

Case Report
Case Report of Delayed Treatment of Lepromatous Leprosy Masquerading as Acne Vulgaris in Post Elimination Era in Nepal
- Latika Giri *
- Suyash Acharya
- Niroj Bhandari
- Grishma Sharma
- Prabesh Gautam
Kathmandu University School of Medical, Sciences, Dhulikhel, Nepal.
*Corresponding Author: Latika Giri, Kathmandu University School of Medical, Sciences, Dhulikhel, Nepal.
Citation: Giri L, Acharya S, Bhandari N, Sharma G, Gautam P. (2023). Case Report of Delayed Treatment of Lepromatous Leprosy Masquerading as Acne Vulgaris in Post Elimination Era in Nepal. Dermatology Research and Reports, BRS publishers. 2(1); DOI: 10.59657/2993-1118.brs.23.005
Copyright: © 2023 Latika Giri, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 12, 2023 | Accepted: June 30, 2023 | Published: July 04, 2023
Abstract
Leprosy affects multiple systems and causes morbidity. However, with attainment of global elimination, and prevalence being 0.89/10000 at national level in Nepal; it is seldom considered a diagnosis when it doesn't manifest telltale signs. Leprosy can masquerade various dermatological, orthopedic or neurological problems thus delaying the diagnosis.
Keywords: general dermatology; leprosy; acne; infection
Introduction
Mycobacterium lepromatosis is one of the oldest recorded diseases to mankind prevalent even in biblical texts. In recent times multi-drug therapy (MDT) usage has eliminated this disease as a public health problem from the western world but the disease is still endemic to low resource settings in Asia, Africa and South American regions [2]. The disease is due to infection of Mycobacterium leprae, producing chronic infection; majorly but not limited to skin, nerves and reticuloendothelial system [3,4]. The disease can also affect upper respiratory tract, bones, joints, eyes, testes and adrenal glands [4]. Clinical spectrum of leprosy ranges from “paucibacillary” tuberculoid leprosy to “multibacillary” lepromatous leprosy depending on the immune response of the host [5,6]. The common clinical findings are hypo pigmented or erythematous patches which has partial or complete loss of sensation [4].
Case Presentation
We present a case of 20 years old female from the Hilly terrain of Nepal who presented to out -patient department of an outreach center of Dhulikhel Hospital on mid-May, 2021. She presented with chief complaints of acne like lesions (maculopapular lesions, pustules and later nodules) on face since 2 years which gradually progressed to back, and flexor surface of lower limbs bilaterally (Figure 1, 2, 3). The lesions first noted on her face were comedones, papules,pustules and gradually developed to nodules on face, back and flexor surface of lower limbs. Her past medical history was uneventful and she had neither significant family history nor contact history with Tuberculosis patients, Leprosy or Sexually Transmitted Infections (STDs). There was no history of weight loss, loss of appetite, hair fall, loss of eyebrows, loss of sensation, hypo pigmented areas, thickening of nerves, loss of motor function, lethargy or arthritis. She had been using Topical Retinoic Acid Gel 0.25% on face for acne, based on advice from friends along with topical application of Herbs from traditional healers for 2 years prior to consultation in our hospital. There was no use of antibiotics or any other medication. She was born in hilly district of Nepal, had no travel outside of home district, student by occupation, had exposure to cattle reared at home.

Figure 1: Multiple hyperpigmented macules, nodules and ulcerated lesions in different stages of healing.

Figure 2: Hyperpigmented patch and multiple nodules on back.
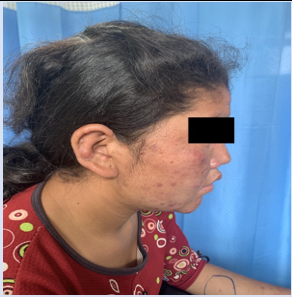
Figure 3: Acne like nodules on fase.
