

Research Article
Cerebellar Cognitive Affective Syndrome in Cerebellar Disorders: An Experience from Tertiary Care Centre
1Resident, Department of Neurology, Mahatma Gandhi Medical College and Hospital, Jaipur, Rajasthan, India.
Rajendra Kumar Sureka
2Emeritus Professor, Department of Neurology, Mahatma Gandhi Medical College and Hospital, Jaipur, Rajasthan India.
Amit Kumar Agarwal
3Professor, Department of Neurology, Mahatma Gandhi Medical College and Hospital, Jaipur, Rajasthan India
*Corresponding Author: Himanshu kaushal
Citation: Kaushal H, Sureka RK, Agarwal A.K. (2024). Cerebellar Cognitive Affective Syndrome in Cerebellar Disorders: An Experience from Tertiary Care Centre. Journal of Neuroscience and Neurological Research. BioRes Scientia Publishers. 1(1):1-8. DOI: 10.59657/2837-4843.brs.24.019
Copyright: © 2024 Himanshu kaushal, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.2024 Himanshu kaushal, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and so
Received: May 18, 2024 | Accepted: June 01, 2024 | Published: June 10, 2024
Abstract
Introduction: Cerebellar cognitive affective syndrome is the syndrome of neurocognitive symptoms and signs including executive function, linguistic processing, spatial cognition, and affect regulation with or without motor and/or balance symptoms.
Methods: A cross sectional study conducted in the Department of Neurology in a tertiary care hospital in North-east Rajasthan in Indian subcontinent. 30 patients with cerebellar symptoms were recruited in the study.
Inclusion Criteria: Patients with cerebellar symptoms and signs with 1) age more than 18 years, 2) willing to participate.
Exclusion criteria: Patients with other causes of cerebellar dysfunction including hepatic and renal failure, dyselectrolytemia, thyroid disorder etc. were excluded from the study. Those patients who could not give consent due to cognitive impairment the consent of primary caregiver with age more than 18 years was taken the cognitive functions were studied in the patients using the two assessment tools namely cerebellar cognitive affective syndrome scale (CCAS-S) and Mini Mental State Examination (MMSE) Scale.
Results: Amongst 30 total patients 21(70%) were males and 9 (30%) were females with mean age of 56.13 years. 20 (66.66%) out of 30 patients were illiterate whereas 10 (33.33%) received formal education. Out of 30 patients, 11 patients had vascular events (9 infarcts, 2 hemorrhage), 8 had ataxia (7 SCA, 1 FA), 6 had drug induced cerebellar signs (4 phenytoin, 1 lithium, 1 carbamazepine), 3 MSA-C, 2 alcohol induced cerebellar degeneration. No, Mild and Major Cognitive Impairment was found in 10, 15 and 5 patients respectively on MMSE. According to the CCAS scale, almost all patients (n=28) were found to have definitive CCAS, 1 had probable CCAS and 1 had no CCAS. When CCAS Scale was applied, 28 out of 30 (93.33%) patients failed in “semantic fluency task” whereas 27 out of 30 (90%) failed in “phonemic fluency task”. “Category switching” was impaired in 28 out of 30 patients (93.33%). When attention was assessed by “Digit span forward” and “Digit span backward” tests 26 (86.66%) and 28 (93.33%) failed in these tasks. Verbal registration and recall were impaired in 21 (70%) and 24 (80%) patients. When patients were asked to draw a cube or asked to copy the cube patients if not able to draw on their own, 22 patients out of 30 patients (73.33%) failed to do so. Examination of affect revealed that 20 out of 30 patients had “difficulty with focusing attention or mental flexibility” and 18 patients had blunted affect. No patient had shown avoidant behavior or aggressive, irritable, oppositional behavior or difficulty with social boundaries
Conclusion: Cerebellar Cognitive Affective Syndrome is relatively an underreported and underdiagnosed entity. CCAS-S is better scale for cognitive functions screening as compared to MMSE in patients with cerebellar syndromes.
