

Case Report
Clinical Case of Simultaneous Coronary and Neuro Intervention in A Patient with Multifocal Lesions
- Kolisnik V
- Peleshenko A
- Oleksiy V. Goriachyi *
- Brovarskaya O
Department of interventional cardiology and neuroradiology, Odessa Regional Hospital, Ukraine.
*Corresponding Author: Oleksiy V. Goriachyi, Department of interventional cardiology and neuroradiology, Odessa Regional Hospital, Ukraine
Citation: Kolisnik V, Peleshenko A, Oleksiy V. Goriachyi, Brovarskaya O. (2023). Clinical Case of Simultaneous Coronary and Neuro Intervention in A Patient with Multifocal Lesions, Journal of Clinical Research and Clinical Trials, BRS publishers. 2(2); DOI: 10.59657/2837-7184.brs.23.011
Copyright: © 2023 Oleksiy V. Goriachyi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 13, 2023 | Accepted: June 05, 2023 | Published: June 12, 2023
Abstract
Multifocal atherosclerotic disease is most severe of cardiovascular pathology, which associated with significantly higher rate of MACCE, mortality, rehospitalization that requires multidisciplinary approach, multimodality imaging, complex treatment algorithm. Both, endovascular procedure and optimal medical therapy are used for each CAD and CVD. A hybrid simultaneous interventional procedure with using new antithrombotic agent may become a solution for improvement of outcomes in patients with Acute Coronary Syndrome and TIA/Stroke.
Keywords: coronary; neuro; multifocal lesions patient; hypertension; diabetes; dyslipidemia; mild renal impairment
Introduction
This presentation emphasizes the depth of multifocal atherosclerosis, its simultaneous presentation, and possible combined surgical treatment. We describe a clinical case of a 67-year-old male with severe cardiac and cerebral symptoms and multiple comorbidities. He underwent a hybrid interventional procedure performed jointly by the cardiac and interventional teams.
Case presentation
A 67-year-old male with history of multiple illness including: hypertension, diabetes, dyslipidemia, mild renal impairment, coronary artery disease. Patient was hospitalized to ED with recurrent transit ischemic attacks (TIAs) combining with NSTEMI-MI. At the time of the examination, the patient complained of diffuse headache, marked general weakness, increased blood pressure up to 190/120 mmHg, weakness in the left side extremities and numbness of the tongue, recurrent chest pain. The patient had episodes of unconsciousness twice at home without seizures.
The 12-lead electrocardiogram (ECG) showed ST segment depression in V2–V6 leads. Transthoracic echocardiogram was performed, which showed preserved cardiac function (EF – 50%), with aortic sclerosis, anterior LV wall hypokinesis (mostly interventricular septal segments). Hb -112 g/l, creatinine – 1.28mg/dL, Troponin 1.8ng/ml. Cerebral CT demonstrated severe kinking C1 and critical stenosis of the Right ICA and MCA (Figure 1).
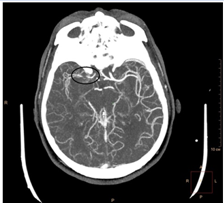
Figure 1: CT showed 95-99% stenosis right MCA.
To clarify the cardiac and neurologic diagnosis a coronary and cerebral angiogram was planned. Selective carotid/cerebral angiography showed right internal carotid artery stenosis C2 segment 70-75%, and intracranial Right MCA in the M1 segment has critical stenosis of 95-99% blood flow TIСI 1-2 (Figure 2).
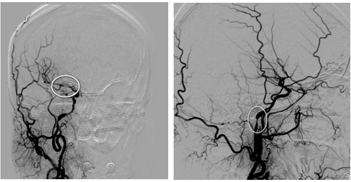
Figure 2: Selective carotid/cerebral angiography showed 95-99% right MCA stenosis and C2 ICA stenosis 70%, severe kinking C1
Coronary angiography showed critical narrowing along the anterior interventricular branch of the left coronary artery 90% in the proximal segment, 75-80% in the middle segment and 70-80% in the marginal branch (Figure 3).
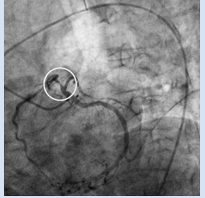
Figure 3: Selective coronary angiography showed critical narrowing along the anterior interventricular branch of the left coronary artery 85-90% in the proximal segment.
The simultaneous endovascular procedure was performed. Transfemoral approach, anesthesia–local+ sedation, antithrombotic agent–Cangrelol 30mcg/kg bolus and followed by a 4mcg/kg/min infusion via IV line. The first stage was neuro intervention:
- Angioplasty M1 segment right MCA with thrombo aspiration technique
- Angioplasty stenosis C2 segment ICA.
A Neuro max 6F guiding catheter was placed in the distal right common carotid artery. A pressurized flushing system was set up. A Distal access catheter Sophia 5F with coaxial system neuro wire Traxess 0.014 +and Neuro speed 2.5x 8 mm intracranial balloon (3 -4 atm) were used. The ball on inflation lasted 10 sec with next following aspiration via Penumbra System. After that, balloon angioplasty was performed in C2 segment ICA using Neuro speed 2.5x 8 mm (8 -10 atm) intracranial balloon. Control angiography was performed with result TICI 3. (Figure 4).
