

Case Report
Case Report of Young Female with Anomalous Origin of RCA from Left Coronary Cusp Repaired with Rima to RCA and Its Proximal Ligation
- Yasser Mubarak MD 1*
Professor of cardiothoracic surgery department, Faculty of Medicine, Minia University, Egypt. Medina cardiac center, AL Medina Al Munawarra, Saudi Arabia. King Fahad Medical City, King Salman Heart Center, Riyadh, Saudi Arabia.
*Corresponding Author: Yasser Mubarak MD
Citation: Mubarak Y. (2023). Case Report of Young Female with Anomalous Origin of RCA from Left Coronary Cusp Repaired with RIMA to RCA and its Proximal Ligation, Journal of Clinical Cardiology and Cardiology Research, BioRes Scientia Publishers. 2(2); DOI: 10.59657/2837-4673.brs.23.014.
Copyright: © 2023 Yasser Mubarak, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 11, 2023 | Accepted: September 29, 2023 | Published: October 05, 2023
Abstract
Coronary artery anomalies (CAA) include a rare condition characterized by an abnormality in the course or origin of any of the three main coronary arteries (right coronary artery, left coronary artery, and left anterior descending artery). [1] CAA are found in <1% of general population. Anomalous origin of the right coronary artery (ARCA) from the left sinus of Valsalva represents less than 3% of the congenital coronary anomalies and 0.1% of patients undergoing angiography.
Keywords: coronary artery anomaly; anomalous right coronary artery; coronary artery bypass grafting; right internal mammary artery
Introduction
Coronary artery anomalies (CAA) include a rare condition characterized by an abnormality in the course or origin of any of the three main coronary arteries (right coronary artery, left coronary artery, and left anterior descending artery). [1] CAA are found in <1>
Although, most of CAA are asymptomatic, about 20% produce symptoms like; arrhythmias, syncope, myocardial infarction (MI), or sudden cardiac death (SCD). The mechanism of SCD in these patients is thought to be due to myocardial ischemia occurring during physical exertion and resultant arrhythmia. So, it can be fatal if it remains undiscovered. Variable surgical techniques have been used, including coronary reimplantation, unroofing the intramural segment, and coronary artery bypass grafting (CABG). CABG eliminates the need to open the aorta, but subjects the patient to graft thrombosis due to competitive flow. So, ligation of the proximal coronary is recommended to prevent competitive flow [2].
The American College of Cardiology (ACC) and the American Heart Association (AHA) advised a class IIb recommendation for repairing an asymptomatic anomalous right or left coronary artery from the contralateral coronary sinus that follows an intra-arterial course. [3] Anomalous coronary arteries can be surgically corrected by CABG, re-implantation of the artery to its proper coronary sinus, or by an unroofing procedure [4].
Case Presentation
20-years female who is known to have chronic complaint of cardiac chest pain with exertion since childhood. She had Computed Tomographic Angiography (CTA) of the coronaries then Positron Emission Tomography (PET) stress study in another facility. CTA showed anomalous origin of the RCA from the left coronary sinus, and anomalous course between aorta and pulmonary artery. Figure (1) Positron Emissions Tomography–Computed Tomography (PET–CT) showed stress-induced ischemia of the myocardium supplied by RCA. She advised to undergo surgical intervention and she agreed. Preoperative transthoracic echocardiography (TTE) was normal. She underwent on pump coronary artery bypass grafting (CABG) skeletonized right internal mammary artery (RIMA) to RCA with proximal ligation of ARCA. Intra-operative trans-esophageal echocardiography (TEE) revealed normal left ventricular ejection fraction (LVEF) of 55-60%, and no valvular abnormalities. She extubated fast track at intensive care unit (ICU). She discharges on 5th postoperative day (POD) with uneventful course. She was seen in follow up outpatient clinic (OPD) 2 weeks after discharge, when she was recovering well and reported no recurrence of symptoms 1year duration.