Keywords: cerebellar cognitive affective syndrome; cerebellum; cerebellar disorders; schmahmman and sherman syndrome;, cerebellar cognitive affective syndrome scale; mini mental state examination scale
Introduction
Cerebellum is one of vital areas of brain which is predominantly involved in the motor control and balance. Besides its role in coordination, balance and motor functions, there is emerging evidence of cerebellum also being involved in the neurocognitive functioning. Literature suggests that there are dense interconnections seen in cerebellum and cerebral hemispheres [1]. These interconnections are thought to play a major role in neurocognitive functioning as well as motor control and balance. The major neurocognitive domains that are influenced by cerebellum are language, memory and executive function which were once thought to be controlled only by cerebral cortical areas. With discovery of the various functional connections between the cerebellum and cerebrum with advent of functional imaging, there arise an important question of non-motor functions and symptoms which can arise in various cerebellar disorders. Moreover, cerebellum is involved in overall functional adaption of motor and non-motor activities. The role of cerebellum in these aforementioned domains is dynamic and it is given the name of “supervised learning machine”. The areas of cerebellum responsible for this neurocognitive functioning are termed as “Cognitive cerebellum” which includes the neocerebellum and major cerebello-cerebral connections [2]. Disorders of cerebellum that can cause neurocognitive, motor signs and incoordination are classified into two categories: One with “Pure cerebellar” involvement and others ones are “Cerebellar-plus syndromes” characterized by involvement of one or more areas of nervous system along with cerebellar features. The disorders of cerebellum can present as cerebellar cognitive affective syndrome (CCAS) which occurs in isolation or in combination with motor and incoordination symptoms. It was first described by Schmahmann and Sherman in 1998 hence the name “Schmahmman and Sherman syndrome” [3]. There is lack of studies assessing CCAS in patients with cerebellar disorders and there is equal lack of awareness regarding CCAS scale being used as better screening tool for CCAS. Hence, the present was done with aim to assess the features of CCAS in patients presenting with various cerebellar pathologies and compare the standard easy to use screening tool Mini Mental State Examination (MMSE) with CCAS scale.
Methods
The present study was a cross sectional study conducted in the Department of Neurology in a tertiary care hospital in North-east Rajasthan in Indian subcontinent after approval from Institutional ethics committee. 30 patients with cerebellar symptoms were recruited in the study from both the out-patient and in-patient department using non-probability simple consecutive sampling method.
Inclusion Criteria: Patients with
1) age of or more than 18 years as the Department of Neurology in the institute deals with Adult Neurology and patients less than 18 years are dealt by Pediatric Neurology Department.
2) willing to participate in the study after giving written informed consent and
3) cerebellar symptoms and signs (unsteadiness, incoordination, past pointing, action tremors, nystagmus, cerebellar dysarthria etc. with or without other features) were included in the study.
Exclusion criteria: Patients who were
1) less than 18 years of age
2) cerebellar features were initially present but the condition was severe enough or altered mental status in the form of delirium, stupor, comatose state which hampered testing and
3) those who did not give written informed consent to participate in the study were excluded from the study. Patients with other causes of cerebellar dysfunction including hepatic and renal failure, dyselectrolytemia, thyroid disorder etc. were excluded from the study. Those patients who could not give consent due to cognitive impairment the consent of primary caregiver with age more than 18 years was taken. The sociodemographic profile, laboratory investigations, clinical diagnosis, aetiology and radiological features were studied in the patient population. The cognitive functions were studied in the patients using the two assessment tools and the results of the two scales were compared as a part of secondary objectives of the study
Assessment tools: The cognitive functions of these patients were assessed using cerebellar cognitive affective syndrome scale (CCAS-S) and Mini Mental State Examination (MMSE) Scale.
