-on miscegenation of teeth evokes the imagination to see unnatural wild carnivore canines seen in cats, tigers or snakes. This is frequently used in horror movies. This is typical example of Theatrical Dentistry.
Theatrical Dentistry (TD) alters the mission of esthetic dentistry in that it ignores the aims of therapy, durability, survival, and function. All of TD is conceived to procure a modified appearance. Esthetic Dentistry (ED) expects all the positive aspects of therapy to be realized to the maximum, as ED’s mission and aims do not tolerate any compromise. The mission of Cosmetic Dentistry is consciously impermanent and a compromise, but aims at-, and expectations of-, some qualified appearance change with reduced optimal function. The mission of Theatrical Dentistry is strictly ephemeral, successfully altering appearance to a desired appearance form with mouth modification. Should restorative dentistry induce unwanted cellular reactions, it is judged to be cosmetic. [3] See Figures 9->12.

Figure 9: Cosmetic crowns. The front upper central incisors [Tooth-18 and Tooth-19 ADA numerology] are treated with fixed crowns. A reactive marginal gingival hyperplasia has developed around the margins. This is deemed to be Cosmetic Dentistry and needs attention.

Figure 10: Cosmetic crowns. Tooth 18 and tooth-19 [ADA numeration] impact on the biologically width (BW) sub-gingivally, and the adjacent surrounding gingivae have changed in color, show inflammatory hyperplasia. Are swollen and manifest bleeding on probing (BOP) is positive [3].

Figure 11: A cosmetic crown placed on Tooth-18 (ADA numerology). The embracing marginal gingivae are inflamed, bleed on probing and are swollen. This cellular tissue response comes from the subgingival crown margins impacting on the BW, the width demanded for enduring healthy dento-gingival attachment [3].

Figure 12: An esthetic crown was constructed and fitted onto the same Tooth-18 as in Figure-11 above. The gum and adjacent dentoalveolar bone were shaped (ostectomy and osteoplasty) with a ‘Clinical Crown-lengthening’ (CCL) periodontal surgical procedure. Gingival inflammation is absent, with no BOP (Bleeding-On-Probing), and the outcome resolved to a healthy permanent, sustainable and durable gingival architecture. The new esthetic crown does not occupy or damage the BW. Healthy tissue is present. This is ideal Esthetic Dentistry [3].
The ultimate success of Esthetic dentistry is preventive dentistry [11]. Any dentistry that is not sustainable in health with function for years is considered as cosmetic. Osseo integrated implants are often used in the esthetic zone (Teeth seen in a smile), but because the implants with crowns are anticipated to last for decades, if not a lifetime, they may be classed as esthetic dentistry [4].

Figure 13: A natural healthy dentition; The health of this pristine natural beauty was attained by sustained home oral Hygiene and regular visits for "prophylaxis" provided by professionals.
The growth development and sustaining natural teeth in excellent condition and function for a lifetime through preventive dentistry is the ultimate mission of all health care workers, but especially Dental health care providers.

Figure 14: Cosmetic Dentistry: The dentition is restored and provides tolerable, but not ideal, form and function. Pre-operative view.