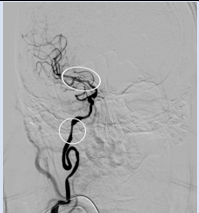
Figure 4: Restoration of blood flow in the intracranial section of the internal carotid artery and the M1 segment of the right spinal artery
The second stage was coronary artery stenting. A guidewire system was inserted into the left coronary artery. Predilatation with a 2.5 x 15 mm balloon was performed (p 11-12 atm) in the proximal LAD. DES Resolute Integrity 2.75 x 14 mm (p11 -12 atm) was implanted. Control angiography was performed with a positive angiographic result TIMI3 (Figure 5).
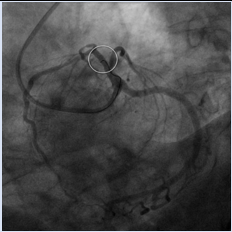
Figure 5: Restoration of blood flow in the left anterior descendance artery
The closer device Angio Seal. Duration of procedure 85min, contrast–210ml. There was not any complication. Optimal medical therapy: Ticagrelor 90mg x twice per day, Aspirin 75mg, Rosuvastatin 20mg. Patient discharged on the fourth day.
Discussion
Angiography and stenting of carotid and coronary arteries are becoming part of routine interventional practice and are widely performed by appropriately trained and qualified specialists. Each procedure has its own indications and contraindications, its own risks, its own techniques, and areas of application. It requires appropriate knowledge and experience and specialized medical instruments. In clinical practice, we are often confronted with these procedures being performed separately, sometimes even at different time intervals. This leads to a loss of precious time for the patient.
Of course, there are reasons and indications for this too. However, after carefully weighing and weighing up the risks and benefits, we are more inclined toward the simultaneous performance of such interventions. Firstly, the X-ray burden on the staff and the patient is significantly reduced. Repeated interventions always exponentially increase the risk of infection and septic complications. Most importantly, the patient receives all necessary care at once, without losing any time. This significantly increases the chances of subsequent recovery. This reduces the length of hospital stay and the overall financial burden on the healthcare system as a whole.
Acknowledgment
We present this case to raise awareness of the extent of atherosclerosis and the possibility of combined surgery. To date, many authors have presented similar data. We, in turn, once again want to emphasize the possibility of such interventions.
Conflict of Interest
No Conflict of Interest.
References
- Yadav JS, Roubin GS, Iyer S, Vitek J, King P, et al. (1997). Elective stenting of the extracranial carotid arteries. Circulation. 95(2):376-381.
Publisher | Google Scholor - Roubin GS, New G, Iyer SS, Vitek JJ, Al-Mubarak N, et al. (2001). Immediate and late clinical outcomes of carotid artery stenting in patients with symptomatic and asymptomatic carotid artery stenosis: a 5-year prospective analysis. Circulation. 103(4): 532-537.
| Google Scholor - Morey SS. (1998). AHA updates guidelines for carotid endarterectomy. Am Fam Physician 58(8):1903-1904.
Publisher | Google Scholor - Wholey MH, Al-Mubarek N, Wholey MH. (2003). Updated review of the global carotid artery stent registry. Catheter Cardiovasc Interv. 60(2):259-266.
Publisher | Google Scholor - Al-Mubarak N, Liu MW, Dean LS (1999) Incidences and outcomes of prolonged hypoten
Publisher | Google Scholor - Mas JL, Chatellier G, Beyssen B, Branchereau A, Moulin T, et al. (2006). Endarterectomy versus stenting in patients with s.
Publisher | Google Scholor - Ringleb PA, Allenberg J, Bruckmann H, Eckstein HH, Fraedrich G, et al. (2006). 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised non-inferiority trial. Lancet. 368(9543):1239-1247.
Publisher | Google Scholor - Cremonesi A, Setacci C, Manetti R, de Donato G, Setacci F, et al. (2005). Carotid angioplasty and stenting: lesion related treatment strategies. EuroIntervention 1(3):289-295.
Publisher | Google Scholor - Gilutz H, Shindel S, Shoham-Vardi I. (2019). Adherence to NSTEMI Guidelines in the Emergency Department: Regression to Reality. Crit Pathw Cardiol. 18(1):40-46.
Publisher | Google Scholor - Piątek Ł, Wilczek K, Janion-Sadowska A, Gierlotka M, Gąsior M, Sadowski M. (2019). Outcomes of a routine invasive strategy in elderly patients with non-ST-segment elevation myocardial infarction from 2005 to 2014: results from the PL-ACS registry. Coron Artery Dis. 30(5):326-331.
Publisher | Google Scholor - Alpert JS, Thygesen K, Antman E, Bassand JP. (2000). Myocardial infarction redefined--a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 36(3):959-969.
Publisher | Google Scholor - Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD., ESC Scientific Document Group. (2019). Fourth universal definition of myocardial infarction (2018). Eur Heart J. 40(3):237-269.
Publisher | Google Scholor - Wilson PW. (1994). Established risk factors and coronary artery disease: the Framingham Study. Am J Hypertens. 7(7 Pt 2):7-12.
Publisher | Google Scholor - Canto JG, Kiefe CI, Rogers WJ, Peterson ED, Frederick PD, French WJ, Gibson CM, Pollack CV, Ornato JP, Zalenski RJ, Penney J, Tiefenbrunn AJ, Greenland P. (2011). NRMI Investigators. Number of coronary heart disease risk factors and mortality in patients with first myocardial infarction. JAMA. 306(19):2120-2127.
Publisher | Google Scholor - Hartikainen TS, Sörensen NA, Haller PM, Goßling A, Lehmacher J, Zeller T, Blankenberg S, Westermann D, Neumann JT. (2020). Clinical application of the 4th Universal Definition of Myocardial Infarction. Eur Heart J. 41(23):2209-2216.
Publisher | Google Scholor