CCAS-S: This scale is a 10-item battery to assess cerebellar cognitive functions. The components of scale are: semantic fluency, phonemic fluency, category switching, verbal registration, digit span forward, digit span backward, cube draw and cube copy, delayed verbal recall, similarities, go/no-go, and assessment of neuropsychiatric domains. Each domain has a cut off score on the basis of which the person is labelled pass or fail in that particular domain testing. Generally, it takes less than<10>
Results
Amongst 30 total patients 21(70%) were males and 9 (30%) were females. The age of patients ranged from 20 to 79 years with mean age of 56.13 years. 20 (66.66%) out of 30 patients were illiterate whereas 10 (33.33%) received formal education (4 graduate, 2 post graduate, 2 primary education, 2 senior secondary). 12 patients in the study were hypertensive, 6 were diabetic, 2 prediabetic, 1 pulmonary tuberculosis, 3 coronary artery diseases. Out of 30 patients, 11 patients had vascular events (9 infarcts, 2 hemorrhage), 8 had ataxia (7 SCA, 1 FA), 6 had drug induced cerebellar signs (4 phenytoin, 1 lithium, 1 carbamazepine), 3 MSA-C, 2 alcohol induced cerebellar degeneration. Median MMSE Score was 24(Range 15-28). No, Mild and Major Cognitive Impairment was found in 10, 15 and 5 patients respectively. Cerebral Cognitive Affective Syndrome was diagnosed in patients with these cerebellar pathologies using CCAS Scale. Median score at CCAS was 36 (Range 5-101). According to the CCAS scale, almost all patients (n=28) were found to have definitive CCAS, 1 had probable CCAS and 1 had no CCAS. When the mean MMSE scores were compared amongst various subgroups the median MMSE score in stroke subgroup was 24 as compared to 27 in non-stroke group which were comparable to each other. In contrast, the neurodegenerative subgroup comprising MSA-C, FA and SCA, the median MMSE score was 27 and in toxic/drug toxicity group it was found to be26. Amongst the neurodegenerative subcategory MSA-C patients had a median MMSE of 27 whereas the score was 27 in SCA and FA combined. Similarly, the mean CCAS Score was calculated and comparison was done amongst various subgroups and subcategories. Median CCAS score in stroke subgroup was 36 as compared to 32 in non-stroke group which were non comparable to each other unlike median MMSE. In contrast, the neurodegenerative subgroup comprising MSA-C, FA and SCA, the median CCAS score was and in toxic/drug toxicity group it was found to be 32. Amongst the neurodegenerative subcategory MSA-C patients had a median CCAS of 40 whereas the score was 32 in SCA and FA combined. Using CCAS Scale more patients were found to have cognitive impairment in contrast to routinely used MMSE scale (Table 1).
Table 1: Descriptive statistics of the study
| Characteristics | Number of patients, n (%) |
| Total number of patients | 30 (100%) |
| Males | 21 (70.00%) |
| Females | 9 (30.00%) |
| Mean Age (Range) | 56.13 Years (Range: 20 to 79) |
| Illiterate | 20 (66.66%) |
| Literate | 10 (33.33%) |
| Primary education | 2 (6.66%) |
