

Case Report
Chondrodysplasia: Thanatophoric Dwarfism, Diagnosis and Management
- Marwen Nadia 1*
- Fdhila Sana 2
- Aidi Hadhami 1
- Hammadi Jawaher 1
- Ben Ali Yassmine 1
- Dhouibi Maryam 1
- Tarhouni Khouloud 1
- Khalfaoui Aymen 1
- Dinari Amrou 1
- Bayoudh Imen 3
1Gynecology and Obstetrics Department, Kairouan, Tunisia.
2Faculty of Medicine, Monastir, Tunisia.
3Family Planning, Fathat Hached, Sousse, Tunisia.
*Corresponding Author: Marwen Nadia, Gynecology and Obstetrics Department, Kairouan, Tunisia.
Citation: Nadia M., Sana F., Hadhami A., Jawaher H., Yassmine B.A., et al. (2024). Chondrodysplasia: Thanatophoric Dwarfism, Diagnosis and Management, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 1(5):1-4. DOI: 10.59657/2997-6103.brs.24.028
Copyright: © 2024 Marwen Nadia, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 29, 2024 | Accepted: October 11, 2024 | Published: October 18, 2024
Abstract
Osteochondrodysplasic are constitutional bone diseases responsible for an elective disorder of skeletal growth, structure or morphology. They bring together abnormalities in the growth or structure of bone or cartilage. Thanatophoric dwarfism (NT) is the most common osteochondrodysplasic. It is a lethal disease consisting of two types: I and II. It is caused by a mutation of the FGFR3 (fibroblast growth factor receptor 3) gene located on the short arm of chromosome 4. We report the case of a 34-year-old patient who consulted our maternity ward in labor, at a term of 39 weeks of amenorrhea. She delivered a female newborn with short upper and lower limbs, macrocephaly, narrow chest and prominent abdomen. One hour after delivery, she suffered an acute respiratory distress, extreme bradycardia and died shortly after.
Keywords: osteochondrodysplasic; thanatophoric dwarfism; diagnosis; prenatal ultrasound; management
Introduction
Osteochondrodysplasic include a heterogeneous group of constitutional bone diseases responsible for an elective disorder of skeletal growth, structure or morphology. They combine abnormalities in the growth or structure of bone or cartilage [1]. Among these chondrodystrophies, some are still lethal such as thanatophoric dwarfism [2].
Described by Maroteaux for the first time in 1967 [1], thanatophoric dwarfism (NT) is a rare malformation. Its incidence is estimated at 1/20 000 to 1/40 000 births [2]. It is constantly lethal. Therefore, a prenatal diagnosis is necessary as early as possible to practice a medical termination of the pregnancy with the least psychological repercussions [3]. The diagnosis would be based on ultrasound, possibly associated with the radiography of the uterine contents.
Clinical Observation
This is a 34-year-old patient, tertigravida, bipara, with no notable medical history. During her first pregnancy, she gave birth naturally, without incidents, of a healthy male newborn. It was later followed by a spontaneous miscarriage. No notion of consanguinity was noted. Although her pregnancy is carried out until 39 weeks of amenorrhea, the patient did not have regular checkups. Therefore, no morphological ultrasound was performed. She consulted our maternity ward in labor. She gave birth naturally, without incidents. After delivery, on examination the newborn was female with short upper and lower limbs, a macrocephaly, a narrow thorax and a prominent abdomen. Her height was 38cm (Figure 1).

Figure 1: Macroscopic appearance of the newborn.
She suffered an acute respiratory distress, extreme bradycardia and died 1 hour after delivery. The diagnosis of thanatophoric Dwarfism was suspected. Therefore, it was supplemented by a radiological examination of the skeleton (Figure 2) and a pathological examination of the newborn that confirmed the diagnosis.
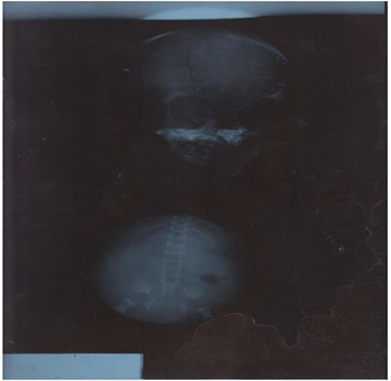
Figure 2: Radiological aspect of the newborn.