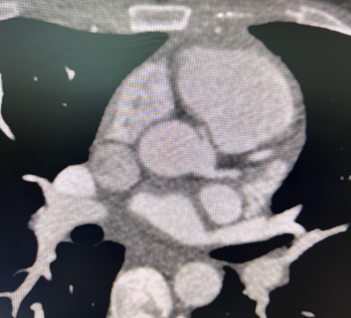
Figure 1: CTA showing ARCA from LCC
Discussion
Coronary artery anomalies (CAA) have been associated with a wide range of clinical manifestations. Anomalous RCA (ARCA) between the aorta and the pulmonary artery compressed by the increased cardiac output during exercise. It can increase risks of MI, arrhythmia, syncope, and SCD. Possible mechanisms of ischemia-induced SCD by the anomalous RCA from left coronary sinus have been suggested: mechanical compression of the RCA by the pulmonary artery and aorta during physical exertion [5].
ARCA is incidentally found more frequently than anomalous left coronary arteries. Three subtypes of anomalous RCA have been described: (1) a high inter-arterial course between the pulmonary artery and the aorta; (2) a low inter-arterial course between the right ventricular outflow tract and the aorta; and (3) a hypoplastic anomalous RCA orifice. Routine testing with resting or exercise electrocardiography (ECG) is not sufficiently sensitive to rule out this congenital anomaly. The diagnosis of anomalous coronary arteries can be made by the use of conventional coronary angiography or CT angiography, or cardiac magnetic resonance imaging (MRI). Both cardiac MRI and CT are becoming increasingly popular imaging modalities for detecting coronary anomalies [4].
In our case ARCA was diagnosed by CTA, and she was manifested with recurrent cardiac chest pain during exercise.
Up to one-third of SCD in the young population are caused by CAA, and especially an inter-arterial course, as suspected in this case, and early diagnosis is crucial. Clinical presentation of these patients ranges from asymptomatic to nonspecific cardiac chest pain, palpitations, dizziness, or syncope. While SCD is usually associated with young athletes, however, other clinical manifestations are frequently seen in older adults [3].
Different management strategies have been used, but recently the primary strategy has shifted from medical observation to surgical treatment, however still depending on the symptoms. Among the surgical techniques used are the bypass graft surgery, reimplantation of the coronary ostium, unroofing technique, and direct translocation of the pulmonary artery [5].
In our case, surgical correction was performed due to patient’s chest pain symptoms, malignant course of the ARCA, and evidence of external compression of the coronary artery. She was the youngest case for CABG was performed.
Conclusion
Coronary artery bypass grafting for anomalous origin of right coronary artery from left coronary cusp is safe procedure and prevent sudden cardiac death.
Declarations
Conflict of interest: No conflicts to declare.
Funding: No funding was received for this study.
Ethical approval: The study was approved by adult cardiac surgery department.
Consent
Informed consent was obtained from the patient for publication of this case report and accompanying images.
References
- Pramukh A, Boskey P, Mahati D, Pradnya B, Sushmita P, et al. (2023). Anomalous aortic origin of right coronary artery from left coronary cusp: a management conundrum: a case report. Journal of Medical Case Reports. 17(191).
Publisher | Google Scholor - Sai V, Abhishek B, Neeta S, Gregory B. (2021). Complex Clinical Cases. J Am Coll Cardiol. 2371
Publisher | Google Scholor - Malik M J, Seibolt L. (2022). Anomalous Origin of the Right Coronary Artery From the Left Coronary Cusp Presenting as a Non-ST-Elevation Myocardial Infarction (NSTEMI). Cureus. e30839.
Publisher | Google Scholor - Brian G, Adriana Q, Monvadi S, Sripal B, Robert R. (2012). Anomalous Right Coronary Artery and Sudden Cardiac Death. Circulation: Arrhythmia and Electrophysiology. 111–12.
Publisher | Google Scholor - Nha H, Ronald R, Paul B, Jon G. (2015). Anomalous Right Coronary Artery From Left Coronary Cusp With Inter-Arterial Course: Evaluation and Management. Cath lab digest. 23(8).
Publisher | Google Scholor










