

Research Article
Breech Delivery at Term: Maternal and Fetal Prognosis: About 194 Cases
- Marwen Nadia *
- Kouloud Tarhouni
- Aidi Hadhemi
- Dinari Amrou
- Soui Slah
Obstetrics and Gynecology, Ibn El Jazzar University Hospital, Kairouan, Tunisia.
*Corresponding Author: Marwen Nadia, Obstetrics and Gynecology, Ibn El Jazzar University Hospital, Kairouan, Tunisia.
Citation: Nadia M, Kouloud T, Hadhemi A, Amrou D, Slah S. (2024). Breech Delivery at Term: Maternal and Fetal Prognosis: About 194 Cases, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 1(5):1-5. DOI: 10.59657/2997-6103.brs.24.027
Copyright: © 2024 Marwen Nadia, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 29, 2024 | Accepted: September 10, 2024 | Published: September 19, 2024
Abstract
Introduction: Breech presentation is the most common presentation after vertex presentation. It is considered as a dangerous presentation because of the attached higher rates of perinatal mortality and morbidity. The aim of this work was to study the different etiological factors, the elements of choice of the delivery route as well as the maternal and fetal prognosis of the delivery routes.
Material and Methods: A retrospective study was carried in the Gynecology and Obstetrics Department of Ibn Jazzer Hospital in Kairouan, including all cases of breech deliveries observed over a period of one year from January 1st 2023 to December 31, 2023.Twin pregnancies, fetal deaths in utero, preterm birth and medical interruption of pregnancy were excluded from this study.
Results: A total of 194 breech deliveries were included in our study. Overall, 53, 1% of the women were primiparous. The most frequently encountered variety was the left anterior sacro iliac (44.4%). Overall, 43, 3% vaginal deliveries and 56.7% caesarean sections were noted. A significant statistic relationship was found between the caesarean section and cervical dilatation of more than 4 cm (p = 0.0001), a low Bishop score (p = 0.0001), a biparietal diameter of more than 98 mm (p = 0.007). Only one case of obstetrical trauma was found.
Conclusion: this study shows that when the selection criteria are well respected and the monitoring of labour progress is rigorous, vaginal delivery does not constitute a significant excess of neonatal risk compared to caesarean section.
Keywords: breech presentation; delivery; obstetric; cesarean section
Introduction
Breech presentation is defined as a fetus in longitudinal lie with the buttocks or feet closest to the cervix at term. This presentation occurs in 3 to 4% of pregnancies. It is the most common presentation after vertex presentation [1]. Compared to the vertex presentation, breech delivery is considered dangerous because of the higher rates of perinatal mortality and morbidity attached to it. Indeed, some complications are more numerous or specific to the breech presentation. This reputation of eutocic presentation on the verge of dystocia has over the years led to an unresolved debate about the choice of the delivery route: vaginal or caesarean section [2]. Our work consists of a retrospective study that involved 194 deliveries at our hospital. Our objective is to study the different etiological factors, the elements of choice of the delivery route as well as the maternal and fetal prognosis of the two delivery routes. We will try through this work to evaluate the practice.
Material and Methods
A retrospective study was conducted in the Gynecology and Obstetrics Department of ibn Jazzer Hospital in Kairouan, over a period of one year from January 1st 2023 to December 31, 2023. During this period, there were 9281 deliveries in the department, all the breech deliveries of singleton pregnancies on term over or equal to 37 weeks of gestation were include. The non-inclusion criteria were Twin pregnancies with one or both of the twins with breech presentation, fetal deaths in utero, preterm birth and medical interruption of pregnancy. Data was collected from the medical files using a structured questionnaire including items concerning the history of the parturient, the characteristics of the pregnancy, the labour, the delivery and the findings of the new born examination.
