

Review Article
Bilateral Cleft Palate Appliance
Department of Medical Boarded of Orthodontics, St Kitts-Nevis.
*Corresponding Author: Mhd Azhar Ibrahim Kharsa,Department of Medical Boarded of Orthodontics, St Kitts-Nevis.
Citation: M.A.I. Kharsa. (2024). Bilateral Cleft Palate Appliance. Dentistry and Oral Health Care, BioRes Scientia Publishers 3(3):1-4. DOI: 10.59657/2993-0863.brs.24.033
Copyright: © 2024 Mhd Azhar Ibrahim Kharsa, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: March 28, 2024 | Accepted: April 15, 2024 | Published: May 17, 2024
Abstract
In this article, the author is trying to describe an approach for treating the “bilateral cleft palate” newborn patients, by a simple removable appliance, BCP “Bilateral Cleft Palate” Appliance. The appliance is a removable acrylic plane, with Y shaped three sectors, an expander “works as an intraoral retractor to retract the prognathism” and a “filament” or string for appliance withdrawal and removal when required. This appliance is indicated for newborn bilateral cleft palate patients, especially during the first days of extra uterus life when infant patient suffers difficulties in nursing and feeding because of the cleft palate effects, nasopalatine fistula, and when requirements are existed to retract the anteriorly protruded prognathism, as well. The action of this appliance is orthopedic as it works to retract the prognathism by activation of the “opened central expander” that works herein as in fact a “retractor and contractor”.
Keywords: bilateral cleft palate; prognathism; newborn patients; bcp appliance
Introduction
Patients with bilateral palate clefting often have maxillary evolution disorders and hypoplasia. The first step in such pitfall cases is to start treating the patient orthopedically since the first month of patient’s extra uterus life.The dilemma is that orthodontist has to do his uttermost best to retract the prognathism whereas patient is unable to be cooperative and difficulties in patient’s feeding and nurturing are in their utmost climax especially when nasal-palatine fistula exists (Figure 1).Even after cleft repair and orthodontic treatment, a severe maxillary deficiency may persist. However, the more treatment is early, the more complications are less.
Discussion
The BCP “Bilateral Cleft Palate” patients traditionally undergo repair with surgical approaches. These approaches may fail because:
1- Palatal scarring,
2- Soft tissue memory,
3- Scar formation.
Orthopedic traction leads to slow retraction of the surrounding tissues, allowing the body to accommodate the new position of the maxilla (Krimmel et al), what may enhance the circumstances of orthopedic and surgical procedure of the patient during his next years of growth.
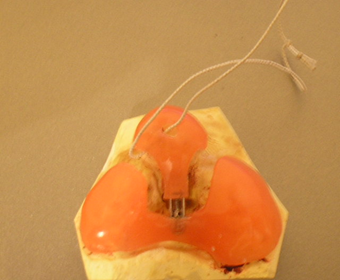
Figure 2: BCP Appliance for prognathism retraction.
BCP Appliance
The BCP Appliance (Bilateral Cleft Palate Appliance) may act as an initial treatment (Figure 2). The appliance consists of a retractor (counter-expander) in a center of an acrylic plane, split to three sectors Y-shaped. By activation of the Central “Counter-Expander” of this appliance, the anterior portion of the appliance is drawn back, enforcing the prognathism to follow, consequently this mechanism works as an orthopedic therapy in such patients, whereas the acrylic plane in the base of this appliance ensures the blocking of the nasopalatine fistula in case of existence, as well. The appliance is activated by following the “Vector” of arrow existed at the center of this appliance (Figure3). By such activation, the anterior portion of this appliance turns back gradually.

Figure 3: Activation of BCP Appliance, the left photo shows the appliance before its activation, whereas the right one shows it after activation. Notice the “posterior-traction” of the anterior part of the appliance in the right photo, after the activation.

Figure 4: BCP Appliance “The internal projection”.
The activation average is ¼ rounds per 72 hours, what insures regular prognathism traction of almost 2mm. per month. It is recommended that appliance be glossed, buffed and smooth from its outside and inside to evade and shun off any traumatic potential effect onto the infant (Figure 4). The string and filament also enable the patient’s parents to remove and withdraw the appliance simply (Figure 5).
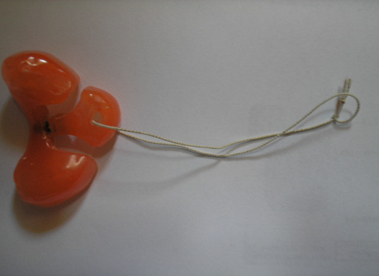
Figure 5: BCP Appliance has a filament that facilitates its withdrawal outside of infant’s mouth.
Conclusion
This appliance is a simple initiative treatment of bilateral cleft palate newborn patients. Such cases are really challenging to orthodontist, orthopedist and maxillo-facial surgeon as well. However, it is recommended that each case be studied, treated and approached as a unique entity per se. In other words, such an appliance is NOT an “antidote” for all bilateral cleft palate cases, as practitioner is advised to take into account case severity, patient’s age, existence of systemic diseases or syndromes and patient’s parents’ cooperation and comprehension. In addition to that, the average of activation should be studied for each case separately, discussed with the whole team of orthodontists, orthopedists and maxillo-facial surgeons. Finally, the cases of cleft lip and palates need an integrated teamwork to provide the best therapy for patients.
References
- Bell WH. (1992). Modern Practice in Orthognathic and Reconstructive Surgery. Philadelphia: WB Saunders Co.
Publisher | Google Scholor - Graber TM, Vanarsdall RL. (2000). Orthodontics: Current Principles and Techniques. Year Book Medical Pub.
Publisher | Google Scholor - Epker BN, Stella JP, Fish LC. (1998). Dentofacial Deformities: Integrated Orthodontic & Surgical Correction. Year Book Medical Pub.
Publisher | Google Scholor - Handelman CS. ((1996). The anterior alveolus: its importance in limiting orthodontic treatment and its influence on the occurrence of iatrogenic sequelae. Angle Orthod, 66:95-110.
Publisher | Google Scholor - Proffit WR. (1996). Contemporary Orthodontics. 2nd ed. St Louis, MO: CV Mosby, 2-16.
Publisher | Google Scholor - Subtlety JD. (1961). The soft tissue profile, growth and treatment changes. Angle Orthod, 31:105-122.
Publisher | Google Scholor