| Senior secondary | 2 (6.66%) |
| Graduate | 4 (13.33%) |
| Postgraduate | 2 (6.66%) |
| Comorbidities | |
| Hypertensive | 12 (40.00%) |
| Diabetes Mellitus | 6 (20.00%) |
| Prediabetic | 2 (6.66%) |
| Pulmonary Tuberculosis | 1 (3.33%) |
| Coronary artery disease | 3 (10.00%) |
| Cerebellar lesions: | n=30 |
| Pure cerebellar | 11 (36.66%) |
| Complex cerebellar/ cerebellar plus | 19 (63.33%) |
| Etiological classification: | |
| Vascular events: | n=11 |
| Ischemic infarct (unilateral/bilateral) | 9 (81.81%) |
| Haemorrhage (unilateral/bilateral) | 2 (18.18%) |
| Ataxias: | n=8 |
| SCA | 7 (87.50%) |
| FA | 1 (12.50%) |
| Drug/Toxins | n=8 |
| Alcohol induced cerebellar degeneration | 2 (25.00%) |
| Drug induced cerebellar toxicity | 6 (75.00%) |
| MSA-C | n=3 |
| Mean MMSE Score: 24 (Range 15-28) | n=30 |
| No Cognitive Impairment | 10 (33.33%) |
| Mild Cognitive Impairment | 15 (50.00%) |
| Major Cognitive Impairment | 5 (16.66%) |
| Mean CCAS Score: 36 (Range 5-101) | n=30 |
| Possible CCAS | 1 (3.33%) |
| Probable CCAS | 1 (3.33%) |
| Definitive CCAS | 28 (93.33%) |
When CCAS Scale was applied (results shown in Table 2.), 28 out of 30 (93.33%) patients failed in “semantic fluency task” whereas 27 out of 30 (90%) failed in “phonemic fluency task”. “Category switching” was impaired in 28 out of 30 patients (93.33%). When attention was assessed by “Digit span forward” and “Digit span backward” tests 26 (86.66%) and 28 (93.33%) failed in these tasks. Verbal registration and recall were impaired in 21 (70%) and 24 (80%) patients. When patients were asked to draw a cube or asked to copy the cube patients if not able to draw on their own, 22 patients out of 30 patients (73.33%) failed to do so. Figure 1. shows the cubes drawn by the patients spontaneously and Figure 2. shows cubes copied on showing the reference cube (Figure 3.). Examination of affect revealed that 20 out of 30 patients had “difficulty with focusing attention or mental flexibility” and 18 patients had blunted affect. No patient had shown avoidant behavior or aggressive, irritable, oppositional behavior or difficulty with social boundaries.
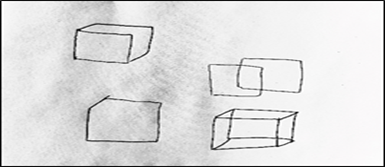
Figure 1
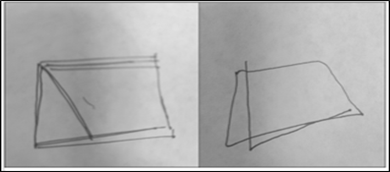
Figure 2
Figure 3
Figure 1 (Left) shows the spontaneous cube drawing task and cube copying (Figure 2., Right) task performed by the patients and Figure 3. (Middle, Lower) shows the normal cube structure shown to the patients for copying or reference.
Table 2: Results of CCAS Scale
| CCAS Scale Component | Median score | Number of patients Failed to do | Percentage |
| SEMANTIC FLUENCY | 3 | 28 | 93.33% |
| PHONEMIC FLUENCY | 4 | 27 | 90% |
| CATEGORY SWITCHING | 4 | 28 | 93.33% |
| VERBAL REGISTRATION | -NA- | 21 | 70% |
| DIGIT SPAN FORWARD | 3 | 26 | 86.66% |
| DIGIT SPAN BACKWARD | 1 | 28 | 93.33% |
| CUBE (DRAW) | 10 | 22 | 73.33% |
| CUBE (COPY) | 10 | 22 | 73.33% |
| VERBAL RECALL | 1 | 24 | 80% |
| SIMILARITIES | 3 | 30 | 100% |
| GO NO-GO | 1 | 11 | 36.66% |
The laboratory investigations are summarized in table 3.