On examination, she was afebrile, her general condition was fair. There were multiple maculopapular lesions, pustules, nodules, face, lower back and lower part of lower extremities. Perineal lesions were absent. Lymphadenopathy was not present, and there was no organomegaly. Routine tests CBC (complete blood count), LFT, RFT, UREME, total count, Culture of sputum, Mantoux tests were sent which all yielded normal results. However ESR was raised and differential count showed lymphocyte predominance. Serology (HbSAg, HIV, VDRL) was non-reactive and chest radiograph was also within normal limits. Laboratory markers are presented in the table (Table 1).
| Laboratory parameter | Value | Reference Range |
| Total WBC Count | 9200/cumm | 4000-11000 |
| Hemoglobin | 12.2 gm/dL | 11-15 |
Differential Count Neutrophil Lymphocyte Eosinophil Monocyte Basophil |
38 55 02 05 00 |
% % % % % |
| Platelet count | 155000/cumm | 150000-450000 |
Prothrombin Time (PT) PT Control INR |
15 sec 13.5 sec 1.1 |
10-15 13 |
| Glucose, Random (Serum) | 115.1 mg/dL | 80-140 |
Liver Function Test (LFT) Bilirubin, Total Bilirubin, Direct SGOT (AST) SGPT(ALT) |
0.6 mg/dL 0.3 mg/dL 27.1 IU/L 17.0 U/L |
0.20-1 0.00-0.50 <40> <40> |
Renal Function Test (RFT) Urea, serum Creatinine, serum Sodium, serum Potassium, serum |
43 mg/dL 0.53 mg/dL 139 mmol/L 4.2 mmol/L |
15-50 0.40-1.40 135-155 3.50-5.50 |
| ESR | 50 mm/hr | 0-25 mm/hr |
Thyroid Function Test (TFT) fT3 fT4 TSH |
3.18 pg/ml 1.21 ng/dl 0.52 mIU/L |
2.77-5.27 pg/ml 0.78-2.19 ng/dL 0.46-4.68 mIU/L |
| C- reactive protein | 0.6mg/dl | 0.3-1 mg/dl |
On history taking retrospectively from the past 2 years, treatment with Topical Retinoic Acid Gel 0.25% with application of herbal pastes had shown no improvement and there was gradual spread of lesions. The presenting findings were suggestive of Acne Vulgaris, Cutaneous Tuberculosis, Leprosy, Sarcoidosis, SLE, Granuloma Annulare, fungal infection.
Patient was offered Excisional biopsy of skin lesions for HPE which showed Lepromatous Leprosy.
Skin biopsy specimen consisted of single piece of skin covered tissue measuring 0.3 cm. Entire specimen was submitted in two sections. Sections showed orthokeratotic epidermis with basal layer with melanin pigmentation. Subepithelially, band of collagen fibres forming Grenz zone were seen (Figure 4). Underlying dermis showed lymphohistiocytotic clusters with dense perivascular and periadnexal lymphocytic infiltrations with neural tissue destruction (Figure 5). Granuloma was not seen. Stain for AFB Leprae was positive (Figure 6). Bacillary Index was 3 (1 to 10 per HPF)
Leprosy though eliminated is fairly common in this part of the world hence in view of this patient was referred to Anandaban Hospital which is a national center where state of the art treatment is provided free of cost to patients.
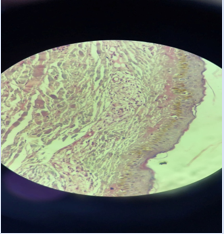
Figure 4: Grenz zone and Foamy macrophages.
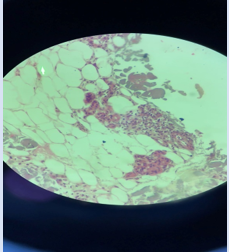
Figure 5: Perivascular inflammation with lymphocytic infiltrates.
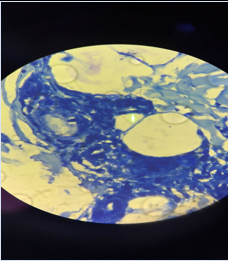
Figure 6: Arrow showing Lepra bacilli.