Results
A total of 194 cases were collected representing 2.09% of all the deliveries. The mean age of the parturient was 29 years old, ranging from 18 to 44 years. Women aged over 36 represented 17% of the total number of deliveries. Overall, 53.1% of the women were primiparous and 4.6% had parity over five. Pregnancy-related related illness such as pre-eclampsia/ eclampsia or gestational diabetes was found among 8.7% of our participants. Unfortunately, 95.2% of the breech presentations were discovered at full term. Out of the 21 parturient (38.1%) with uterine scarring, 20 had cesarean sections and only one of them gave birth vaginally (she presented to the department during labor, fully dilated). The average gestational age at the admission was 39SA + 2days. Late and post- term pregnancies represented 18.2% and 7 patients could not specify the exact term of their pregnancy.
Cervical dilatation at admission was appreciated in 188 women, 36 parturient (18.6%) did not have a dilated cervix on admission and 11 women (5.7%) were admitted with full dilatation. The type of breech delivery was noted in only 105 cases (it was not specified in 15.5% of vaginal deliveries and 69.1% of caesarean sections), and was incomplete breech in 77.1% and complete in 22.9%. There were no footling or kneeling presentations. The most frequently encountered variety (44.4%) was the left anterior sacroiliac. An incomplete breech position was noted in of 53.1percentage cases among primiparous and complete breech position in 62.5percentage of cases. In total; 43.3percentage vaginal deliveries were noted in 43.3percentage of cases VS 56.7percentage caesarean sections. A vaginal attempt was possible in 57.7percentage of cases among which 75percentage were delivered vaginally. A scheduled caesarean section was indicated in 42.3percentage of cases (Figure1).
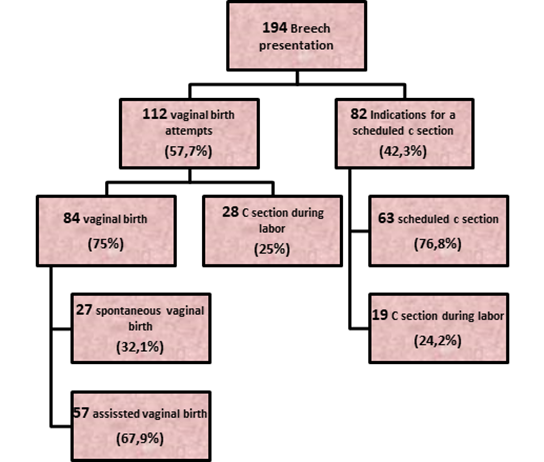
Figure 1: Delivery Methods for Women with Breech Presentation in Our Hospital During 2017.
A statistically significant association was found between cervical dilatation and delivery way. Indeed, 62.7% of women with cervical dilatation of less than 4 cm were delivered by caesarean section while 80%of those with cervical dilatation of more than 4 cm delivered vaginally (p = 0.0001). Despite that the caesarean section was the most common mode of delivery for primiparous women (60.2%), no statistically difference was found between the two delivery routes among primiparous and multiparous women (p = 0.08). Overall, 41.7% of complete breech presentations were delivered by caesarean section. The difference in delivery route between complete breech and incomplete breech was not statistically significant (p greaterthan 0.05). Once vaginal delivery was established, the incomplete breech was more likely to result in a vaginal birth than a complete breech (85.1% versus 63.6%) p = 0.03.
Bishop's score was appreciated in 173 cases. A statistical relationship was found between Bishop Score and the delivery way in favor of vaginal delivery. In fact, 70% of women with bishop score ≥ 6 gave birth virginally VS 67.3% with Bishop score lessthan 6, delivered by caesarean section (p = 0.0001). Within the established vaginal delivery group, a low Bishop score at the start of labour resulted in a cesarean delivery (p = 0.028). The biparietal diameter ranged between 82 and 106 mm, with an average of 94.14 mm. A biparietal diameter of more than 98 mm was statistically favorable for caesarean delivery (p = 0.007). All fetuses with BIP≥100 mm was delivered by caesarean section. The fetal weight estimated on ultrasound ranged between 1700 and 4600 g. overall, 16.8% of the fetuses had an estimated fetal weight greater or equal to 3800g. fetuses with an estimated fetal weight of less than 3800g were delivered by caesarean section in 53.5% of cases and 86.2% for fetuses with an estimated fetal weight greater or equal to 3800g (p = 0.001).