Discussion
The malformations of the limbs constitute a large heterogeneous group of skeletal anomalies. Their incidence is estimated at 1/5000 births [1,2]. The lethal forms of these osteochondrodysplasic form a group of rare affections. Their frequency is estimated at 1 / 10,000 births. Since the first description of a chondrogenesis by Parenti, numerous cases of lethal osteochondrodysplasic have been published, in this case thanatophoric dwarfism [4]. The latter is a major lethal fetal malformation. It is inherited via an autosomal dominant gene. It is due to a mutation of the FGFR3 gene (fibroblast growth factor receptor 3) located on the short arm of chromosome 4 [4]. The researchers described two major forms of thanatophoric dysplasia, type I and type II. The frequency of this disease is estimated to be 1: 6400 to 1: 100000 births [3,4].
The prenatal discovery of thanatophoric dwarfism requires the practice of a therapeutic termination of the pregnancy [3]. Thus, the prenatal diagnosis of these lethal skeletal malformations is valuable. Some authors encourage the search for these morphological abnormalities as early as the first trimester ultrasound [6,7]. The first trimester ultrasound should focus on the nuchal translucency. According to Tonni et al [8], an increased nuchal translucency is an early sign frequently associated with thanatophoric dwarfism. The amount of amniotic fluid must also be taken into account. In fact, hydramnios is a clinical and ultrasound sign that is constantly associated with thanatophoric dwarfism [1,4]. According to Schramm et al, the diagnosis of skeletal abnormalities is essentially made during the second trimester with an accuracy between 30 and 50%. However, 85% of lethal skeletal abnormalities can be diagnosed in the first trimester [9].
According to Trotter [10], the skeletal study of limbs is preferentially between 19 and 22 weeks of amenorrhea. This study is based on the combination between ultrasound, radiological and sometimes biochemical tests. Indeed, the ultrasound diagnosis of thanatophoric dwarfism can be performed from 14 weeks of amenorrhea. Thus, a femoral or humeral length less than 5% or -2DS of the average should make the diagnosis suspect and should be reevaluated in a specialized center to provide genetic counseling. The direct signs of thanatophoric dwarfism, as well as the classification in type I or II, can be obvious from the second trimester. In fact, the ultrasound can show a macrocephaly, a narrowness of the thorax, a prominent abdomen and extremely shortened limbs. In type I, the femur is curved while it is not in type II. Recent advances in technology have further facilitated the diagnosis of thanatophoric dwarfism, with an easier access to a three-dimensional ultrasound [10]. However, sometimes it may be needed to perform a molecular biology examination, which gives the diagnosis of certainty [4,8]. Table 1 illustrates the ultrasound features of the prenatal diagnosis in case of thanatophoric dwarfism compared with other osteochondrodysplasic.
Table 1: Main radiographic abnormalities of lethal osteochondrodysplasic.
| Thanatophoric Dwarfism | Osteogenesis Imperfecta | Achondroplasia |
| Appearance Of Clover Skull | Crane Little Ossified. | Crane Little Ossified. |
| Ossified Vertebrae, Flat | Vertebrae And Pelvis Very Little Ossified. | Vertebrae And Pelvis Very Little Ossified. |
| Short Odds | Odds Sometimes Fractured. | Short Odds. Narrow Chest. |
| Curved Short Limbs | Demineralized Limbs, Short, Deformed, Curved and Sometimes Fractured. | Demineralized Members. |
In case of doubt, it would be desirable to associate the ultrasound with a radiograph of the uterine contents [8]. Moreover, in case of difficulty of diagnosis, some authors propose the realization of a CT scan [11]. According to a retrospective study, 50 pregnant women between 28 and 39 weeks of amenorrhea presented fetal skeletal abnormalities in the ultrasound; The purpose of this work was to correlate the CT aspects with those of the ultrasound in the antenatal diagnosis of skeletal abnormalities. This study concluded that the results of the ultrasound and the CT scan were consistent, but the latter should be limited in the case of late detection of skeletal abnormalities [11]. The morphotype of these newborns varies according to the type of osteochondrodysplasic. However, the common signs are extremely short and curved members, often associated with a narrow thorax and facial dysmorphism [12,13] (Table 2).
Table 2: Main macroscopic aspects of lethal osteochondrodysplasic.
| Thanatophoric dwarfism | Very short, curved limbs |
| Macrocephaly with trunk of normal length | |
| Facial dysmorphism | |
| A chondrogenesis | Extremely short limbs |
| Generalized edema | |
| Osteogenesis imperfecta | Members are very short and curved |
| Macrocephaly | |
| Facial dysmorphism |
The life expectancy of newborns with thanatophoric dwarfism is evaluated, by Noah et al [4], at about one hour after birth. However, rare cases of survival up to five and eight years of age have been reported. According to Pietryga et al, neonatal death is often due to severe respiratory distress related to the narrowness of the thoracic cavity with no lung development [6]. In our observation, the newborn died immediately, one hour after delivery.