In Anandaban Hospital, detailed history was taken and examination was done. Contact and Family history were ruled out. Repeat biopsy was taken which showed features consistent with Lepromatous Leprosy. On examination multiple lesions were found on face, back, legs, however other telltale signs of Leprosy such as hypochromic anesthetic skin patches, thickening of nerve, loss of sensation, loss of motor function, amputation of limbs or nasal septum, loss of eyebrows, clawing, visible deformities were absent. A large number of acid-fast bacilli were present in the slit skin smears (BI: 3+) taken from left lower limb. Patient was diagnosed and confirmed as a case of Lepromatous Leprosy with BI 3+ based on HPE report of skin.
She was given Multibacillary Multidrug therapy which consists of the following regimen:Rifampicin 600 mg PO once a month, Dapsone 100 mg PO once a day, Clofazimine 300 mg PO once a month and Clofazimine 50 mg PO once a day for 12 months. She is doing well and responding well to the treatment with visible decrement of nodules on face and limbs. There has been no intolerance to medications provided in course of the treatment. Initiation of treatment was delayed by two years due to delay in seeking an alternative, suitable diagnosis for the patient.
Discussion
Leprosy is classically characterized by hypo pigmented or erythematous skin lesions with loss of sensation with or without peripheral nerve thickening [7]. Along with increasing prevalence of Leprosy in the post elimination era, various atypical presentations have been recorded [8].
The diagnosis of leprosy when it presents as acne vulgaris without the telltale features in skin or nerve involvement is often difficult and remains a diagnostic challenge often inundating physicians. It is because in the post elimination era, leprosy as a differential doesn't strike physicians easily due to significantly decreased incidence [9]. Our patient presented with acne-like lesions (maculopapularlesions, pustules and nodules) on the face which later progressed to different parts of the body. Though papules have been a common presentation, progression of lesions to pustules and nodules has rarely been witnessed.
Leprosy rarely presents with singular manifestation of skin lesions only [10]. The skin lesions when present are in the form of papules but rarely comedones, papules progressing to nodules [11].
Acne vulgaris is common in teenagers, and incidence has been noted in every 9 out of 10 adolescents [12]. The common presentation being comedones, papules, nodules on face, back and patient being a young female with above features in absence of any other appreciable systemic features acne vulgaris was considered as diagnosis of inclusion. Skin biopsy of acne vulgaris presents with dilated follicle with keratin plug, in advanced cases dilated follicle with open comedone may be seen, with signs of inflammation, presence of bacteria when follicle ruptures along with fibrosis and scarring [13].
Most adolescents experiencing facial acne have responded to Local application of Retinoic Acid Gel as demonstrated by PERFECT trail however our patient did not respond [14]. Thus her workup was performed to rule out other dermatological conditions causes like Cutaneous Tuberculosis, SLE, Fungal or Bacterial Infections. This was done because of the fact that in the clinical setting, skin lesion of leprosy is often misdiagnosed as other dermatological conditions like erythematous plaque seen on leprosy may be labeled as tinea, psoriasis, lupus vulgaris etc. and hypopigmented patches are labeled as pityriasis alba, pityriasisversicolor, and vitiligo etc [15].
The pathogenesis behind such skin manifestations would be generation of inflammatory mediators like prostaglandins which were not suppressed with treatment in line with Acne vulgaris hence the patient didn’t show improvement [8].
In the reported case, some aspects drew our attention. Our patient was a young female with macules and comedones on the skin of face, without recognizable signs of neuropathy, which was non- contagious as family members weren’t affected by disease, and although she had prolonged disease period; with treatment disease was managed without irreversible disability involving eyes, hands and feet due to neuropathy.
Close contact with leprosy patients in elderly and age group 5-15 years, immunosuppressed individuals should be ruled out in skin lesions persisting for long periods, resistant to routine treatment even when neurological symptoms are lacking, skin biopsy must be obtained.
Conclusion
Leprosy mimics an army of various clinical manifestations, the presenting time ranging from months to years often mimicking a different diagnosis altogether. Though eliminated, it is an important differential to keep in mind while managing skin related disorders as it can get obscured by various skin conditions with more common incidence. To maintain elimination of leprosy physicians should not forget Leprosy and religiously consider it as a diagnosis in such a case and report and treat cases timely to decrease the burden of it in the community.
Acknowledgments
The authors would like to appreciate the cooperation of the patient and the patient's family for this paper.