Table 3: Laboratory Investigation of patients with cerebellar lesions
| INVESTIGATION | MEAN VALUE |
| TOTAL LEUCOCYTE COUNT (cells/uL) | 9130.68 |
| HEMOGLOBIN (g/dL) | 11.09 |
| PLATELET COUNT (cells/uL) | 276142.9 |
| SODIUM (meq/ml) | 138.38 |
| POTASSIUM (meq/ml) | 4.11 |
| CHLORIDE (meq/ml) | 102.03 |
| CALCIUM (mg/dL) | 8.38 |
| BLOOD UREA (mg/dL) | 50.17 |
| SERUM CREATININE (mg/dL) | 1.36 |
| SGOT | 41.3 |
| SGPT | 40.28 |
| T3 | 1.01 |
| T4 | 8.39 |
| TSH | 0.94 |
| VITAMIN B12 | 293.46 |
| Random Blood Sugar (RBS) | 118.65 |
| HBA1C | 6.45 |
6 patients with drug induced cerebellar syndrome had reversible Cerebral cognitive affective syndrome that improved after stopping the drug. There was overall improvement in MMSE and CCAS scores after the patients recovered from illness. The average time taken was 7.8 days with average improvement by a score of 6.4 points in MMSE and 22.9 points in CCAS. Family history was positive in preceding 2 generations and 1st degree relatives in 4/7 SCA patients whereas 3/7 couldn’t provide relevant history.
- Patients with MSA-C had associated signs of autonomic dysfunction in the form of positive orthostatic fall in blood pressure, hand grip test and R-R variability test.
Discussion
In the present study, a total of 30 patients were studied with a male preponderance of 70% (n=21). The average age in our study was 56.13 years with a range of 20 to 79 years. In study by Schachman and Sherman in 1998, 12 out of 20 patients studied were males [4]. Higher reporting of symptoms by males and early recognition of symptoms in male group and ignorance towards females’ health can be the cause of such a difference. Otherwise irrespective of gender (except few cerebellar ataxias with female predominance or specific male gender predilection for e.g. Friedrich ataxia) the features of cerebellar involvement are same. In a study by Hoche F et al. in 2018 where Seventy-seven patients were included in the study with age between 17–80 years and male preponderance was seen (42 out of 77 patients). mean education 15.01 years) were included in the study, of whom 36 had disease confined to cerebellum [5]. 10 out of 30 received formal education. The mean years of education were years 16.77 years (total of 9 patient who received formal education). This was in comparison to 15.65 years as found by Hoche F et al in their study. Random sampling for cerebellar disorders yielded a number of 11 patients with vascular events (9 infarcts, 2 hemorrhage), 8 with ataxia (7 SCA, 1 FA), 6 with drug induced cerebellar signs (4 phenytoin, 1 lithium, 1 carbamazepine), 3 with MSA-C, 2 with alcohol induced cerebellar degeneration. Hoche F et al. in their study of 77 patients, patients were classified as isolated cerebellar pathology and complex cerebrocerebellar pathology. Number of patients with isolated cerebellar pathology and complex cerebrocerebellar pathology were 36 and 41 respectively. Previous studies did not describe these sub-categories under various subcategories like vascular lesions including stroke and non-vascular lesions like neurodegenerative, drugs toxicities, infections etc. which was in contrast to the present study as in the latter an attempt was made to compare the subcategories. Moreover, an attempt was made to compare the CCAS scores and MMSE score in different sub groups including stroke and non-stroke groups, stroke and neurodegenerative group, toxic/metabolic and stroke sub-groups. Lastly the scores were also compared in between MSA and SCA groups which was unique to this study. The median score of CCAS scale was 36 among stall the patients. All patients performed poorly on CCAS contributing to 100% cognitive affection with 28 (93.33%) patients were found to have definitive CCAS whereas only 1 (3.33%) each were found to have probable and possible CCAS. On MMSE scale, only 9 (30%) patients were found to have a cognitive decline. The median MMSE score was found to be 24 in our study.