Figure 15: Esthetic Dentistry with post-operative view, showing full mouth rehabilitation with esthetic dental techniques. Note recovery of healthy soft tissues, the gum-margin adaptation, and absence of gingival inflammation. With good oral hygiene this result can last decades.
Dentistry has evolved into a highly disciplined biomedical based discipline and profession. [9] The scientific principles that determine policies, processes and pragmatic execution of dental therapy are basic factors in guiding all dental health care providers. Most people demand their dentists provide them with a “Hollywood Smile”. But nothing can improve a natural healthy dentition. Any unnatural modification to a natural dentition may be regarded as cosmetic. Historically, colored stones were set into human-teeth; coloring teeth black, or specific ritualistic mutilations as tribal identifiers are known [10-16]. All these practices are seen as Cosmetic Dentistry as none mimic pristine Nature. Exploitation of growth factors with orthodontics and major foundation osseous reshaping using orofacial and maxillofacial surgery, is regarded as esthetic improvements, as they are intended to promote health and last for a lifetime. These practices influence appearance and may be judged partially as partly cosmetic should they fail to achieve the permanent harmonious perceptions intended [17].
Esthetic (ED), Cosmetic (CD) and Theatrical Dentistry (TD) may have minor similarities, but all different from each other, and each are all clearly moderated and constrained by very different principles. Preventive dentistry is the management and guidance of Nature to render a person oro-dentally healthy to be in excellent shape and function for the duration of their entire lives. The obvious overlaps from CD to ED and even to TD, are illustrated by the mini-reviews and examples above to illustrate these differences. (See figures above) Esthetic Dentistry is more expensive than Cosmetic Dentistry. Inferior, flashy-fashion ‘crazes’ may pressure people to demand spurious dental changes that may have a place in fashion or Theatrical Dentistry in which short-term emotional appeal is exploited, but the principled practice-ideals of dentistry should not be compromised by resorting to Cosmetic Dentistry.
Concluding Remarks: Esthetic Dentistry is more costly than Cosmetic Dentistry. Contemptable, social practices that may find support in frivolous fads with Cosmetic or Theatrical Dentistry. Short-term hedonist emotional appeal is often exploited but the honorable mission of dentistry should not be abused by using Cosmetic Dentistry. The growth development and sustaining natural teeth in excellent condition and function for a lifetime through preventive dentistry is the ultimate mission of all health care workers, but especially Dental health care providers [17,18].
Conclusion
The growth development and sustaining natural teeth in excellent condition and function for a lifetime through preventive dentistry is the ultimate mission of all Medical Health Care Workers, but especially Dental Health Care providers in Dentistry.The ultimate Cosmetic-Dentistry is Theatrical- Dentistry, and the zenith of Esthetic-Dentistry is Preventive-Dentistry.
Author statement: The Author has no conflict of interest to declare.
References
- Little W., Fowler H.W. Coulson J. (1972). The Shorter Oxford English Dictionary. Third Ed. The Oxford at The Clarendon Press, 1:401.
Publisher | Google Scholor - Touyz L.Z.G., Raviv E, Raviv, M. (1999). Cosmetic and Esthetic Dentistry. Quintessence International, 30:227-223.
Publisher | Google Scholor - Touyz L.Z.G. (2023). Tissue Accommodation Matters: In Esthetic and Cosmetic Dentistry. ICARE. International Case Reports, 2(2):1025.123-127.
Publisher | Google Scholor - Touyz L.Z. G .and Nassani LM. (2023). Osseointegrated Implants Deemed Cosmetic or Esthetic. Scientific Archives of Dental Sciences, 6(2):05-07.
Publisher | Google Scholor - Touyz L.Z.G. (2018). “Cosmetic Dentistry: Unnatural Coloring of the Dentition”. Oral Health and Dentistry, 3(5):744-750.
Publisher | Google Scholor - Touyz L.Z.G. (2016). Theatrical Dentistry. Principles and practice. Journal of Cosmetology and Maxillofacial Surgery, 2:106.
Publisher | Google Scholor - Touyz L.Z.G. (2023). Cosmetic Dentistry and Decorative Diamonds in Prosthodontics. ICARE. 2(3):1031
Publisher | Google Scholor - Touyz L.Z.G, Lamontagne P, Mojon P. (2004). Diamonds and Cosmetic Dentistry. Restorative and Aesthetic Practice. 2004 Dec. 6(4):10-17.
Publisher | Google Scholor - Gutman J. (1976). The Evolution of America's Scientific Advancements in Dentistry in the Past 150 Years. Passim. Journal of the American Dental Stomatologica, 25(1):33-48.
Publisher | Google Scholor - Van Reenen J.F. (1977). Swallow-tail form of tooth mutilation amongst early Iron-Age people living at Broederstroom Transvaal, circa 500AD. Jnl of the Dent Asstn of S Afr, 32(9) 529-533.
Publisher | Google Scholor - Flynn M. (1977). Black teeth: a primitive method of caries prevention in Southeast Asia. Jnl Am Dent Ass, 95:96-97.
Publisher | Google Scholor - Ai S., Ishikawa T., Seino A. (1965). “Ohaguro” traditional tooth-staining custom in Japan. Int Dent J. 5(4):426-441.
Publisher | Google Scholor - Fastlicht S. (1976). Tooth mutilations and Dentistry in pre-Columbian Mexico. Passim. Quintessence Books. 1976. Berlin.
Publisher | Google Scholor - Fitton F.S. (1993). A tooth ablation custom in the Maldives. Br Dent Jnl, 175(8):299-300.
Publisher | Google Scholor - Jones A. (2001). Dental transfigurements in Borneo. Br Dent Jnl, 191(2):98-102.
Publisher | Google Scholor - Jones A. (1992). Tooth mutilation in Angola. Br Dent Jnl, 173(5):177-179.
Publisher | Google Scholor - Touyz L.Z.G. (2018). Sanative dentistry: Bringing sanity back into dentistry. Scientific Archives of Dental Sciences, 1:115-19.
Publisher | Google Scholor - Touyz L.Z.G. (2024). “After a Centuries of Dentistry. Prevention Remains Best
Publisher | Google Scholor