Conflict of Interest
None
Author Contributions
Giri L is the corresponding author, who was involved in the patient examination and care, writing and editing manuscript.
Acharya S helped in writing and editing the manuscript.
Sharma G contributed to manuscript editing.
Bhandari N contributed to the literature review and manuscript revision.
Gautam P contributed to literature review.
Ethical Approval
No ethical limits were crossed during reporting of this article.
Consent
Informed written consent was given by the patient herself.
Conflicts of Interest: None declared.
Consent: Approved by patient.
Funding sources: None.
References
- Marahatta SB, Amatya R, Adhikari S, et al. (2018). Perceived stigma of leprosy among community members and health care providers in Lalitpur district of Nepal: A qualitative study. PLoS One, 13(12):0209676.
Publisher | Google Scholor - Joel Carlos Lastória MAMM de A. (2014). Leprosy: review of the epidemiological, clinical, and etiopathogenic aspects - Part 1. An Bras Dermatol, 89(2):205.
Publisher | Google Scholor - White C, Franco-Paredes C. (2015). Leprosy in the 21st century. Clin Microbiol Rev, 28(1):80-94.
Publisher | Google Scholor - Maymone MBC, Laughter M, Venkatesh S, et al. (2020). Leprosy: Clinical aspects and diagnostic techniques. J Am Acad Dermatol, 83(1):1-14.
Publisher | Google Scholor - Chimenos Küstner E, Pascual Cruz M, Pinol Dansis C, Vinals Iglesias H, Rodríguez de Rivera Campillo ME, López López J. (2006). Lepromatous leprosy: a review and case report. Med Oral Patol Oral Cir Bucal, 11(6):474-479.
Publisher | Google Scholor - Fischer M. (2017). Leprosy - an overview of clinical features, diagnosis, and treatment. J Dtsch Dermatol Ges, 15(8):801-827.
Publisher | Google Scholor - Bhat RM, Prakash C. (2012). Leprosy: an overview of pathophysiology. Interdiscip Perspect Infect Dis, 2012:181089.
Publisher | Google Scholor - Pathania V, Singh J, Sinha A, Kothari R, Baveja S, Shankar P. (2020). Are we witnessing a paradigm shift in leprosy: Two atypical presentations of histoid hansen’s disease. Int J Mycobacteriol, 9(1):103-106.
Publisher | Google Scholor - Gupta S, Li C, Thallapally VK, Sharma P, Nahas J. (2021). Chronic Hand Swelling and Dactylitis in Leprosy: A Case Report and Review of the Literature. Cureus, 13(2):13451.
Publisher | Google Scholor - Signs and Symptoms. Published October 22, 2018.
Publisher | Google Scholor - Eichelmann K, González González SE, Salas-Alanis JC, Ocampo-Candiani J. (2013). Leprosy. An update: definition, pathogenesis, classification, diagnosis, and treatment. Actas Dermosifiliogr, 104(7):554-563.
Publisher | Google Scholor - Lynn DD, Umari T, Dunnick CA, Dellavalle RP. (2016). The epidemiology of acne vulgaris in late adolescence. Adolesc Health Med Ther, 7:13.
Publisher | Google Scholor - Sutaria AH, Masood S, Schlessinger J. (2022). Acne Vulgaris. In: StatPearls [Internet]. StatPearls Publishing.
Publisher | Google Scholor - Blume-Peytavi U, Fowler J, Kemény L, et al. (2020). Long-term safety and efficacy of trifarotene 50 μg/g cream, a first-in-class RAR-γ selective topical retinoid, in patients with moderate facial and truncal acne. J Eur Acad Dermatol Venereol, 34(1).
Publisher | Google Scholor - Kumar B, Dogra S. (2009). Leprosy: a disease with diagnostic and management challenges! Indian J Dermatol Venereol Leprol, 75(2):111-115.
Publisher | Google Scholor - Boushab BM, Fall-Malick FZ, Basco LK. (2018). Two Cases of Delayed Diagnosis of Leprosy in Mauritania. Case Rep Dermatol Med, 2018:4394297.
Publisher | Google Scholor