The mean CCAS score in stroke was 36 which was lower as compared to the neurodegenerative group, toxic/metabolic group where it was found to be 32respectively. The reason for higher score in this group could be attributed to damage caused by vascular events at a point of time whereas in other groups it is cumulative effect over time leading to gradual affection of cognitive functions. The findings are in coherence with study conducted by Naeije et al. [6], Maas et al. [7], Chirino-Pérez et al. [8], Benussi et al. [9] and Chirino-Pérez et al. [8] where the total failed tests as well as raw score of CCAS were seen in patients with chronic or neurodegenerative cerebellar pathology where the cumulative effect caused worsened score as compared to acute lesions. Amongst stroke patients as concluded by Abderrakib A and colleagues, patients with right sided lesions were found to have worse scores and poorer outcome. [10] In the current study all patients (n=30) failed in “Similarities task” done in CCAS followed by “Semantic fluency task”, “Category Switching task” and “Digit Span Backward task” in which 93.33% (n=28) failed. 90% patients failed in “Phonemic Fluency task” whereas 86.66% and 80% patients failed in “Digit Span Forward task” and “Verbal recall task” respectively. 73.33% and 70
Conclusion
CCAS is highly underdiagnosed and underreported conditionIt has various etiologies namely reversible and irreversible. CCAS is spectrum of cognitive deficits seen in cerebellar lesions with or without the motor or balance symptoms. While assessing cognitive impairment in patients with cerebellar lesions, it can be inferred that the routinely administered screening MMSE scale can underrate the patients of CCAS because it is generally normal or shows mild cognitive impairment CCAS scale on the other hand has yield for diagnosis of Cerebellar Cognitive Affective Syndrome. However, large scale multicentric study is required to assess the comparison.
References
- Strick PL, Dum RP, Fiez JA. (2009). Cerebellum and nonmotor function. Annu Rev Neurosci, 32:413-434.
Publisher | Google Scholor - Habas C (2021) Functional Connectivity of the Cognitive Cerebellum.Front. Syst. Neurosci. 15:642225.
Publisher | Google Scholor - Manto M, Mariën P. (2015). Schmahmann’s syndrome - identification of the third cornerstone of clinical ataxiology. Cerebellum Ataxias, 27; 2:2.
Publisher | Google Scholor - Schmahmann JD & Sherman JC. (1998). The cerebellar cognitive affective syndrome. Brain: A Journal of Neurology, 121(4):561-579.
Publisher | Google Scholor - Hoche F, Guell X and Vangel MG et al. (2018). The cerebellar cognitive affective/Schmahmann syndrome scale.Brain: A Journal of Neurology, 141(1):248–270.
Publisher | Google Scholor - Naeije G, Rai M, Allaerts N, Sjogard M, De Tiège X, Pandolfo M. (2020). Cerebellar cognitive disorder parallels cerebellar motor symptoms in Friedreich ataxia. Ann Clin Transl Neurol, 7:1050-1054.
Publisher | Google Scholor - Maas RPPWM, Killaars S, van de Warrenburg BPC, Schutter DJLG. (2021). The cerebellar cognitive affective syndrome scale reveals early neuropsychological deficits in SCA3 patients. J Neurol, 268:3456–3466.
Publisher | Google Scholor - Chirino-Pérez A, Marrufo-Meléndez OR, Muñoz-López JI, Hernandez-Castillo CR, Ramirez-Garcia G, Díaz R, et al. (2021). Mapping the cerebellar cognitive affective syndrome in patients with chronic cerebellar. Strokes,21:208–218.
Publisher | Google Scholor - Benussi A, Koch G, Cotelli M, Padovani A, Borroni B. Cerebellar transcranial direct current stimulation in patients with ataxia: a double-blind, randomized, sham-controlled study. Mov Disord. (2015) 30:1701-1705.
Publisher | Google Scholor - Abderrakib A, Ligot N and Naeije G (2022). Cerebellar cognitive affective syndrome after acute cerebellar stroke. Front. Neurol,13:906293.
Publisher | Google Scholor - Konczak J, Timmann D. (2007). The effect of damage to the cerebellum on sensorimotor and cognitive function in children and adolescents. Neurosci Biobehav Rev, 31:110-113
Publisher | Google Scholor - Murdoch BE. (2010). The cerebellum and language: historical perspective and review. Cortex, 46:858–868.
Publisher | Google Scholor - Wang D, Buckner RL, Liu H. (2013). Cerebellar asymmetry and its relation to cerebral asymmetry estimated by intrinsic functional connectivity. J Neurophysiol, 109:46–57
Publisher | Google Scholor