The estimated risk of caesarean section was 5.4 times higher with fetal macrosomia (OR = 5.4). The most frequent maneuvers found were a combination of the Lovset maneuver and the Bracht maneuver (57.1%). The medical team opted for abstention in 32.1% of vaginal deliveries. The most frequently reported indication of Caesarean sections in our study was the arrest of the dilatation (19.1%), macrosomic fetuses (14.55%) and other indications such as presence of a vaginal septum, umbilical cord prolapse, intra uterine growth retardation, placenta praevialate term or well as post-term with a contra indication to induction (15.45%). The sex ratio for new born with breech presentations was 1.12. The fetal weight estimated on ultrasound ranged between 1700 and 4600 g. overall, 16.8% of the fetuses had an estimated fetal weight greater or equal to 3800g. fetuses with an estimated fetal weight of less than 3800g were delivered by caesarean section in 53.5% of cases and 86,2% for fetuses with an estimated fetal weight greater or equal to 3800g (p = 0.001).
There was no statistically significant correlation (p greaterthan 0.05) between the sex of the newborn and the delivery route.37.3% of new born in our study weighed between 3000 and 3499 grams and 19.1% were macrosoms (weight≥3800). The estimated risk of caesarean section was 5.4 times higher with fetal macrosomia (OR = 5.4). For newborn macrosomes, there was a statistically significant difference (p = 0.003) in favour of caesarean delivery. Overall, 97,2% of new borns had an Apgar score of 10. Out of 194 births of fetuses with breech presentation, only one case of obstetrical trauma was found: a paralysis of the upper limb following a vaginal delivery without manoeuvers. This new born did not require a transfer to the intensive care unit. We did not find any cases of limb fracture or genital haematoma. Six newborns (3.1%) had to be transferred urgently to a neonatal intensive care unit: four cases were delivered vaginally. Among them, the medical team used Lovset and Bracht manoeuvers in 3 cases, and in one case only Lovset and Mauriceau manoeuvers. Our study includes a single case of neonatal death (0.6%). It was a vaginal delivery using the manoeuvers of Lovset and Bracht.
Discussion
Breech presentation is the most frequent presentation after vertex estimated 3 to 4% of all presentations [3]. Among all births in France; 4.8% are of breech presentation at the time of delivery. In our study the frequency was 2.09%.
This percentage varies mainly with gestational age. The average gestational age of our series was 39 SA + 2 days. The percentage of late and post term pregnancies in our study are 18.2%; this rate is 16.93% for the general population [3]. Never the less this difference is not significant (p>0.05). The distribution of women by age in the general population shows a very marked predominance of the age group between 20 and 35 years: 81.5% those results are similar to those found in a study conducted in 2008 at the University Hospital Center of Besancon had a patient population aged less than 30 years old [3,4]. This is similar to our patient population (average age of 29).
According to the literature, primiparous women represent approximately half of parturients who have given birth to a fetus at breech presentation. In our study, primiparous women represented 53.1% of women. This difference with the general population is statistically significant (p lessthan 0.001).
The complete breech has a bad reputation because of the frequency of complications during labor such as preterm rupture of the membranes, the risks of umbilical cord prolapse and the potential outcomes of a lower limb due to incomplete cervical dilation. The frank breech has a better prognos is mechanically because it achieves a better dilator cone [5]. According to the PREMODA study series, there was a statistically significant difference in delivery route between the two types of breech presentations (p = 0.002) [6]. In our study, this difference was not significant (p>0.05). According to a study conducted at the University Hospital Center of Besançon (2005), it has been shown, contrary to what is described in the literature, that there is no disadvantage of vaginal delivery of a complete breech compared to a frank breech since there is a rigorous selection of candidates for the vaginal delivery [7]. In our study; 64.9% of women with a breech presentation fetus presented to the hospital in spontaneous vaginal labour.