Some risk factors could be identified. Thus, advanced maternal age is considered to be a major risk factor for this type of malformation [14]. The consanguinity of the couple is frequently found in the literature [14]. In the Lahmar-Boufaroua study, consanguinity was found in 61% of cases [3]. The age of our patient was 34 years old, and no notion of consanguinity was found in our case.
Conclusion
Thanatophoric dwarfism is a major and lethal skeletal malformation. Antenatal diagnosis is imperative and essential. In the absence of molecular biology, obstetrical ultrasound, sometimes coupled with radiography of the uterine contents, enables an early diagnosis.
Fetal CT scan has very limited indications. Studies have not shown its superiority over ultrasound in the prenatal diagnosis of skeletal abnormalities. An early prenatal diagnosis makes it possible to terminate the pregnancy with the least psychological impact.
Declaration of Competing Interest
The authors have no conflicts of interest relevant to this article.
References
- Maroteaux P, Lamy M, Robert J.M. (1967). Thanatophoric Dwarfism. Presse Med. 75:2519-2524.
Publisher | Google Scholor - Orioli I.M, Castilla E.E, Barbosa-Neto J.G. (1986). The Birth Prevalence Rates for The Skeletal Dysplasia’s. J Med Genet. 23:328-332.
Publisher | Google Scholor - Lahmar-Boufaroua A, Yacoubi M.T, Hmisssa S, Selmi M, Korbi S. (2009). Lethal Osteochondrodysplasia: A Photo Pathological Study of 32 Cases. Tunisia Med. 87(2):127-132.
Publisher | Google Scholor - Noe J, Yoo HW, Kim KN, Lee SY. (2010). A Case of Thanatophoric Dysplasia Type I With an R248C Mutation in The FGFR3 Gene. Korean J Pediatr. 53(12):1022-1025.
Publisher | Google Scholor - Machado LE, Bonilla-Musoles F, Osborne NG. (2001). Thanatophoric Dysplasia. Ultrasound Obstet Gynecol. 18:85-86.
Publisher | Google Scholor - Pietryga M, Iciek R, Brazert M, Wender-Ozegowska E, Brazert J. (2010). Thanatophoric Dysplasia-Case Report. Ginekol Pol. 81(1):55-60.
Publisher | Google Scholor - Petitcolas J, Couvreur A, Leboullenger P, Rossi A. (1994). Interest of Early Morphological Ultrasonography for The Detection of Chromosomal Abnormalities. J Gynecol Obstet Biol Reprod. 23(1):57-63.
Publisher | Google Scholor - Tonni G, Azzoni D, Ventura A, Ferrari B, Felice CD, et al. (2010). Thanatophoric Dysplasia Type I Associated with Increased Nuchal Translucency in The First Trimester: Early Prenatal Diagnosis Using Combined Ultrasonography and Molecular Biology. Fetal Pediatr Pathol. 29(5):314-322.
Publisher | Google Scholor - Schramm T, Gloning KP, Minderer S, Daumer-haas C, Rtnage HKO, et al. (2009). Prenatal Sonographic Diagnosis of Skeletal Dysplasia’s. Ultrasound Obstet Gynecol. 34:160-170.
Publisher | Google Scholor - Trotter Kouamé, Anne-Marie N’goan-Domoua, Roger-Daniel N’gbesso, Abdul-Kader Kéita. (2011). Antenatal Diagnosis of a Case of Thanatophore Dwarfism Type I. Female Imaging. 21:171-175.
Publisher | Google Scholor - Boubbou A, Belarbi N, Alison M, Sebag G. (2009). Contribution of Fetal Skeletal Scanning in the Diagnosis of Bone Malformations. Pediatric Imaging.
Publisher | Google Scholor - Tsai PY, Chang C.H, Yu C.H, Cheng Y.C, Chang F.M. (2009). Thanatophoric Dysplasia: Role of 3-Dimensional Sonography. J Clin Ultrasound. 37(1):31-34.
Publisher | Google Scholor - Robert Y, Guérin du Masgenêt B, Ardaens Y. (2003). Ultrasound in Obstetric Practice. Paris: Masson.
Publisher | Google Scholor - Miller E, Blaser S, Shannon P, Widjaja E. (2009). Brain and Bone Abnormalities of Thanatophoric Dwarfism. AJR. 192:48-51.
Publisher | Google Scholor