The Vermelin method is used in 32.1% of vaginal deliveries in our study. In the Chaibi A. et al and Ben Moussa I. et al series, the Lovset method accounted for 40% and 25.69%, respectively, of vaginal deliveries [3,8]. This maneuver was used alone in our study in 1.2% of cases but was often associated with the Bracht manoeuver (57.1% of vaginal deliveries). In our study Bracht's maneuver was used alone in 8.3% of vaginal deliveries; this was associated with the Lovset maneuver in 57.1% of cases. The combination of these two maneuvers is also the most represented in the series of Ben Moussa I. (40.97%) and Chaibi A. (53.3%) [3,8]. In our study, we used the Mauriceau manoeuver in only one case; the Lovset's maneouver was also used in this case. According to a study by Descargues G, only the Mauriceau Maneuver is significantly found more frequently in the complete breech [9]. During the natural delivery of a fetus in the breech presentation, soft tissue lesions are common: tearing of the cervix, bladder or rectum, secondary to abrupt extractions and in the rare case where, during the delivery of a complete breech, one of the feet is externalized through the recto-vaginal septum and the anus [8].
In this series none of these complications was found among parturients who gave birth vaginally. A study published by the team of the Term Breech Trial, at three months postpartum follow-up of the mothers of the same series, there was a statistically significant difference in women reporting pain in the genital area after a vaginal delivery (5,5%) compared to a caesarean section (1,8%); p lessthan 0.001. In addition, there was no greater risk of urinary incontinence in women who gave birth vaginally than those who delivered by caesarean section (p = 0.09) [10]. A study conducted in a French maternity level III, published in 2008, the analysis of Apgar scores at 1.5 and 10 minutes of life and transfers in neonatology did not show any significant difference between the attempted vaginal group and the scheduled caesarean section group [11]. There was no significant excess of fetal morbidity and mortality between the vaginal delivery group and the caesarean section. Similarly, the Franco-Belgian PREMODA study has shown that provided the use of the acceptability of the vaginal birth criteria, the selection of a vaginal delivery was not accompanied by an increase in the risk of vaginal neonatal complications [12]. Only one case of obstetric trauma was noted out of 194 (paralysis of an upper limb), with a frequency of 0.51%. In the AUDIPOG study, 9 children had traumatic injuries after delivery, including 8 in the accepted vaginal birth group (cranio-facial trauma, brachial plexus palsy and other lesions) [13].
Conclusion
Our study shows that when the selection criteria is well respected and the monitoring of labour progresses rigorous, vaginal delivery does not constitute a significant excess of neonatal risk compared to caesarean section. The vaginal delivery should be accepted each time the criteria are met. It is certain that if these recommendations are well implemented, neonatal outcome can be improved without increasing the rate of caesarean sections which can affect the maternal prognosis.
What is Already Know on This Topic
Breech presentation is the most common presentation after vertex presentation. It is considered as a dangerous presentation because of the attached higher rates of perinatal mortality and morbidity. Delivery route recommendations are still controversial based on a bundle of criteria.
Declarations
Competing Interests
The authors declare no competing interest.
Authors’ Contributions
Conception and Design of Study: Nadia Marouen, Aidi Hadhemi, Tarhouni KHouloud Slah Soui. Acquisition of Data: Nadia Marouen, Amrou Dinari, Slah Soui. Analysis And/or Interpretation of Data: Nadia Marouen, Hadhemi Aidi, Amrou Dinari. Drafting the Manuscript: Nadia Marouen, Aidi Hadhemi, Tarhouni KHouloud Slah Soui. Revising the Manuscript for Important Intellectual Content: Marwen Nadia, Amrou Dinari.
Acknowledgements
No Acknowledgements to declare.
References
- Goffinet F, Carayol M, Foidart J-M, Alexander S, Uzan S, et al. (2006). Is Planned Vaginal Delivery for Breech Presentation at Term Still an Option? Results Of an Observational Prospective Survey in France and Belgium. American Journal of Obstetrics and Gynecology. 194:1002-1011.
Publisher | Google Scholor - Vendittelli F, Riviere O, Pons J-C, Mamelle N. (2002). Breech Presentation at Term: Evolution of Practices in France and Analysis of Neonatal Outcomes According to Obstetric Practices, Based on The Audipog Sentinel Network. J Gynécol Obstét Biol Reprod. 31:261-272.
Publisher | Google Scholor - Boudhraa Kh, Jellouli Ma, Trabelsi A, Triki A, Ouerhani R, et al. (2009). Breech Presentation: A Retrospective Study About 137 Cases. La Lettre du Gynécologue. 346:33-37.
Publisher | Google Scholor - Ross S, Hannah M, Committee TBTS. (2006). Interpretation of the Term Breech Trial Findings. American Journal of Obstetrics & Gynecology. 195:1873.
Publisher | Google Scholor - Mattuizzi A. (2020). Breech Presentation: CNGOF Clinical Practice Recommendations - Epidemiology, Risk Factors and Complications. Gynecology Obstetrics Fertility & Senology. 48:70-80.
Publisher | Google Scholor - Roman H, Carayol M, Watier L, Le Ray C, Breart G, et al. (2008). Planned Vaginal Delivery of Fetuses in Breech Presentation at Term: Prenatal Determinants Predicting of Elevated Risk of Cesarean Delivery During Labor. Eur J Obstet Gynecol Reprod Biol. 138(1):14-22.
Publisher | Google Scholor - Broche D-E, Riethmuller D, Vidal C, Sautière J-L, Schaal J-P, et al. (2005). Obstetric and Neonatal Prognosis of a Poorly Known Podalic Presentation: The Complete Breech. Journal Of Gynecology Obstetrics and Reproductive Biology. 34:781-788.
Publisher | Google Scholor - Breton A, Gueudry P, Branger B, Le Baccon F-A, Thubert T, et al. (2018). Comparison of The Obstetric Prognosis of Attempted Breech Delivery: Spontaneous Versus Induced Labor. Gynecology Obstetrics Fertility & Senology. 46:632-638.
Publisher | Google Scholor - Descargues G, Doucet S, Mauger-Tinlot F, Gravier A, Lemoine J-P, et al. (2001). Influence of the Mode of Presentation in Breech Delivery in Selected Term Primiparas. J Gynécol Obstét Biol Reprod. 30:664-673.
Publisher | Google Scholor - Hannah ME, Hannah WJ, Hodnett ED, et al. (2002). Outcomes at 3 Months After Planned Cesarean vs Planned Vaginal Delivery for Breech Presentation at Term: The International Randomized Term Breech Trial. JAMA. 287(14):1822-1831.
Publisher | Google Scholor - Delotte J, Trastour C, Bafghi A, Boucoiran I, D’angelo L, et al. (2008). Influence of The Delivery Route in Breech Presentation at Term on The Apgar Score and Neonatology Transfers: Results of The Management Of 568 Singleton Pregnancies in A French Level III Maternity Hospital. Journal Of Gynecology Obstetrics and Reproductive Biology. 37:149-153.
Publisher | Google Scholor - Michel S, Drain A, Closset E, Deruelle P, Subtil D. (2009). Evaluation of Delivery Route Decision Protocols in Breech Presentation In 19 University Hospitals in France. Journal Of Gynecology Obstetrics and Reproductive Biology. 38:411-420.
Publisher | Google Scholor - Broche D-E, Ramanah R, Collin A, Mangin M, Vidal C, et al. (2008). Breech Presentation at Term: Predictive Factors for Cesarean Section During Labor. Journal Of Obstetrics and Gynecology and Reproductive Biology. 37:483-492.
Publisher | Google Scholor













